
Abstract
BACKGROUND:
Neurodynamic tests (NDT) have shown to be useful in evaluating neural tissue involvement. Clinicians evaluate NDT using range of motion, sensory responses like location or quality of symptoms, Nerve conduction values and compare its results with normal values. Currently, there are no studies in lumbar radiculopathy patients that define the normal response to peroneal neurodynamic test (NDTPER)
PURPOSE:
To study the sensory responses to neurodynamic testing of peroneal nerve in patients with lumbar radiculopathy.
DESIGN:
A cross sectional study design.
METHODS:
NDTPER was performed on 57 patients with lumbar radiculopathy. Hip flexion angle was taken at the onset of symptoms (P1) and point of maximally tolerated symptoms (P2), quality and distribution of symptoms were recorded. Sensory nerve conduction velocity measure (SNCV) was also noted in those patients.
MAIN RESULTS:
The descriptor of nature of sensory responses most often used by patients was tingling (28.07%) in the lateral foot (26.32%). Hip flexion was significantly higher at P2 than P1 (mean difference: 22.54±3.73°; 95% CI: 21.55°, 23.54°; p < 0.0001). The SNCV of affected limb was marginally reduced but not statistically significant compared to contralateral limb (mean difference: –1.467±0.8013; 95% CI: –3.054, 0.1209; p = 0.0698).
CONCLUSION:
This study describes the hip angle at which symptoms are reproduced, nature and distribution of sensory responses to the NDTPER in patients with lumbar radiculopathy. However, the sensory nerve conduction velocity of affected limb was reduced marginally but not statistically significant as compared to unaffected limb.
Introduction
Low back pain is one of the foremost common musculoskeletal complaints seen in clinical practice and is the leading cause of disability all over the world. The differential diagnosis for low back pain is broad and should include lumbar radiculopathy among other diagnoses [1]. Lumbar radiculopathy affects both men and women, and its prevalence is estimated to be between 3% and 5% of the population. Symptoms begin in midlife, with men often affected in their 40s while women in their 50s and 60s [2]. Lumbar radiculopathies most commonly occur at L5 (48%), S1 (30%), L4 (17%), L3 (5%), S2 (4%) and L2 (3%) [3].
Radiculopathy is most commonly caused by irritation of a specific nerve, which can occur anywhere along the nerve course, and is most commonly caused by compressive pressures [4]. In the lower extremity, various nerves originate from the lumbar and lumbosacral plexus out of which the sciatic nerve. It is an important nerve which supplies the major part of the lower extremity and is most commonly affected in lumbar radiculopathy [5]. It later divides into tibial and peroneal nerve at popliteal fossa [6]. Due to the proximity of the common peroneal nerve and its branches to the lateral aspect of the proximal lower leg, injuries to it are very common [6]. As in lumbar radiculopathy there is compression and irritation of the nerves so the nervous system should be placed in a healthy environment for normal functioning of nervous system [7].
For the evaluation of lumbar radiculopathy, the clinical neurological examination is useful [8, 9]. It includes physical assessment, neuroimaging, and electrodiagnosis. One of the useful physical examinations is assessing the sensitivity of peripheral nerves which is known as mechanosensitivity [9]. For assessing mechanosensitivity of the nervous system, neurodynamic tests are performed. SLR 4 or peroneal neurodynamic test is used to evaluate the mechanical and sensory functioning of the peroneal nerve. It produces mechanical and/or physiological changes on the nervous tissues in the lower limb and lumbar region, which is essential in our studies [10]. Clinicians assess neurodynamic tests by comparing sides/or comparing the results to normal values of the range of motion, sensory responses such as location or quality of symptoms [11].
In electrodiagnosis, a nerve conduction study is the most important diagnostic method to evaluate the nerve impairment in the extremities [12]. Nerve conduction velocity (NCV) test is the most popular and reliable method used to investigate the velocity of nerve conduction for peripheral nerves in both upper and lower limbs. To assess the functional integrity of sensory nerve fibers of the body, sensory nerve conduction velocity (SNCV) is used. It involves electrically stimulating a peripheral neuron and recording from a completely sensory part of the nerve. The delay and distance between the stimulating and recording electrodes are used to determine the sensory NCV [13].
