
Abstract
INTRODUCTION:
Physiotherapists in Irish hospitals with critical care units deliver physiotherapy services 24 hours a day, seven days a week. There is a perceived lack of consistency in the level of clinical competence, required skills and content of training between hospitals, compounded by the absence of a national policy, procedure or clinical framework for physiotherapists working in critical care. The study aimed to identify the minimum standards of clinical practice expected of physiotherapists working in critical care settings in Ireland.
METHODS:
A modified Delphi technique was used to survey a panel of senior and clinical specialist physiotherapists working in critical care units in Ireland to obtain consensus of items. The questionnaire of 214 items was completed over three rounds. Items were determined ‘Essential/Not Essential/Unsure’ by participants. Items that did not reach consensus were included in the subsequent round with additional items suggested by participants.
RESULTS:
25/46(54%) physiotherapists completed the first round, with 17 and 13 completing round 2 and round 3 respectively. A total of 220 items were included, 120 of which were deemed essential for a minimum standards of independent clinical practice in Irish critical care units. Fifty-six items were considered not essential while consensus was not reached on 44 items.
CONCLUSIONS:
This study identified 120 items of knowledge and clinical skills considered essential as a minimum standard by physiotherapists working in Irish critical care units. Further discussion is required to determine how these results can be applied to guide clinical practice for physiotherapists working in critical care in Ireland.
Introduction
Critically ill patients are usually cared for in a High Dependency Unit (HDU) or Intensive Care Unit (ICU) [1]. Physiotherapists in Irish hospitals with critical care units deliver physiotherapy services 24 hours a day, seven days a week [1]. This is achieved by provision of physiotherapists working on call during evenings and weekends. On call working requires all physiotherapy staff to maintain a level of competence in the management of patients in critical care, irrespective of clinical specialty or primary area of practice [1, 2]. Competence to work in critical care is subjective to both the physiotherapist undertaking the training and their educator. Anecdotally, from the authors’ clinical experience and through peer discussion there is an understanding that both training to work in critical care and clinical practice may vary between hospitals. The perceived lack of consistency in the level of clinical competence, required skills and content of training between hospitals is compounded by the absence of a national policy, procedure or clinical framework for physiotherapists working in critical care. Previous research found clinically important differences in the treatment administered by the critical care physiotherapist compared with the on-call physiotherapists including duration of assessment, treatment selection and execution [3]. This indicates a need to standardise training.
Existing research suggests there is international interest in exploring the minimum clinical standards required of physiotherapists to work in critical care with studies conducted in Australia and New Zealand, the United Kingdom (UK), Japan and South Africa [4–7]. Skinner et al [4] used a modified Delphi technique to investigate the minimum standards of clinical practice expected of physiotherapists working in critical care in Australia and New Zealand. An expert panel of physiotherapists completed three rounds of questionnaires to identify the required clinical skills. Twose et al [5] and Takahashi et al [6] replicated the study investigating the clinical standards expected in the United Kingdom and Japan respectively. The study conducted in South Africa [7] investigated the minimum standards required for physiotherapists working in critical cares, adopting qualitative methodology completing focus group sessions with experienced physiotherapists, both clinicians and academics [8]. While the study conducted in South Africa [7] differed in design to the Australasian, UK and Japanese studies [4–6] all studies identified the need to develop national standards and clinical frameworks to support education and reduce variability in clinical practice.
The differences in health service provision, pre-registration physiotherapy education and post-graduate training make it difficult to apply the results of the previous studies to the Irish setting. Therefore the aim of this study was to identify the minimum standards of clinical practice expected of physiotherapists working in critical care settings in Ireland. The objectives of this study were to gain a professional consensus of the minimum standards of clinical practice for physiotherapists working in critical care in Ireland and to understand the clinical skills expected of a physiotherapist to work independently in a critical care setting in Ireland.
Methods
Ethical considerations
The study was reviewed and approved by the Nursing and Health Research Ethics Filter Committee, Ulster University and the Clinical Research Ethics Committee, Galway University Hospital. A participant information sheet was provided to participants outlining the purpose and methodology of the study. Informed consent was assumed by completion of the questionnaires in each round. All data collected was anonymised in adherence with Ulster University General Data Protection Regulation (GDPR) guidelines [9].
