
Abstract
INTRODUCTION:
Previous research has shown that 40% of people who suffer an ankle sprain will develop chronic ankle instability (CAI). Both mechanical insufficiencies and functional insufficiencies contribute to the development of CAI. In order to reduce the incidence of CAI and to provide the highest standard of care to patients, physiotherapists must be able to identify these insufficiencies in order to develop an appropriate treatment pathway.
METHODS:
We designed an online survey which the Irish Society of Chartered Physiotherapists sent to members within particular subgroups. The survey allowed us to determine the competencies of Chartered Physiotherapists in conducting a comprehensive clinical ankle assessment, their knowledge of CAI and their self-rated confidence in treating and assessing an ankle injury.
RESULTS:
From the emails distributed, 263 people chose to take part. Of those, 87 people completed the survey, yielding a response rate of 33%. Of the 87 respondents, 49% could not identify any mechanical impairments, and 40% could only identify one. 47% could not identify any functional impairments, 21% identified one and 25% identified two. 62% of participants did not include ankle joints arthrokinematics in their clinical assessments of ankle injury, and 60% did not include patient reported outcome measures. Therefore the majority of Irish physiotherapist’s are not meeting the minimally accepted standards of ankle injury assessments. Despite this, 86% of participants rated themselves as 6/10 or greater in their own clinical assessment proficiency.
CONCLUSION:
Our results highlight that Irish physiotherapist have a limited understanding of the mechanical and functional insufficiencies contributing to the development of CAI.
Keywords
Abbreviations
Chronic ankle instability
International Ankle Consortium
Irish Society of Chartered Physiotherapists
Rehabilitation Orientated Assessment
Introduction
Lateral ankle sprains are one of the most commonly sustained musculoskeletal injuries with a high prevalence particularly amongst athletes and individuals who engage in recreational sports [1]. In the UK, lateral ankle sprains account for 3–5% of all musculoskeletal injury presentations to hospital emergency departments equating to 5,600 daily incidents [2]. Despite the high prevalence and potential for the development of long-term injury-related symptoms, lateral ankle sprains are often regarded as mild injuries that will recover with limited intervention. Unfortunately, the opposite is the case with more than 40% of individuals who incur an acute lateral ankle sprain developing chronic ankle instability (CAI) within the first 12 months following their injury [3].
An article published by Delahunt et al. in 2010 [4] has detailed the characteristic features used to classify individuals with CAI reported in studies published up to 2009. These features include: (1) the regular occurrence of “giving way” of the ankle joint; (2) self-reported feelings of ankle joint instability; (3) recurrent injury. These characteristic features of CAI suggest that it is likely the result of a degradation in the capacity of the sensorimotor system to maintain functional joint stability.
Traditionally, CAI has been attributed to two causes: mechanical instability and functional instability. However such a reductionist approach does not accurately encapsulate the wide range of impairments which may contribute to the development of CAI. In a seminal article, Hertel [5] discusses the pathomechanics and pathophysiology of CAI (Fig. 1). This article presents data which illustrates that mechanical and functional instability are unlikely to exist as separate entities but more likely to form a continuum of pathologic contributions to CAI. Either entity can consist of many separate insufficiencies either in combination or isolation. Specific insufficiencies contributing to the presence of mechanical instability include: (1) pathologic laxity; (2) arthrokinematics changes; (3) synovial changes; (4) degenerative joint disease. Specific insufficiencies contributing to the presence of functional instability include: (1) impaired proprioception; (2) impaired neuromuscular control; (3) strength deficits; (4) impaired postural control.
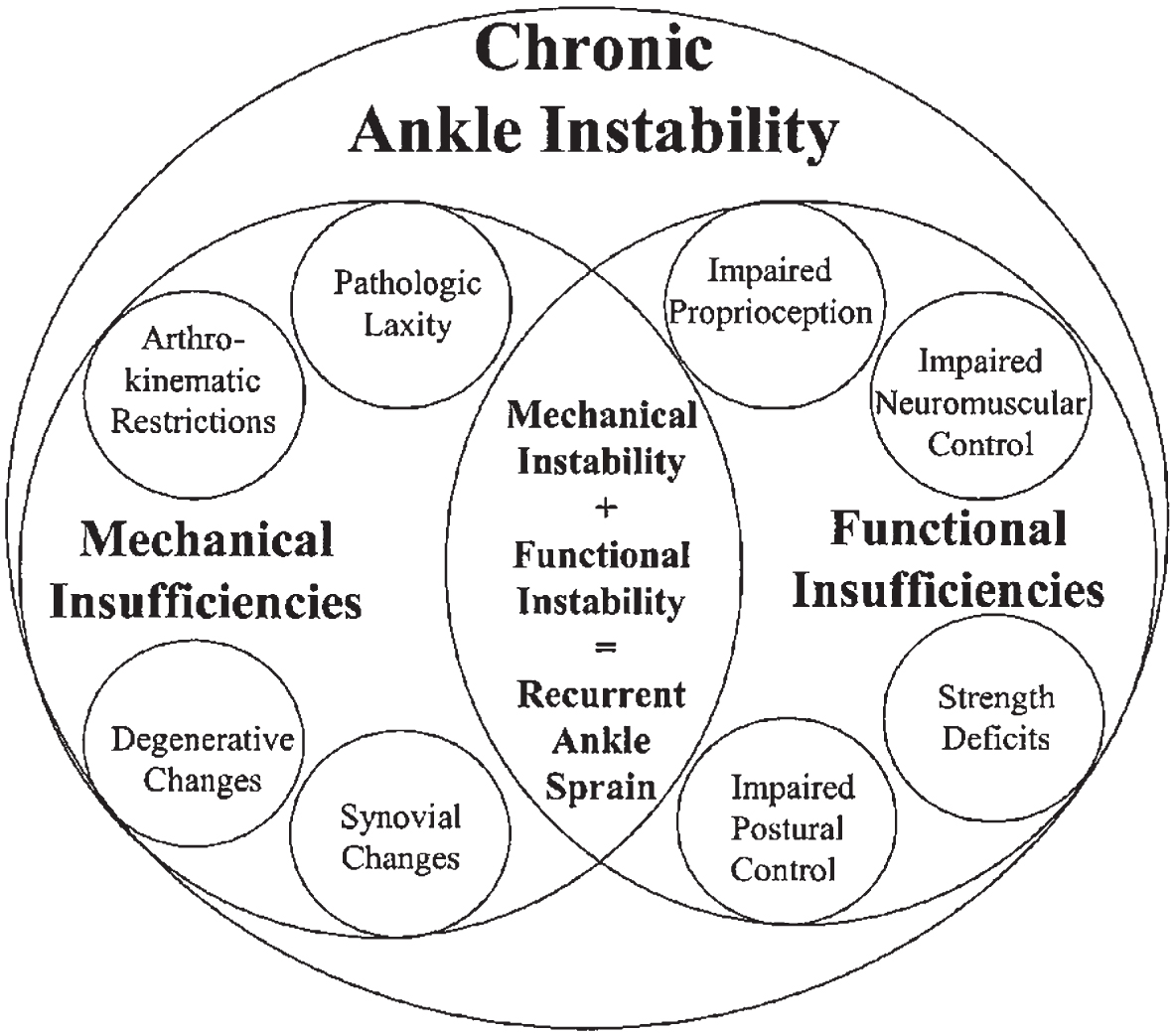
Paradigm of CAI (5).