Previous studies were focused on the neurodynamic test of the peroneal nerve in asymptomatic individuals [14]. However, there were no studies found to investigate the responses of neurodynamic test of the peroneal nerve in symptomatic individuals i.e., in patients with lumbar radiculopathy. In addition, the nature of pain, type of response, and range of motion are subjective measurements that may vary. Henceforth, the aim of the study was to investigate the effect of the neurodynamic test of the peroneal nerve in symptomatic patients with lumbar radiculopathy along with sensory nerve conduction velocity of the peroneal nerve.
Materials and methods
Study design
This study was a cross-sectional study was carried out from February 2020 to September 2021. The local Ethics Committee approved the protocol of this study. Registration number for this trial was CTRI/2021/07/035034.
Study subjects
Total 57 patients with lumbar radiculopathy (31 males, 26 females) were recruited for the study. The patients who met the following criteria were included in the study: Age criteria: 40–60 years, medically or clinically diagnosed with lumbar radiculopathy and SLR 4 positive. Exclusion criteria for the participation were any previous spinal surgery, fracture of lower limb, diabetes or thyroid disorders, any type of autoimmune disease, range of motion limitation in any of the movements required to perform the NDTPER, any type of peripheral nerve injuries. Written informed consent was obtained from each subject prior to study participation.
Procedure
Determined eligibility to participate, based on inclusion and exclusion criteria, subjects were initially screened by the researcher who collected demographic data, medical history, past history, surgical history, and current medications. Subjects who met the selection criteria were subsequently provided with an explanation of the study procedures and instructions regarding the information they should provide during the NDTPER.
Before the primary component of the study, a pilot study was done for evaluation of sample size on 10 patients with lumbar radiculopathy. These patients which were included in the pilot study were excluded from the sample of the study.
Neurodynamic test of peroneal nerve
The starting position for the test was standardized so that the participants remained supine without a pillow (so that initial neural tension was avoided resulting from cervical spine flexion), their arms besides their body, and their lower limbs straight [15]. The standard sequence of movement was decided: plantarflexion/inversion of the ankle, foot, and toes, followed by hip flexion and knee extension. The main researcher performed this sequence of movements. The patient was instructed to tell both, the first appearance of symptoms (P1) and the point at which patients feel uncomfortable to continue with the test (P2), that is, the maximum tolerable point. The patients were asked to remember the quality and location of symptoms at the point of tolerance so that they could report this after the test was performed.
The characteristic of symptoms was recorded once the test was completed. To describe the quality or nature of the symptoms, the participants were told to choose between the following descriptors: stretching pain, tingling, pricking, numbness, burning, or combinations of these [14]. Participants may use any other descriptors for this purpose.
The location of symptoms was collected by marking the area of pain on the body chart depicting the affected lower limb. The body chart of the lower limb was divided into 6 areas. They were lateral foot, lateral leg, medial leg, posterior leg, posterior knee, and posterior thigh. Patients were asked to mark the location of their sensory responses on the body chart.
All the measurements were taken with the help of another therapist who participated only in this part of the study. The hip flexion angle at P1 and P2 was documented using an Inclinometer.
Sensory nerve conduction velocity
It was done using the Innotech Neuroscan EMG machine. The patients were examined while they were lying comfortably in the supine position. The room temperature was kept at 25–28°C. The filters were set at 20 Hz to 5 KHz. The sweep speed was set at 100 msec/division. A stimulus duration of 50–500μs and a current of 0–100 mA were required for effective nerve stimulation. The active recording electrode was positioned at a standard site, a point on the bimalleolar line, which was in the midway between the edge of the tibia and the tip of the lateral malleolus. The reference recording electrode was placed 3 cm distal to the active electrode over the dorsum of the ankle. The ground electrode was placed between the stimulating and recording electrodes. The site of stimulation was 10–15 cm proximal to the active ankle electrode, just anterior to the edge of the shaft of the fibula. Before applying electrodes, the skin was cleaned with an alcohol swab. Then the stimulus was given and the readings were recorded [16–18].

Neurodynamic test of peroneal nerve.

Sensory nerve conduction velocity of peroneal nerve.
The collected data was entered in Microsoft Excel and analysed using SPSS (Statistical package for the social sciences) version 24.0th. Mean and SD was calculated for hip flexion angles and sensory nerve conduction velocity and proportions were calculated for nature and area of symptoms. Also, data was represented in the form of visual impression like bar-diagram, Pie diagram etc. Paired t-test was applied for checking significant difference between S1 and S2 angles and difference between nerve conduction velocities of affected and unaffected limb. p-value of < 0.05 was considered statistically significant.