Research design
A modified Delphi technique was used in this study. The Delphi technique is a process used to establish a consensus by surveying a panel of experts through a series of questionnaires [10, 11]. The expert’s responses may change as survey rounds are completed based on the information provided by the other panellists thus, establishing a true consensus by the end of the process [11, 12]. For the purpose of this study the modified Delphi technique that was used in previous studies [4–6] was replicated for this study in order to be consistent and enable comparison of results later. A structured questionnaire of 214 items was used in the opening round with an open field for comments below each questionnaire item. This allowed for refinement of questionnaire items, the addition of new items and definitive consensus by the panel of experts.
Recruitment and participants
Senior and clinical specialist physiotherapists working in critical care were recruited to create the expert panel. All 26 public hospitals listed in the National Adult Critical Care Capacity and Activity Census [13] with critical care units in Ireland were contacted by telephone in order to identify potential participants to receive the recruitment email. Additional participants were identified through snowball recruitment. Eligibility for recruitment was based on the inclusion and exclusion criteria. Senior or clinical specialist physiotherapist predominantly working in critical care were included while physiotherapists working in higher education institutions, senior or clinical specialist physiotherapists not working in critical care, staff grade physiotherapists, physiotherapy assistants and physiotherapy students were excluded from the study. Recruitment was sought by an email including the participant information sheet. A pre-determined sample size was not determined to allow as many physiotherapists as possible participate [4, 12].
Questionnaire
The same survey design as the Australia and New Zealand, UK and Japanese research was used to allow for comparison of data [4–6]. Permission for use of the questionnaire was sought from Twose et al [5]. The questionnaire was reviewed to ensure the wording was appropriate for the Irish setting. Prior to commencing a pilot of the questionnaire and study procedure was completed with two senior physiotherapists that were not recruited to the study. Feedback was sought and no alterations were required. The survey questionnaire was developed with the intention of being as expansive as possible across the skills and knowledge required of a physiotherapist working in critical care [4]. The 214 questionnaire items were comprised of common critical care clinical conditions, physiotherapy assessments and treatments in a critical care setting. Participants were asked to grade each questionnaire item on the survey as “essential” for clinical practice, “not essential” for clinical practice or “unsure”. Participants were invited to submit additional items thought to be required for clinical practice in critical care in Ireland in Rounds 1 and 2. Suggested items were added to the subsequent rounds for consensus opinion from the panel.
Procedure
Three rounds of questionnaires were administered to participants. Each round of the questionnaires were completed within three weeks. Questionnaires were disseminated electronically via SurveyMonkeyTM (SurveyMonkey, Inc., San Mateo, CA, USA) [14], an online survey software package. Electronic reminders were sent to non-responders 1 and 2 weeks after the initial invite to encourage response. In the first round, demographic data was sought to characterise participants. Between each round, participants were sent a personalised report containing quantitative group results, qualitative feedback, and the participant’s own responses for comparison purposes.
Items were determined as essential or non-essential once consensus was reached. Consensus for the purpose of this study was defined as > 70%, in keeping with previous research [4–6] to allow for comparison of findings. When the threshold of > 70% consensus was reached, for either essential or non-essential, the item was removed from the successive rounds of questionnaires. Items where consensus was not reached were included in the subsequent round. Additional items suggested in Rounds 1 and 2 were cross-referenced against existing survey items, and were only included in following rounds when they did not duplicate an already administered item.
In keeping with the UK study [5], and to ensure the final consensus was not biased by ‘unsure’ responses, consensus was calculated using three potential denominators; 1. Total number of participants completing survey 2. Total number of responses excluding missing answers and 3. Total number of definite ‘essential’ or ‘not essential’ responses, excluding unsure responses. To be included as essential or not essential, consensus of 70% was required for all three calculations.