The paradigm of CAI presented by Hertel [5] can be used to guide practitioners in their clinical assessment of acute lateral ankle sprain patients and CAI patients. It allows them to focus the attention of their clinical assessments towards impairments known to associate with CAI. In doing so, practitioners can then use the findings of their assessments to implement a patient-specific impairment-based model of injury rehabilitation, which could mitigate the risk of developing long-standing ankle sprain injury associated symptoms, including “giving-way”, feelings of ankle instability and recurrent injury.
Kerin and Delahunt [6] performed a cross-section analysis of Irish Chartered Physiotherapists who regularly treat patients with CAI in order to ascertain their knowledge and practice patterns relating to the condition. An anonymous survey was distributed to physiotherapists, who were asked to complete it without the assistance of textbooks or other resources. The responses to the survey indicated that most physiotherapists had a good understanding of the concept of CAI. However, the responses highlighted that there was a lack of understanding regarding the functional and mechanical insufficiencies known to associate with CAI. Without proper understanding of the spectrum of insufficiencies which associate with CAI, it is plausible to suggest that sub-optimal care is being administered to CAI patients, which misaligns with the principles of evidenced-based practice.
Despite advances in the literature regarding the understanding of CAI, the prevalence of patients with longstanding ankle sprain injury associated symptoms remain high. Some of the suggested reasons why people develop CAI may be due to inadequate rehabilitation [1], an emphasis on an expediated early return-to-sport [7] and poor follow up following initial treatment in emergency departments [8].
The results of the study by Kerin and Delahunt [6] suggest that a lack of understanding by Irish Chartered Physiotherapists of the mechanical and functional insufficiencies known to associate with CAI may lead to an incomplete or sub-optimal treatment strategy, perhaps contributing to the high numbers of acute ankle sprains which progress to CAI. We hypothesise that Irish Chartered Physiotherapists continue to have a limited understanding of the range of impairments which associate with CAI. Thus, the aim of this study was to conduct a cross sectional analysis of Irish Chartered Physiotherapists who treat acute ankle injuries, with the objective of evaluating their competencies in conducting a comprehensive clinical ankle assessment, their knowledge of CAI and ascertaining their self-rated confidence in treating and assessing an ankle injury. We hypothesised that Irish Chartered Physiotherapists are unlikely to be conducting a comprehensive clinical ankle assessment. As such, Irish Chartered Physiotherapists may not be interacting with the principles of evidence-based practice, which could possibly provide an explanation for the high proportion of acute lateral ankle sprain patients who develop long-standing injury associated symptoms and CAI.
Methods
Participants
Ethical approval for the study was received from the School of Public Health, Physiotherapy and Sports Science Post-Graduate Ethics Committee. An online survey was conducted among a sample of Chartered Physiotherapists in Ireland.
An application was submitted to the Irish Society of Chartered Physiotherapists (ISCP) to send the survey to members of the Chartered Physiotherapists in Sports and Exercise Medicine (CPSEM), Chartered Physiotherapists in Private Practice (CPPP) and Chartered Physiotherapists in Musculoskeletal Therapy (CPMT) subgroups. Physiotherapists who were not a member of any of these subgroups were not considered for inclusion. The survey was sent by the ISCP to members’ email addresses. Contained within the email was a link to the survey, which was created with the software Qualtrics. Qualtrics did not save any identifiable information of the participants. Before the survey was released, a pilot study was conducted with 5 experienced Chartered Physiotherapists to ensure that the survey was clear and concise in its presentation and easily understandable. An information sheet was also included in the email. This document outlined the aims of the survey, types of questions which would be asked and ensured participants about the anonymity of their participation and responses to the questions. Participants were instructed to complete the survey without the help of textbooks, colleagues or the internet.
