
Abstract
PURPOSE:
To determine if people who walked with a lower limb prosthesis on discharge from rehabilitation continued to 20 weeks after discharge.
MATERIALS AND METHODS:
An observational cohort study design. People with major lower extremity amputation (LEA) who were discharged from rehabilitation using a prosthesis to walk and were due for prosthetic review appointment (20 weeks following discharge) during the period of data collection were eligible to be included. The primary outcome was the continuation of walking with a lower limb prosthesis at this time point (T2). Secondary outcome measures were: Timed Up and Go (TUG), Two Minute Walk Test (2MWT), SIGAM score, Locomotor Capability Index-5 (LCI-5), and Orthotic Prosthetic User Survey- Quality of Life (OPUS-QOL). Secondary outcomes were assessed at time of discharge from rehabilitation (T1) and repeated at T2. Statistical analysis was carried out comparing the results of the secondary outcome measures at T1 and T2.
RESULTS:
22/28 participants were still walking with their prostheses at T2. Five of the six who abandoned walking with their prostheses did so because of issues with the skin on their residuum or contralateral foot. Participants who continued to walk with their prostheses demonstrated a statistically significant improvement in TUG (5.01 seconds, p < 0.01) and 2MWT (11.35 metres, p < 0.01) between the two time points. No statistically significant difference was found in LCI-5 or OPUS QOL scores between the two time points.
CONCLUSION:
Most participants continued to walk with their prosthesis and experienced further improvements in their exercise tolerance and decrease in their risk of falls after discharge.
Introduction
There are approximately 4,000 people living in Ireland with lower limb absence and prosthetic needs and an incidence of 500 people per year with primary limb loss [1]. This is anticipated to rise as a result of increasing incidence of diabetes and an aging population [2]. Diabetes is thought to account for an estimated 53.5% of amputations that occur in Ireland each year [3]. While up to date information on trends of amputation rates in Ireland are not available, the most recent rates were 175.7 per 100,000 in 2009, an increase from 144.2 per 100,000 in 2005 [3].
Prosthetic services in Ireland are primarily provided through the National Rehabilitation Hospital, with services also available in other settings around the country. Not all patients undergoing an amputation are suitable for prosthetic rehabilitation and this decision is based on an interdisciplinary team assessment considering evidence-based factors [4]. Current practice at the Irish national prosthetic rehabilitation unit is that a patient is discharged from prosthetic rehabilitation and receives ongoing follow up throughout their lifetime from the national prosthetic service for prosthetic adjustments and maintenance. They are not routinely followed up by other members of the interdisciplinary team and no information is gathered on whether patients continue with prosthetic use in their own environment after discharge. It is not known if the outcomes achieved during prosthetic rehabilitation are maintained after discharge.
The overall aim of prosthetic rehabilitation is to return people to their own environment and to enable them to accomplish usual life habits whilst wearing a prosthesis as independently as possible [5]. The most frequently reported patient goal of prosthetic rehabilitation is to walk with a prosthesis [6]. This is associated with a large cost both in terms of prosthetic componentry and therapeutic input. While no figures are available in the Irish context, the estimated lifetime prosthetic cost for a lower limb amputee in the USA ranges between $0.5–$1.8 million dollars depending on the number and type of prosthesis [7]. The feasibility of maintaining daily prosthetic use post discharge may be challenging secondary to the increased energy expenditure associated with walking with a prosthesis [8]. Critical limb ischaemia is the most common cause of lower extremity amputation (LEA) and is associated with significant medical co-morbidities including peripheral vascular disease, hypertension and diabetes [4]. It is likely that the disease has widespread manifestations by the time it has progressed to requiring amputation and may cause other symptoms including decreased exercise tolerance and fatigue that will further impact on mobility.