Analysis
Survey responses were downloaded from Survey Monkey™. Data analysis was primarily descriptive. Open comments were collated, themed by one researcher and anonymised for the purpose of the personalised reports. Data was exported from Survey Monkey™ and analysed using Microsoft Excel™. Data is presented as n=(%) unless otherwise specified.
Results
Participants
Of the physiotherapists who were invited to participate 54% (35/46) completed round 1 to create the survey panel. Round 2 was completed by 68% of participants (17/25) and 52% (13/25) completed round 3. Participants represented all seven hospital groups in Ireland and 1 private hospital (Table 1). They had an average of 15 years post graduate experience, with 13 years in critical care. Post graduate education to Masters level had been completed by 24% (6/25).
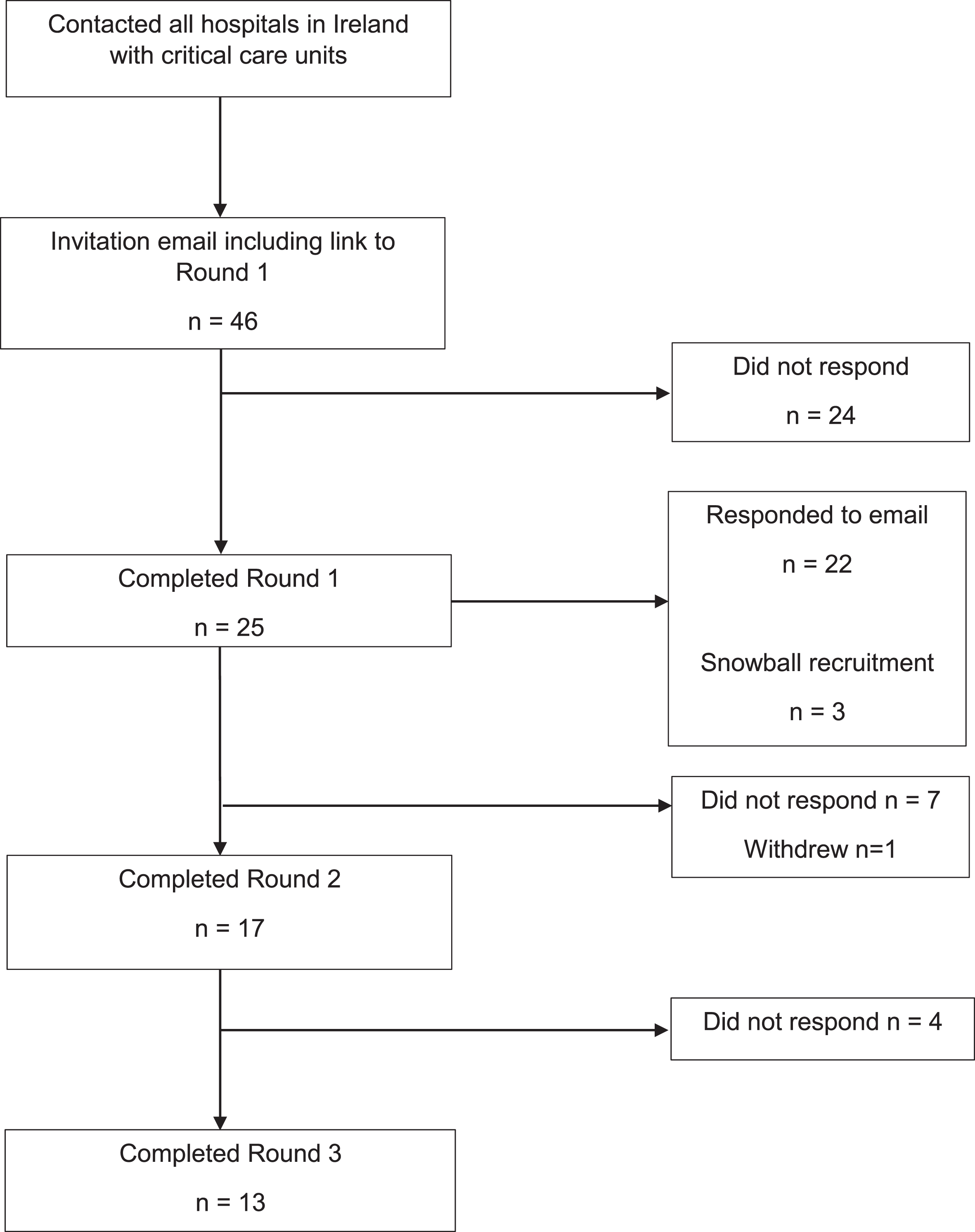
Panel selection and completion rates. Flow chart of participant involvement and completion rates. The flow diagram illustrates the recruitment of participants, their involvement through the three rounds of the survey and the completion through the rounds.