Inclusion/Exclusion criteria
All participants were charted physiotherapists, who practice or had studied in Ireland. Students and other disciplines were excluded. ISCP members who were not members of the aforementioned subgroups were excluded.
Online questionnaire
An anonymous online questionnaire was designed with the objective of ascertaining Chartered Physiotherapist’s competencies in conducting a comprehensive ankle joint assessment, their knowledge of CAI, and their self-rated confidence in treating and assessing an ankle injury.
To assess participants’ competencies in conducting a comprehensive clinical assessment of an acute lateral ankle sprain injury the following questions were mapped to the recent 2019 consensus statement of the International Ankle Consortium [9]: (1) do you assess ankle joint swelling?; (2) do you assess ankle joint range of motion?; (3) do you assess ankle muscle strength?; (4) do you assess joint arthrokinematics?; (5) do you assess static postural balance?; (6) do you assess dynamic postural balance?; (7) do you use any patient reported outcome measures specific to the ankle?
To assess Chartered Physiotherapists’ knowledge of CAI, participants were asked to describe the mechanical and functional insufficiencies that associate with CAI. We mapped participants’ answers to the seminal model of Hertel [5], who outlined the following mechanical insufficiencies: (1) pathological laxity; (2) arthrokinematics impairments; (3) degenerative changes; (4) synovial changes. The following functional insufficiencies were outlined in the seminal model of Hertel [5]: (1) neuromuscular impairments; (2) strength impairments; (3) proprioceptive impairments; (4) neuromuscular control impairments.
To determine Chartered Physiotherapist’s self-rated confidence in treating and assessing an ankle injury, the following questions were used: (1) rate your level of expertise in the clinical assessment of patients with an acute lateral ankle sprain and/or chronic ankle instability; (2) rate your level of expertise in the diagnosis of patients with an acute lateral ankle sprain and/or chronic ankle instability; (3) rate your level of expertise in the treatment and rehabilitation of patients with an acute lateral ankle sprain and/or chronic ankle instability.