Despite the high cost of prosthetic provision and rehabilitation input, evidence from other countries suggests that prosthetic use is frequently abandoned by LEAs post discharge [9, 10]. A seven-year follow up study of 151 vascular patients discharged from a prosthetic centre, found that only 54 continued to use their prosthesis at follow-up [9]. No definition was provided in this study of the criteria for maintaining use of prosthesis in terms of frequency or duration of wearing prosthesis. A shorter follow up time of one year was used in a study in Sheffield which included 281 patients [11]. After one year 66% of transtibial and 50% of transfemoral amputees were household ambulators and 54% of transtibial and 29% of transfemoral amputees were community ambulators. No information was given on the initial levels of mobility at time of discharge from the prosthetic rehabilitation making it difficult to determine if this differed from the initial rehabilitation outcomes. The study used the Stanmore Harold Wood outcome measure of mobility, a measure that is no longer routinely used [12]. Another one year follow up of 75 participants found a similar results; 54% of transtibial and 45% of transfemoral amputees were mobilising with a prosthesis one-year post amputation [10]. They divided patients into categories of outcomes of two extremes; wheelchair/ bedbound or mobilising independently with or without a walking stick. This did not account for therapeutic walkers walking with supervision or those who may have used other walking aids e.g. a walking frame.
Few studies have assessed the maintenance of specific rehabilitation outcome measures post discharge. A small study comprising of 13 participants used a mixed method design to follow up amputee patients three months and six months post discharge from rehabilitation [13]. Functional performance was measured using the 2-minute walk test (2MWT) and L-test, along with qualitative interviews to explore the patients’ perceptions and experiences of factors affecting their functioning. Four of the nine participants declined in walking distance in the 2MWT either at the three- or six-month time point and the other five were unable to walk and therefore unable to complete the functional performance measures. The perceived limitations reported by participants were in autonomy outdoors and family role domains. There was not a correlation between decline in physical function and changes in perceived participation and autonomy.
While these studies have looked at maintaining prosthetic outcomes they have been in countries where the settings and services for this population may be quite different. For the most part they have looked at maintaining or not maintaining walking over longer periods and have rarely considered specific outcome measures. To the authors’ knowledge no study has investigated this in the Irish setting and over the period of adjustment initially following discharge. Measuring outcomes across all domains of the ICF will provide more detailed information as to how people with LEA management over this period. Therefore, the aim of this study was to determine if people with LEA continue to walk with their prosthesis initially after discharge from specialist inpatient prosthetic rehabilitation services.
Method
Study design and participants
This is a prospective cohort observational study. Rehabilitation outcomes measured at the time of discharge from inpatient rehabilitation (T1) were repeated at a follow-up appointment 20 weeks after discharge (T2) at the same time as a routinely scheduled prosthetic review appointment. A consecutive sample of convenience was used. All patients with major LEA, who were discharged from inpatient rehabilitation and due for 20 week prosthetic review during the period of data collection between September 2019 and February 2020, were invited to participate. Inclusion criteria were 1) major LEA, of any cause and 2) ambulatory with a prosthesis at time of discharge. Exclusion criteria were patients who were not using a prosthesis to mobilise on discharge. Major LEA is defined as an amputation at the level of the ankle or above [14].
Ethical considerations
Ethical approval was granted by the institutional ethics committee where the study took place prior to study commencement.
Procedure
Eligible participants were sent an information leaflet by post and invited to take part. Informed consent was obtained. Demographic information including the participant’s age, sex and factors previously found to be predictive of mobility including level of amputation, co-morbidities and cognition was extracted from the healthcare record. Outcome measure results recorded at T1 by the treating physiotherapist were extracted from the participants’ healthcare record.
Data was collected by a research physiotherapist through face-to-face interview and physical assessment in an outpatient setting 20 weeks following discharge. Questions included whether the participant was still walking with their prosthesis daily, the distance and aid they typically used. Continuing to walk with a prosthesis was defined as participants reporting using their prosthesis for a minimum of one hour daily. Participants were asked if they received follow up physiotherapy and the number of sessions. Outcome measures completed on discharge were then repeated after the prosthetic appointment (T2); Special Interest Group in Amputee Medicine (SIGAM), Timed Up and Go (TUG), 2-Minute Walk Test (2MWT) and Locomotor Capability Index-5 (LCI-5). The Orthotic Prosthetic User Survey- Quality of Life (OPUS-QOL) was also completed.
The TUG asks the participant to stand up from a standard height chair (seat height 46cm, with arms), walk at a self-selected comfortable speed for 3 metres, turn around and sit back into the chair [15]. The 2MWT is a measure of functional exercise capacity that assesses the distance a patient can walk over two minutes using a mobility aid of choice [16]. The SIGAM describes six clinically meaningful functional levels (A-F) of walking ability wearing a prosthesis [17]. The participant is assigned a level based on the assistance they require, distance they can walk and mobility aid used. The LCI-5 is a 14-item questionnaire designed for lower limb amputees about self-reported ability to complete functional tasks wearing a prosthesis [18]. A quality of life measure (OPUS QOL) was completed at T2 once the participant had an opportunity to experience the impact of their amputation in their normal lives [19].