Demographic data for participants
Figure 2 shows the progress of items through the three rounds of the survey. Round 1 surveyed the participants on 214 items, of which consensus was not determined on 77 items. Round 2 consisted of these 77 items and an additional 5 items suggested by participants in round 1. Round 3 consisted of 50 items where consensus had not been reached and one additional item. Following the 3 rounds, 120 items were considered ‘Essential’ by the panel (Table 2), 56 ‘Not Essential’ (Table 3) and consensus was not be reached on 44 items. Table 4 shows the items where consensus was not reached as well as the percentage of participants who deemed the item ‘Essential’.
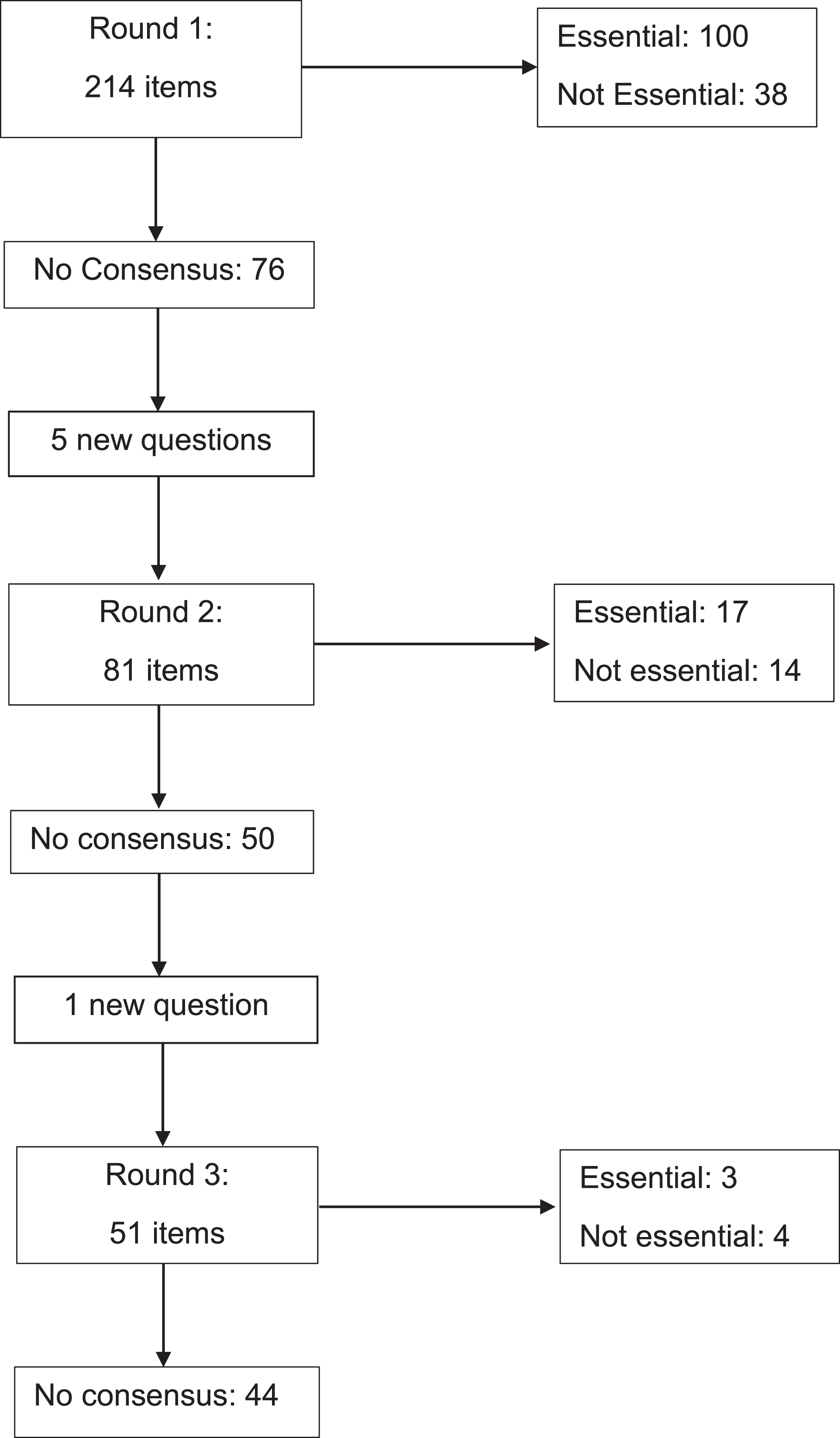
Inclusion and exclusion of questionnaire items. Flow chart of the inclusion and exclusion of questionnaire items. This flow diagram illustrates the number of items included in each questionnaire round, the number of items reaching consensus, the number that did not reach consensus and the number of items included based on suggestions from participants.
Items deemed ‘Essential’ (Consensus > 70%)
(* item added during subsequent round).
Items deemed ‘Not Essential’ (Consensus > 70%)
(* item added during subsequent round).
Items where consensus could not be reached
(* item added during subsequent round).
During the round 225 comments were made by participants regarding the questionnaire items. The comments were collated, anonymised and the content themed. The five most common themes are observed were “Basic understanding/recognition/awareness/interpretation” required (n = 65) “Item is specific to Unit/Hospital” (n = 58) “Not seen/used in practice” (n = 35) “Item (Assessment/Technique) is performed/lead by other members of the multi-disciplinary team” (n = 22) “Not essential for on call working” (n = 21). Additional comments were “As part of/ in collaboration with the multidisciplinary team” (n = 7) “Need to be aware local infection control procedures/implications” (n = 3) “Specialist skill” (n = 3) and “Infrequent use” (n = 2). It was acknowledged that “Imaging is reported” (n = 8) with regard to radiological imaging.