With reference to these questions the following definitions were used: (1) clinical assessment refers to the clinician’s ability to evaluate the patient’s injury and associated prognosis based on information gathered from physical examinations/tests and the patient’s medical history; (2) diagnosis refers to the clinician’s ability to determine which condition (injured structures) likely explain the patient’s symptoms; (3) expertise in treatment/rehabilitation is defined by the clinician’s ability to implement a management strategy that will allow the patient to recover full function without any limitation in future activities and to minimise injury recurrence. For all three questions, participants were required to rate their level of expertise on a scale whereby 0 = no level of expertise, while 10 = maximum level of expertise.
Results
From the emails distributed, 263 people chose to take part. Of those, 87 people completed the survey, yielding a response rate of 33%. Of the respondents, 71% were female. The settings in which they were employed varied, with 53% working in private practice, 28% in an acute hospital setting, 12% in primary care and 4% in professional sports. The mean age of respondents was 40 years (SD = 8.37 years). The average years of experience since qualification was 16 years (SD = 8 years). One respondent had a PhD, 41 (47%) had a master’s degree, 40 (46%) had a bachelor of science degree and 5 (6%) had a diploma. After the demographic information was gathered, respondents were asked: ‘on average how many ankle injuries do you see on a weekly basis?’. The mean was 2.4, with 10% seeing no ankle injuries per week, 45% seeing 1-2, 36% seeing 2–6 and 8% assessed and treated more than 6 ankle injuries per.
Competencies in conducting a comprehensive clinical assessment of an acute lateral ankle sprain injury
The International Ankle Consortium have previously reached a consensus on what particular components are vital to, and should be included in the clinical assessment of acute lateral ankle sprain injuries [9]. The expert panel agreed on ten important considerations which are outlined in (Fig. 2).
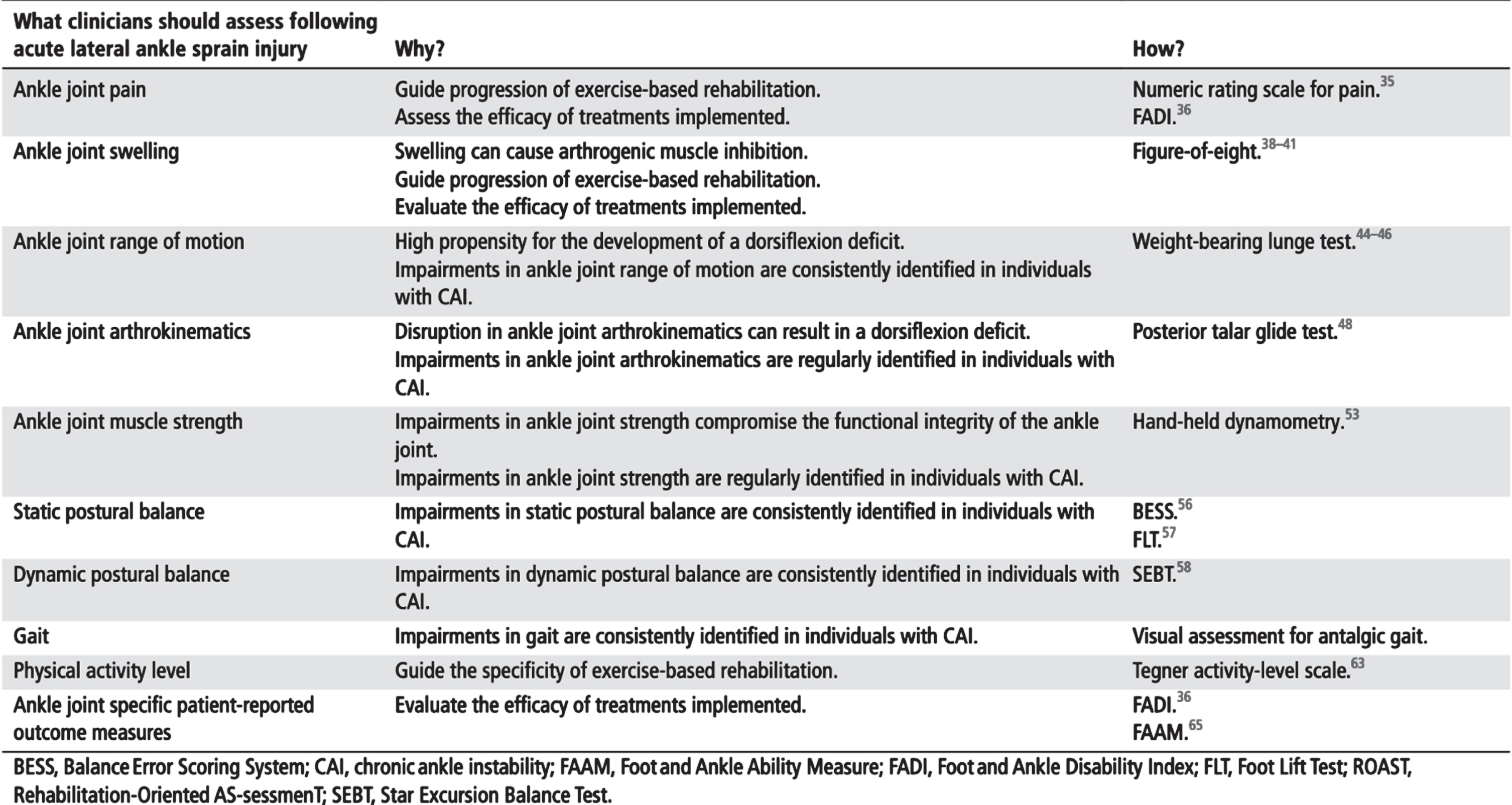
The experts on the panel of the International Ankle Consortium agreed that the above assessment components should be clustered and termed the International Ankle Consortium
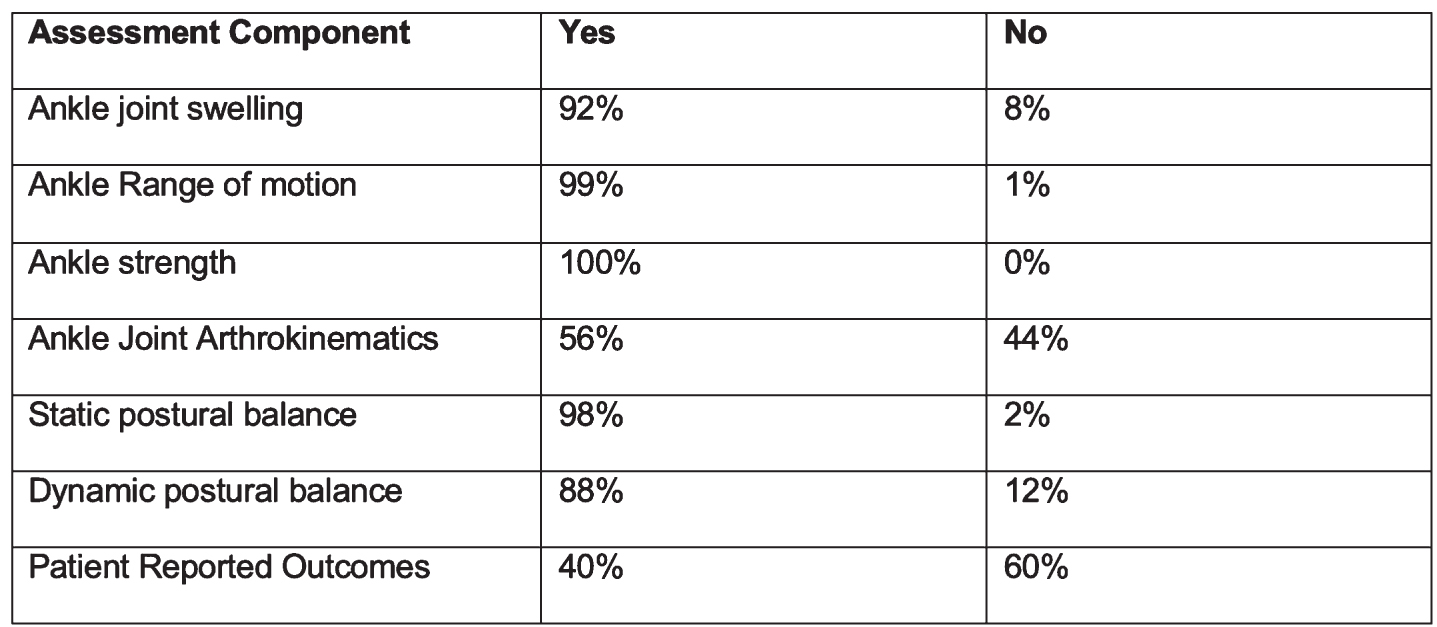
Percentage of participants who included components in their clinical ankle assessments.