Analysis
The primary outcome of this study was the proportion of participants who continued to walk with their prosthesis 20 weeks after discharge. This was calculated as a percentage.
Paired t-tests were used to compare the outcome measure scores at T1 and T2 for normally distributed interval/ ratio data (based on a Shapiro-Wilk test) and Wilcoxon Signed Rank test for ordinal data. It was estimated that 13 continued ambulators would be required to detect a meaningful change of 4 seconds in the Timed Up and Go test assuming a standard deviation of 6.9 seconds based on previous literature [20] (Sample Size Calculator, Maple Tech International). Statistical analysis was completed using IBM SPSS Statistics 26 for Windows.
Results
Participants
Sixty patients were discharged from prosthetic rehabilitation and due for review during the period of data collection. Forty-five of these patients met the inclusion criteria. Twenty-eight participants consented and were included in the study. Figure 1 outlines the reasons for eligible participants not being included in the study. The main reasons were patients having their prosthetic review remotely in satellite clinics (7), not attending review appointments (3) and deceased (3).
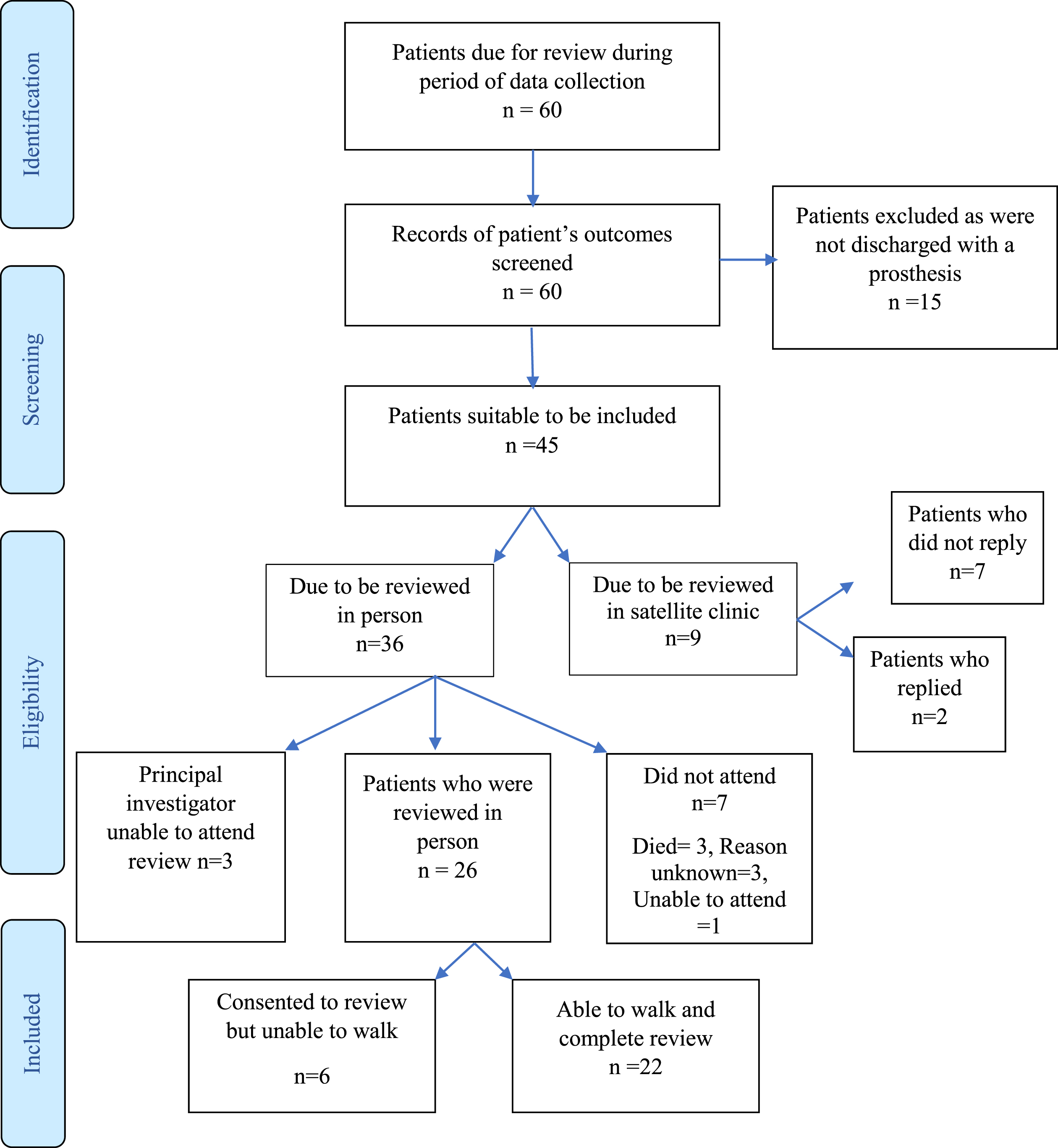
Participants flow diagram.