Discussion
There is an international interest in exploring the minimum clinical standards required for physiotherapists to work in critical care [4–7]. Currently in Ireland there is no national clinical framework for physiotherapists working in critical care. The aim of this study was to identify the minimum standards of clinical practice expected of physiotherapists working in critical care settings in Ireland. The findings provide the first step towards the development of a minimum standards informed framework for physiotherapists working in critical care settings in Ireland by identifying 120 essential items. The study participants had substantial critical care experience, all had delivered on call training within the last 3 years, and all seven hospital groups in Ireland were represented.
In accordance with previous research [5], three survey rounds were used to achieve final consensus. This was to ensure the final result would not be biased by ‘unsure’ responses or unanswered questions. The decision to use 70% as the criteria for consensus was based on previous studies [4–6]. A number of items came close to achieving essential or not essential consensus but did not meet 70% on all three calculations, and therefore were classed as not reaching consensus. The threshold of 70% was a potential limitation of the study. For example, ‘End Tidal Carbon Dioxide’, ‘Neutrophil Count’ and ‘An ability to perform a neurological examination of motor and sensory functions’ achieved 69% consensus in the third round and was determined as ‘consensus could not be reached’. Choosing a threshold is helpful for providing direction about the essential items. However as with this example, when consensus cannot be reached this result does not direct a definitive decision to exclude items from training.