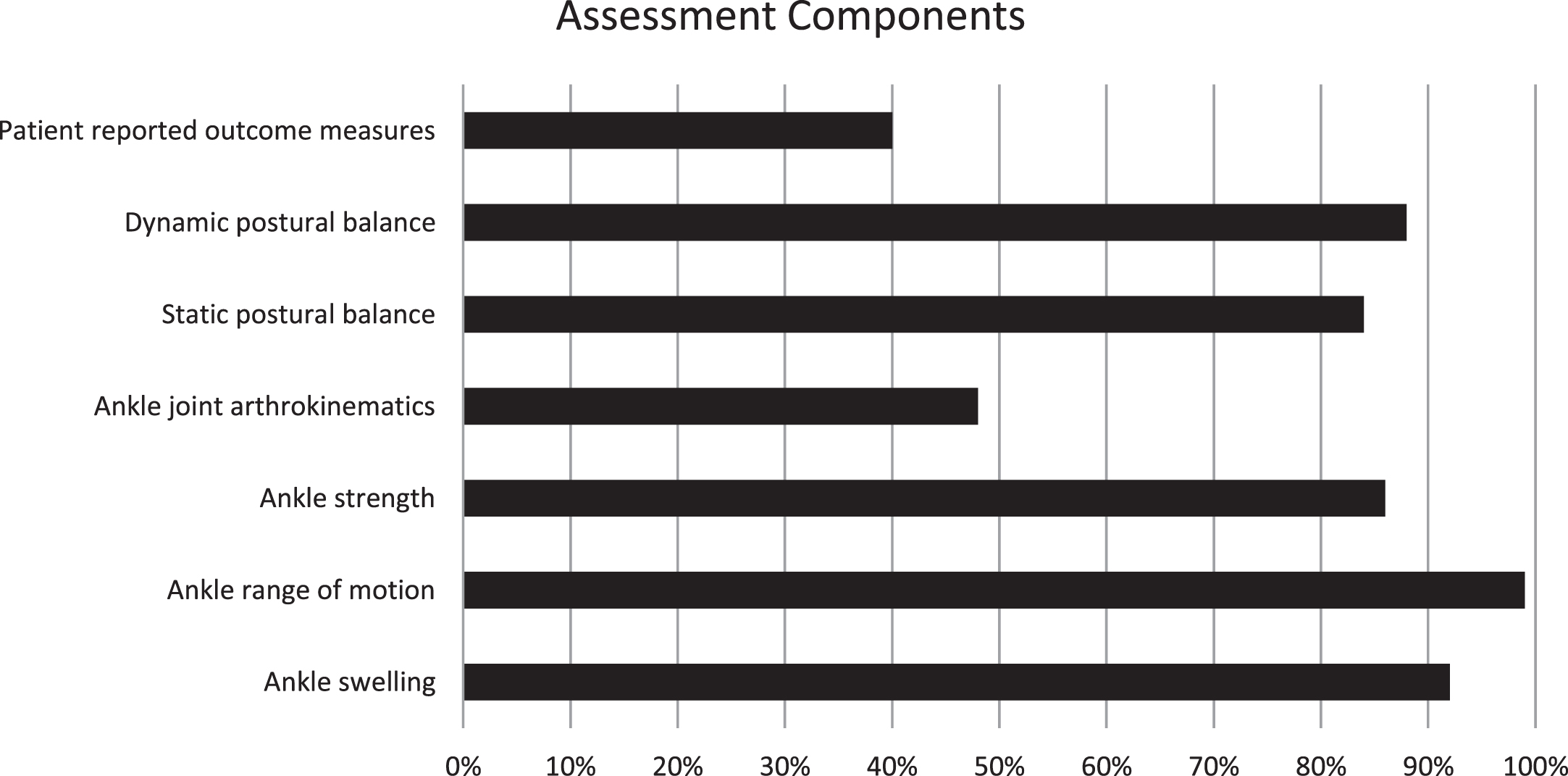
Bar chart representation of the percentage of participants who included components in their clinical ankle assessments.
The results demonstrated that a majority of participants did in fact include most of these components in their assessments, as outlined in the ROAST guidelines [5], with the exceptions of ankle joint arthrokinematics (56%) and patient-reported outcome measures (40%). The most commonly assessed components were strength (100%), ankle joint range of motion (99%) and static postural balance (98%).
In order to assess the participant’s knowledge of CAI, participants were asked to name the mechanical and functional insufficiencies that are associated with CAI. With regard to mechanical insufficiencies, 49% of participants could not describe any of the insufficiencies, 40% identified one, 8% identified two, 2% identified three, and 0% identified four. Pathologic laxity was the most commonly identified insufficiency at 31% and synovial changes the least, at 3%. Results of the mechanical insufficiencies are represented in (Fig. 5).

Results of participants ability to identify mechanical impairments.
With regard to functional insufficiencies, 47% participants identified zero, 21% identified one, 25% identified two, 2% identified three and 3% identified four. Proprioception was the most commonly identified insufficiency at 49% and postural control the least, at 6%. Results are represented in (Fig. 6).