Addressing the primary research aim, 22/28 (78.6 % (95% CI: 59.1% to 91.7%)) of participants maintained walking 20 weeks following discharge. 6/28 (21.4%) of participants did not maintain walking with their prosthesis at the time of review. Skin breakdown on the residuum or contralateral foot, further amputation and back pain were the reasons given by participants for no longer walking with a prosthesis. Table 1 details the differences in participant demographics in those walking versus not walking at time of review (T2).
Participants demographics and presentation categorised by review mobility status
For those who continued to walk with their prosthesis at T2 there was a mean improvement in TUG score of 5.0s, a mean improvement in 2MWT distance of 11.4m and a mean increase in LCI-5 score of 3.6 points. Not all datasets were complete due to outcome measures not fully being completed T1 or time constraints at T2. Statistical analysis was completed on samples with scores at both time points (Table 2). A statistically significant difference was found in TUG and 2MWT scores between the two time points. No statistically significant difference was found in LCI-5 scores between the T1 and T2.
Summary of results of outcome measure score at each time point and statistical analysis completed
Summary of results of outcome measure score at each time point and statistical analysis completed
aData available for 18 participants, bData available for 18 participants, cData available for 24 participants.

Distribution of SIGAM levels at T1 and T2. SIGAM levels: A- Not using prosthesis/ use for cosmesis only, B- transfers/ shorts distances with assistance, C- walks indoors less than 50m with an aid, D-walks outdoors greater than 50m with and aid, E-occasional walking aid use.
Review of the SIGAM scores at T1 and T2 showed that nine participants regressed, six participants improved and 13 participants stayed at the same SIGAM level between the time points. Six participant’s regressed in SIGAM level due to prosthetic limb abandonment, the reason for the regression in SIGAM score for the other 3 participants is unknown.
The mean OPUS QOL score overall was 70.6 (SD 17.6). There was no significant difference in the OPUS QOL for patients who were walking and those who were not walking at the time of prosthetic review appointment (mean OPUS QOL score for walkers: 70.6 (SD 15.2) and non-walkers: 70.4 (SD 27.4))
The results of this study found that walking with a prosthesis is maintained by only 78.6% of participants 20 weeks after discharge from specialist inpatient rehabilitation for limb loss in Ireland. There is a high rate of prosthetic limb abandonment of 21%.
While the rate of limb abandonment is less than in other studies (53%) with a similar proportion of participants with vascular problems, the time to follow up was much shorter [9]. Of the six people reviewed for whom walking was not maintained, the reasons included a wound on the residuum (2 participants), wound on the contralateral heel (1 participant), a subsequent amputation on the other leg (2 participants) and back pain (1 participant). This was not consistent with findings of other studies who found fear of falling, difficulty dressing and the weight of the prosthesis to be the main reasons [9].
Within the short time period from discharge to time of review 2/28 (7%) participants underwent a subsequent major amputation on the contralateral lower limb. This rate of contralateral limb amputation is not dissimilar to other studies however the time frame to further amputation in this study is shorter. A bilateral amputation can result in an increase in disability, depression and mortality [21] and increases the patients care needs. Abnormal loading of the contralateral limb during prosthetic walking and peripheral neuropathy as a result of type 2 diabetes may contribute towards the risk of skin breakdown to the contralateral foot [22]. The results highlight that, as issues with skin on the residuum or contralateral foot or skin breakdown leading to further amputation accounted for the majority of those no longer wearing their prosthesis, an emphasis needs to be placed on skin care management during rehabilitation.