It was anticipated that tertiary services, such as neurosurgery and extra-corpeal membrane oxygenation (ECMO), would be deemed not essential as these services are not commonly available in most critical care units in Ireland, yet most participants commented on the awareness of these as essential. Comments regarding these items did however explain these choices e.g. ‘Specific to Unit/Hospital’ or ‘Not seen/used in this hospital’. All comments that participants provided were categorised into themes. The most common theme was “Basic understanding/ recognition/ awareness/ interpretation required”. This demonstrated participants’ reluctance to determine an item either essential or not essential as for the most part, these comments occurred when a participant replied “unsure”. The theme of ‘performed/lead by other members of the multi-disciplinary team’ was observed with physiotherapists identifying the involvement of a Speech and Language therapist with respect to ‘swallow assessment’ and tracheostomy care, and an Occupational Therapist in splinting.
A number of other differences compared to the previous four studies have been identified. Australia/New Zealand [4] and UK [5] both determined manual hyperinflation (MHI) essential and could not reach consensus on ventilator hyperinflation (VHI), while the Irish study found the opposite. The risk of barotrauma with the use of MHI has been debated in the literature [15] and more recently, was discouraged in the early stage of the of the Covid-19 pandemic [16]. Additionally, the use of non-invasive ventilation (NIV) was determined essential by the Irish study but not essential or no consensus by the Australia/New Zealand, UK or Japanese studies. As six years have passed between the Australia/New Zealand and this study, changes in clinical practice in that time may account for some of the different outcomes. The Japanese study [6] found oxygen therapy, VHI, MHI, nasopharyngeal suctioning and oropharyngeal suctioning not essential as physiotherapists are not permitted to perform these interventions in Japan. This highlighted the international differences in clinical practice and the value of conducting this research in individual countries, in contrast there is more harmonisation that differences.
Limitations
It has been suggested that a response rate of 70% in each round is required to ensure rigor [17]. The study failed to reach the desired response rate despite incorporating strategies to optimise recruitment and retention including identifying at least one contact physiotherapist for each hospital prior to issuing the survey, issuing personalised reports, sending regular reminder emails and access to each round of the questionnaire was open for three weeks. However, the study was conducted during the Covid-19 pandemic (February 2021 –May 2021), in which physiotherapists working in critical care were burdened with significant demands, exhaustion and burnout [18]. Response fatigue may have been a factor [19] due to the length of the questionnaire (214 items in Round 1). The largest drop off in participants was observed from Round 1 to Round 2 [20]. The Delphi process requires continued commitment from participants to maintain involvement until the process is completed [12]. Increasing non response is common in panel surveys and decreased engagement can increase with subsequent rounds [21, 22]. Respondents may give less thoughtful answers or withdraw participation prior to completion of the study [23]. It was observed that fewer comments were received in the later rounds of this study.
Another limitation of the study design is the focus on the “technical competence” of the skill rather than the physiotherapists’ clinical reasoning of appropriateness and application of the skill; this was also acknowledged by Skinner et al [4]. Equally, they must recognise the limitations of their knowledge and practice and seek help when necessary. As experience informs practice, additional training or co-working with senior colleagues may prove beneficial in supporting practice and developing clinical reasoning [24].
Consideration is now required as to how the items identified as essential for clinical practice in this study could be used to inform critical care practice and education, and the development of competency standards for physiotherapists, similar to that of critical care nurses in the UK [25].
Conclusion
This study identified 120 items as essential for a minimum standard of independent clinical practice in critical care units in Ireland. Given the low response rate confirmation of these items and further research may be required before a standard of competency can be developed. The results of this study represent a starting point to inform further discussion and research towards standardising practice for physiotherapists working in critical care in Ireland.
Footnotes
Acknowledgments
The authors would like to thank Paul Twose for supporting this study and for sharing the questionnaire and research design. The authors would like to acknowledge Elizabeth H Skinner, Peter Thomas, Julie C Reeve and Shane Patman for the development of the original questionnaire. The authors would also like to thank all those who gave their time to complete the questionnaire surveys.
Conflict of interest
The authors declared no potential conflicts of interests.
Ethical considerations
Ethical approval for this study was provided by Ulster University Institute of Nursing and Health Research Filter Committee and Galway University Hospitals Clinical Research Ethics Committee (Ref: C.A. 2554).
Funding
This research did not receive any specific grant funding from agencies in the public, commercial, or not-for-profit sectors.