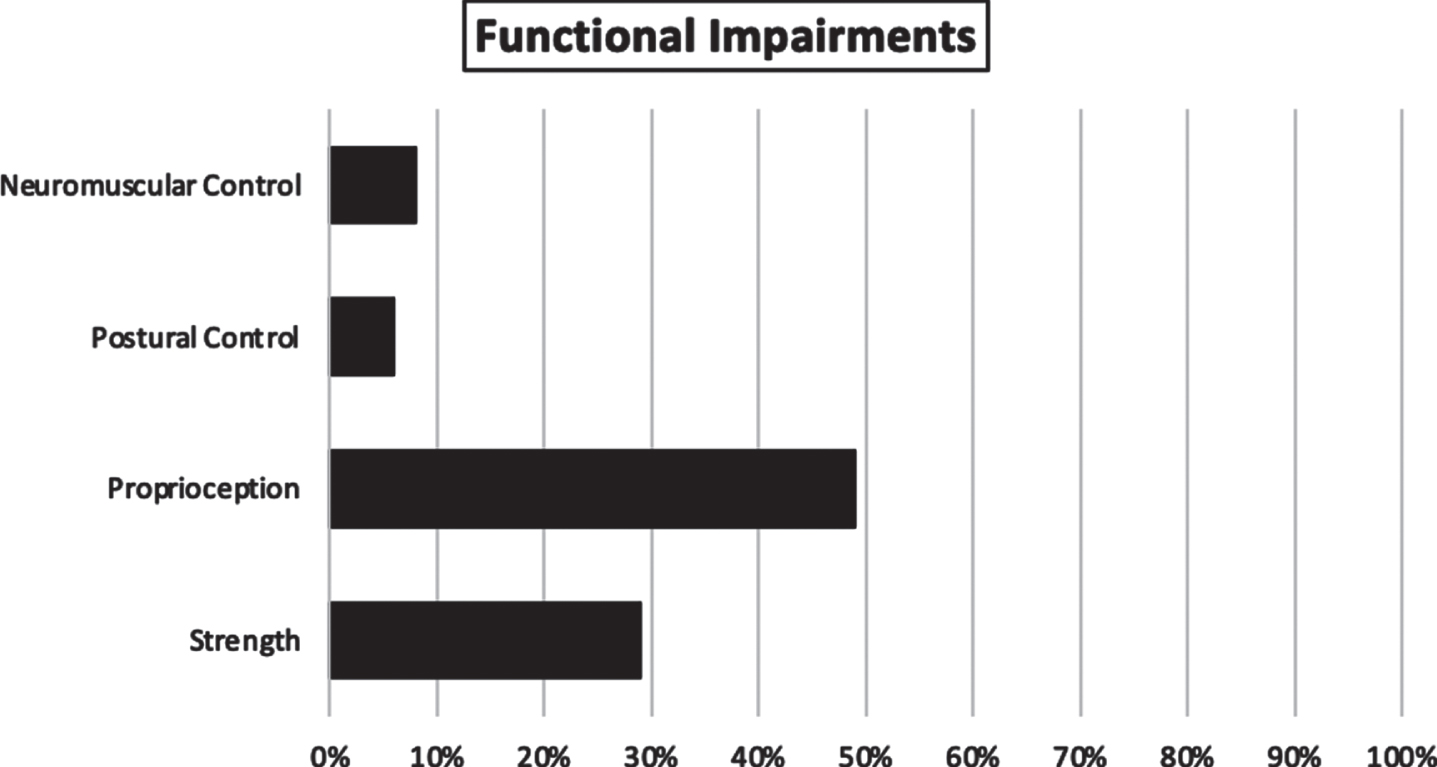
Results of participants ability to identify functional impairments.
Participants were asked to self-rate their own level of expertise or proficiency in the diagnosis, treatment/rehabilitation and clinical assessment of an ankle injury. Participants were asked to select a number between one and ten on a sliding bar graph. The questionnaire instructed that a score of ‘0 = no level of expertise’ and a score of ‘10 = maximum level of expertise’.
Clinical assessment was defined in the questionnaire as the clinician’s ability to evaluate the patient’s injury and associated prognosis based on information gathered from physical examinations/tests and the patient’s medical history. The mean selected score was 7.01/10. The most frequently selected score was 7/10 (30% of participants). This was closely followed by 8/10 (26% of participants). One participant answered 1/10 (1%). One participant answered 10/10 (1%). 75 participants (86%) rated themselves as either 6 or greater out of ten in the clinical assessment of an ankle injury. 12 participants (14%) rated themselves as between 1–5/10 in their clinical assessment proficiency.
Diagnosis as defined in the questionnaire referred to the clinician’s ability to determine which condition or injured structures likely explains the patient’s symptoms. The participants were asked to rate themselves on a scale of 1–10. The results are as follows:
The mean score selected was 7.08/10. The most commonly selected score was 7/10 (27% of participants). The second most frequent score was 8/10 (26% of participants). One participant answered 1/10 (1%) and 3 participants answered 10/10 (3%). 74 participants (86%) rated themselves with a score of either 6 or greater out of ten in their clinical diagnostic skills. 12 participants (14%) rated themselves as between 1–5/10 in their ankle diagnosis proficiency. One participant failed to answer the question at all, meaning that 86 of 87 participants answered this question completely.
Expertise in the treatment/rehabilitation of an ankle injury was defined in the questionnaire as the clinician’s ability to implement a management strategy that will allow the patient to recover full function without any limitation in future activities and to minimise injury recurrence. The participants rated themselves on a scale of 1–10. The results are as follows: the mean selected score was 7.20/10. The most commonly selected scores were 7/10 and 8/10, with 27 participants selecting each respectively (31%). 1 participant answered 1/10 (1%) and 1 participant answered 10/10 (1%). 80 participants rated themselves as either 6 or greater out of ten (92%). 7 participants rated their proficiency in the treatment or rehabilitation of an ankle injury as 5 or less out of ten (8%).
Discussion
The aim of this study was to evaluate Irish Chartered Physiotherapists’ competencies in conducting a comprehensive clinical ankle assessment, their knowledge of CAI and their self-rated confidence in treating and assessing an ankle injury. We hypothesised that Irish Chartered Physiotherapists are unlikely to be conducting a comprehensive clinical ankle assessment. In contrast to our hypothesis, Irish Chartered Physiotherapists do in fact seem to be conducting comprehensive ankle assessments as per the International Ankle Consortium ROAST guidelines [9], with the exceptions of the assessment of joint arthrokinematics and the inclusion of patient-reported outcomes in their clinical assessments. Irish Chartered Physiotherapists have also displayed a high self-rated proficiency in performing clinical ankle assessments. Irish Chartered Physiotherapists’ knowledge of CAI also appears to be lacking, and appears to have deteriorated slightly since similar research was conducted over a decade ago [6].