For participants who continued to walk with their prosthesis, there is a statistically significant and clinically meaningful improvement in TUG scores between the two time points. The mean TUG at T1 indicated that participants were at increased risk of falls however their risk of falls was decreased at T2 based on the cut off score of 19 seconds in this population [20]. One factor that may have contributed to this might be exposure to more challenging balance scenarios in the home and community environment versus the inpatient rehabilitation setting.
The 2MWT has been found to strongly predict the six-minute walk test as a measure of endurance in this population [23]. There is a statistically significant increase in 2MWT scores and therefore exercise tolerance levels between the two time points however the change of 11m was clinically small. The change in walking distance using this measure was recorded however a change in walking aid used was not, which may have confounded the results as positive progress to using a less supportive aid could be associated with slower gait speed. The SIGAM scores indicate that six participants did move to a less supportive aid (this is categorised as a sub score a-c within SIGAM levels C and D).
For those who remained ambulant with their prosthesis at T2, the difference in LCI-5 score between T1 and T2, of 3.6 points was not statistically significant. For the average transtibial or transfemoral vascular amputee their premorbid level of function as per the LCI-5 score was found to be 47.1±12.3 points [24]. Based on these scores the activity level of participants in this sample at the end of rehabilitation (31 points) and time of review (34.5 points) is less than their perceived activity levels prior to amputation. This indicates that despite the positive change in gait speed at the impairment level, patients did not significantly improve their function and activity levels 20 weeks after discharge from prosthetic rehabilitation and were still less active than before their amputation.
No difference was found in QOL based on OPUS QOL score between those walking and not walking at T2. This differed from other studies in the same population that found mobility with a prosthesis to impact on a person with LEA QOL [25]. The ability to walk successfully with a prosthesis was found to have the greatest positive impact on QOL [26]. However other studies compared QOL in those who received a prosthesis and those who did not. In the current study all participants received a prosthesis and had an opportunity to use it in their own home. This may have increased participants insight into the challenges and difficulties of using a prosthesis and may have made not using a prosthesis easier to accept.
This study provides descriptive information on potential previously identified confounders that might contribute towards maintenance of ambulation with a prosthesis including family support, cognitive changes (MOCA) and further physiotherapy input after discharge [27] and it is important that these factors are considered when interpretating the results. Comparison of these factors between groups was limited by the small number of non-ambulators (6 participants). Furthermore not all previously identified factors such as smoking, BMI and length of time from amputation to rehabilitation which have been shown to impact on rehabilitation outcomes were taken into account [4]. Future studies with a larger sample size could explore these factors in more detail.
Limitations
There are several limitations to this study. A proportion of those eligible for the study were not included for reasons identified, thus impacting on the generalisability of the results. The sample size for an observational cohort study is small with only 28 participants reviewed, not all of whom had full datasets. This resulted in a very small sample of only six participants in the non-ambulatory group, limiting any analysis of the characteristics of the non-ambulators. Furthermore, the study was not powered for comparisons between ambulators and non-ambulators. Potential confounding factors were not adjusted for through multivariate analysis so their impact on the outcomes is unknown. Complete follow-up at T2 was limited to those who attended their review appointments at the centre were the study took place.
Conclusion
Ambulation with a prosthesis was maintained by most participants 20 weeks after discharge from prosthetic rehabilitation. Those who continued to walk with their prosthesis demonstrated further improvement in balance and endurance, compared to their performance at discharge. For the 21% who abandoned walking with a prosthesis within 20 weeks, skin breakdown was the most common reason associated with prosthetic abandonment. A review of the delivery of education on the management of skin and also on the implementation of self-management strategies for chronic conditions in this setting may help to ensure durability of prosthetic outcomes post discharge.
Implications for research
Prosthetic use is abandoned by one in five patients shortly after discharge from prosthetic rehabilitation. Skin breakdown on the residuum or the contralateral foot was reported to be the main barrier to continuing with prosthetic use.
Conflicts of interest
The author reports no conflict of interest.