Competencies in conducting a comprehensive clinical assessment of an acute lateral ankle sprain injury
Most respondents in this study, in their clinical assessments, tested strength (100%), range of motion (99%), swelling (92%), static postural balance (88%) and dynamic postural balance (88%). With regards to these particular components, Irish Chartered Physiotherapists appear to be adhering to the minimally accepted standards of ankle injury assessment.
The ROAST guidelines endorse the assessment of ankle joint arthrokinematics as a central component of any ankle joint assessment. Following an ankle injury, alterations can occur in the arthrokinematics of any of the 3 joints of the ankle complex. One fault which occurs is that the distal fibula may become displaced anteriorly and inferiorly. When this occurs, the ATFL may be more slack in its resting position, as the lateral malleolus is displaced. Hence, when the ankle inverts during a typical ankle sprain injury event, the talus can move through a greater range of motion before the ATFL becomes taut. This mechanism is believed to contribute to recurrent ankle injuries [5]. Dorsiflexion is also commonly impaired following an ankle injury. Restrictions in the glide of the talus on the mortise have been demonstrated [10] reducing the ankle’s range of dorsiflexion. When this occurs the ankle cannot reach it’s closed packed position, which due to the bony anatomy of the ankle, is a position of stability. As a result the ankle will be more prone to invert and internally rotate [5]. Mobilisation techniques have been shown to be effective in improving ankle dorsiflexion and posterior talar glide [11]. Identification of arthrokinematics abnormalities are essential in order to create a comprehensive management pathway.
Only 48% of participants in this study assessed ankle joint arthrokinematics. A substantial number of respondents in this study, with regard to arthrokinematics, do not meet the minimum standards of a clinical lateral ankle injury, as endorsed by the International Ankle Consortium [9].
Patient reported outcome measures are also a crucial component of an ankle assessment, as advocated in the ROAST guidelines [9]. Only 40% of participants in this study include patient reported outcome measures in their clinical ankle assessments. By including these outcome measures, physiotherapists can adhere to higher standards of injury assessment and measurement of patient’s progress in the course of their assessment and treatment. These patient reported outcome measures may reveal distinct perceptions and characteristics to the patient’s individual impairments and help guide rehabilitation. Several patient reported outcome measures exist which are commonly used for patients with CAI [12]. The majority (60%) of Irish physiotherapists did not include patient reported outcome measures in their practice, and therefore do not meet the minimally accepted standards of a clinical assessment of an ankle, as proposed by the International Ankle Consortium [9].
Knowledge of CAI
Irish physiotherapist’s knowledge of CAI, assessed via their knowledge of the associated mechanical and functional impairments as outlined by Hertel [5], appears to be lacking. Nearly half (49%) of the participants could not identify any of the mechanical insufficiencies, and nobody could identify all four. With regards to functional insufficiencies, nearly half (47%) could not identify any, and only 3% identified all four. In order to have a good understanding of CAI, physiotherapists must have good knowledge of these various insufficiencies and how they interact with each other, contributing to the development of CAI and the continuum of recurrent injuries. Kerin and Delahunt [6] performed a similar study over a decade ago. The results of this study are compared with this previous study below in (Figs. 7 and 8).

Comparison of participant knowledge of functional impairments in this study (Blue) vs. Kerin.F, Delahunt E (2010) (Orange).
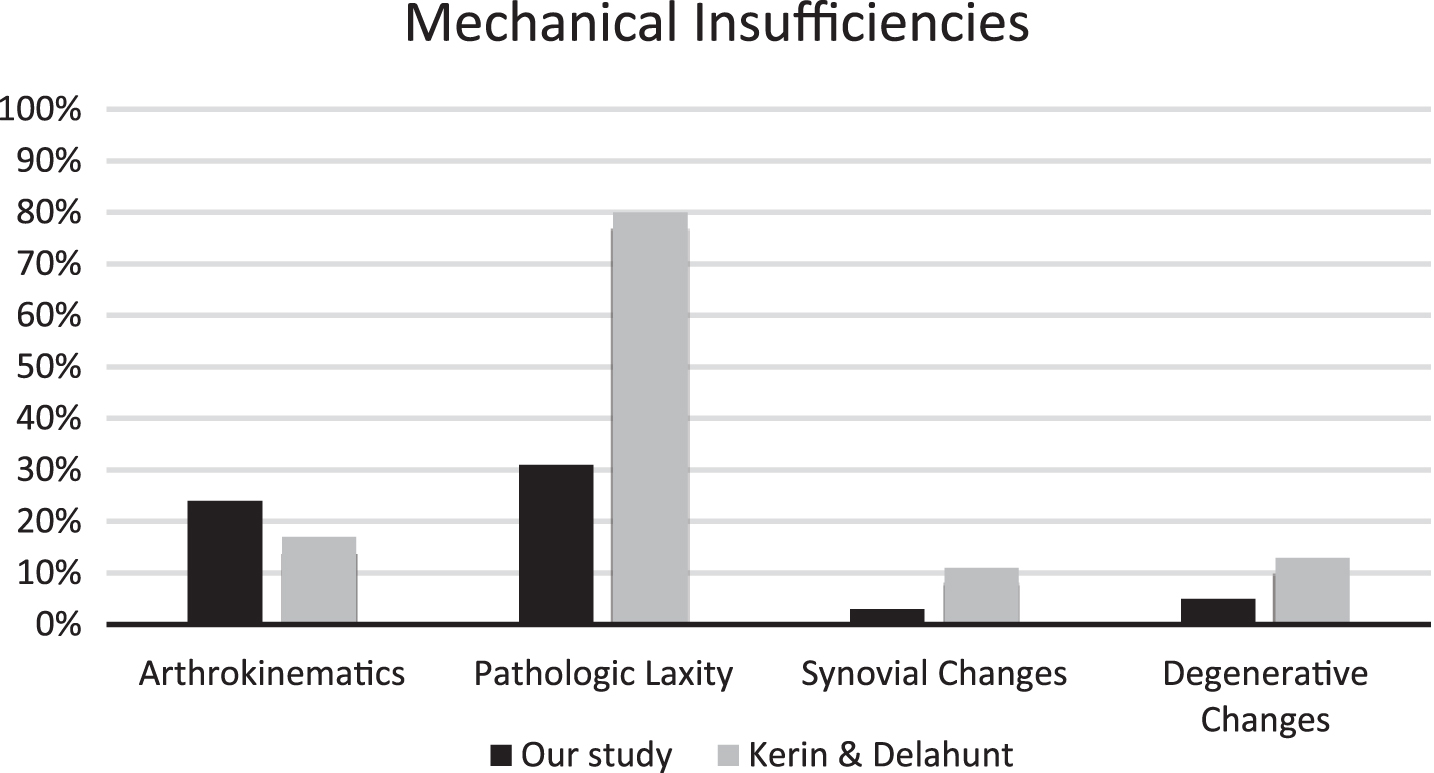
Comparison of participant knowledge of mechanical impairments in this study (Blue) vs. Kerin.F, Delahunt E (2010) (Orange).
The participants in Kerin & Delahunt’s study were capable of identifying more impairments than the participants in our study. There was a higher rate of identification for all impairments except arthrokinematics. These results suggest that Kerin & Delahunt’s participants demonstrated a higher knowledge of CAI than those in our study. The percentage ratios of identification of impairments was similar across both studies. Proprioception was the highest identified functional impairment in both studies. Postural control was the lowest identified functional impairment in our study. Postural control and neuromuscular control were both the lowest identified functional impairment in the Kerin & Delahunt study, with the same percentage of participants who selected them. ‘Pathologic Laxity’ was the most identified mechanical impairment in both studies, and synovial changes the lowest in both.
The results of this study suggest that Irish physiotherapists do not have a comprehensive understanding of CAI, as highlighted by their absence of a thorough understanding of the associated functional and mechanical insufficiencies associated with CAI. Previous research has highlighted this gap in knowledge [6]. Irish physiotherapist’s knowledge of CAI appears to have in fact worsened since that research was carried out in 2010. The authors of this study hypothesise that this may be due to a lack of educational courses being available to Irish physiotherapists focusing on CAI and its associated impairments, and their relation to treatment and rehabilitation.
Despite these shortfalls in Irish physiotherapist’s clinical assessments, participants still self-rated their clinical assessment proficiency very highly. 75 participants (86%) rated themselves as either 6 or greater out of ten in the clinical assessment of an ankle injury. 12 participants (14%) rated themselves as between 1–5/10 in their clinical assessment proficiency. Despite these reasonably high levels of self-rated proficiency, only 28% of all physiotherapists included all seven assessment components in their clinical assessments. 36% included 6 out of 7 components. 23% included 5 components. 13% included 4 or less components. However, considering the above data, despite being unsatisfactory in the areas of arthrokinematics joint assessments and patient reported outcomes, Irish physiotherapists appear to be mostly meeting the minimally accepted standards of a clinical lateral ankle injury.
Limitations of this study
This study only represents a small amount of Irish physiotherapists and may not be applicable to all practitioners in the country. Of the 246 physiotherapists who agreed to participate, only 87 of those finished the survey. This reflects 35% of the original cohort. The survey was only sent to physiotherapists within certain subgroups of the ISCP. The physiotherapists within those subgroups were expected to be those who would most likely be assessing and treating ankle injuries. However there may have been physiotherapists who regularly treat ankle injuries, who were not members of those subgroups, who were not contacted by the ISCP to complete our survey.
The participants in this study are all Irish physiotherapists, hence these results cannot be extrapolated to physiotherapists in other countries. Physiotherapists may have different working practices or have greater or lesser educational emphasis on CAI. Hence the data in this study cannot be assumed to be similar to physiotherapists in other countries.
This study only sought to ascertain if physiotherapists included certain components in their assessments, with a ‘yes’ or ‘no’ answer. This study did not delve into how the participants performed that part of their assessment or whether their means of doing so was correct, or in accordance with the latest literature. Therefore participants may have declared that they included various components in their clinical assessments, however their execution of these assessments may have been incorrect. Further research is needed to clarify this.
Conclusions and implications for clinical practice
This study demonstrated that Irish physiotherapists do not have a comprehensive understanding of CAI, or of the associated impairments. Without this knowledge, physiotherapists are unable to adhere to the principles of evidence based practice, and cannot deliver the highest standard of care to their patients. As a result of this lack of knowledge, incidence of CAI will likely remain high and Irish physiotherapists will continue to deliver sub-optimal care to their patients.
This study demonstrates that Irish physiotherapists have a high level of self-rated proficiency in their clinical ankle assessments. Despite this, nearly half did not assess for ankle joint arthrokinematics, and 60% did not use patient reported outcomes in their clinical assessments. In general Irish physiotherapists performed overall comprehensive assessments, with the exception of arthrokinematics joint assessments and the use of patient reported outcomes.
Conflict of interest
The authors have no conflict of interest to report.