Results
Subjects characteristics
A total 57 patients with lumbar radiculopathy voluntarily participated in this study out of which 31 (54.39%) were males and 26 (45.61%) were females and the range was between 40–60 years.
Peroneal neurodynamic test
The descriptor for nature of symptoms most often used by patients was tingling (28.07%) during the neurodynamic test of the peroneal nerve which was followed by pain (24.56%) and stretching (21.05%). Percentages for each individual sensory response are depicted in Graph 1.
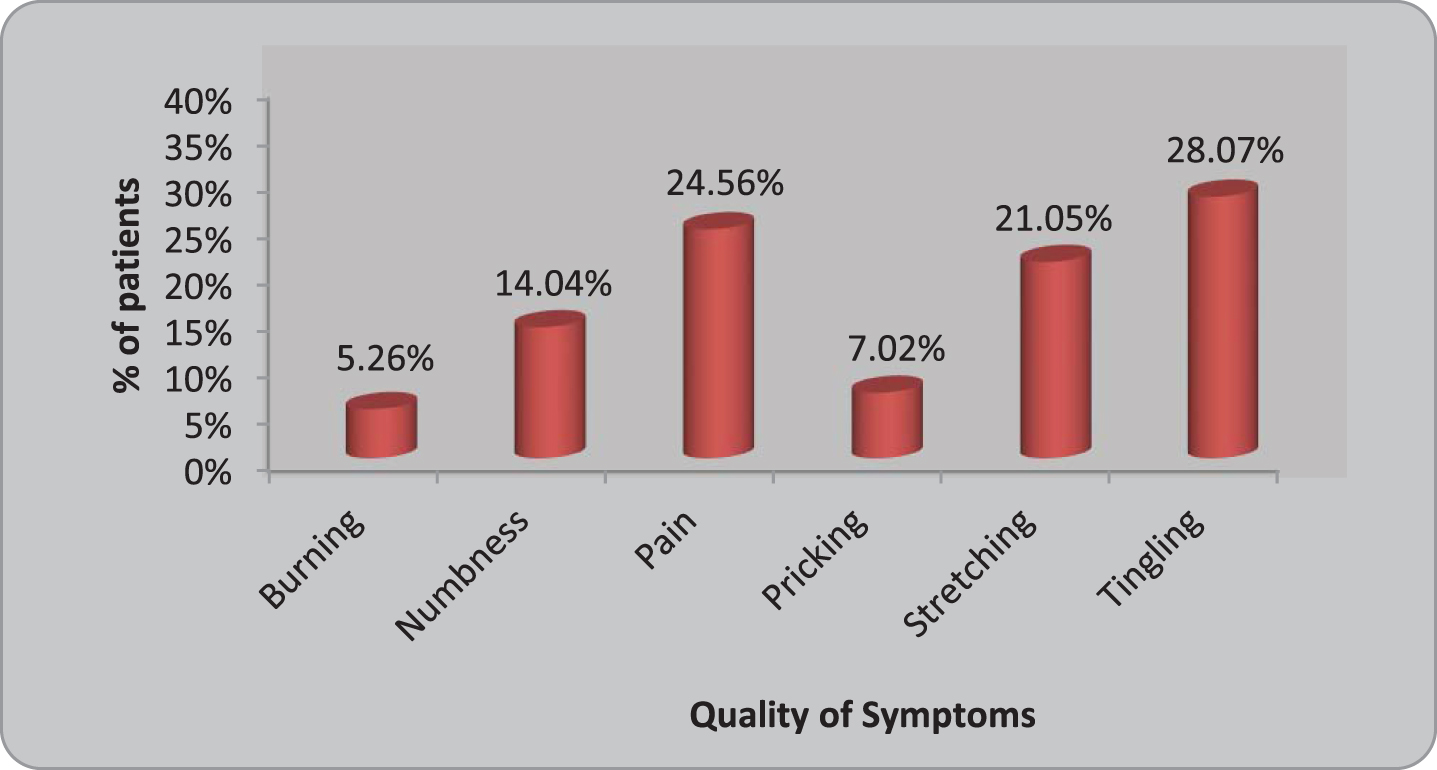
Distribution of patients according to nature of symptoms.
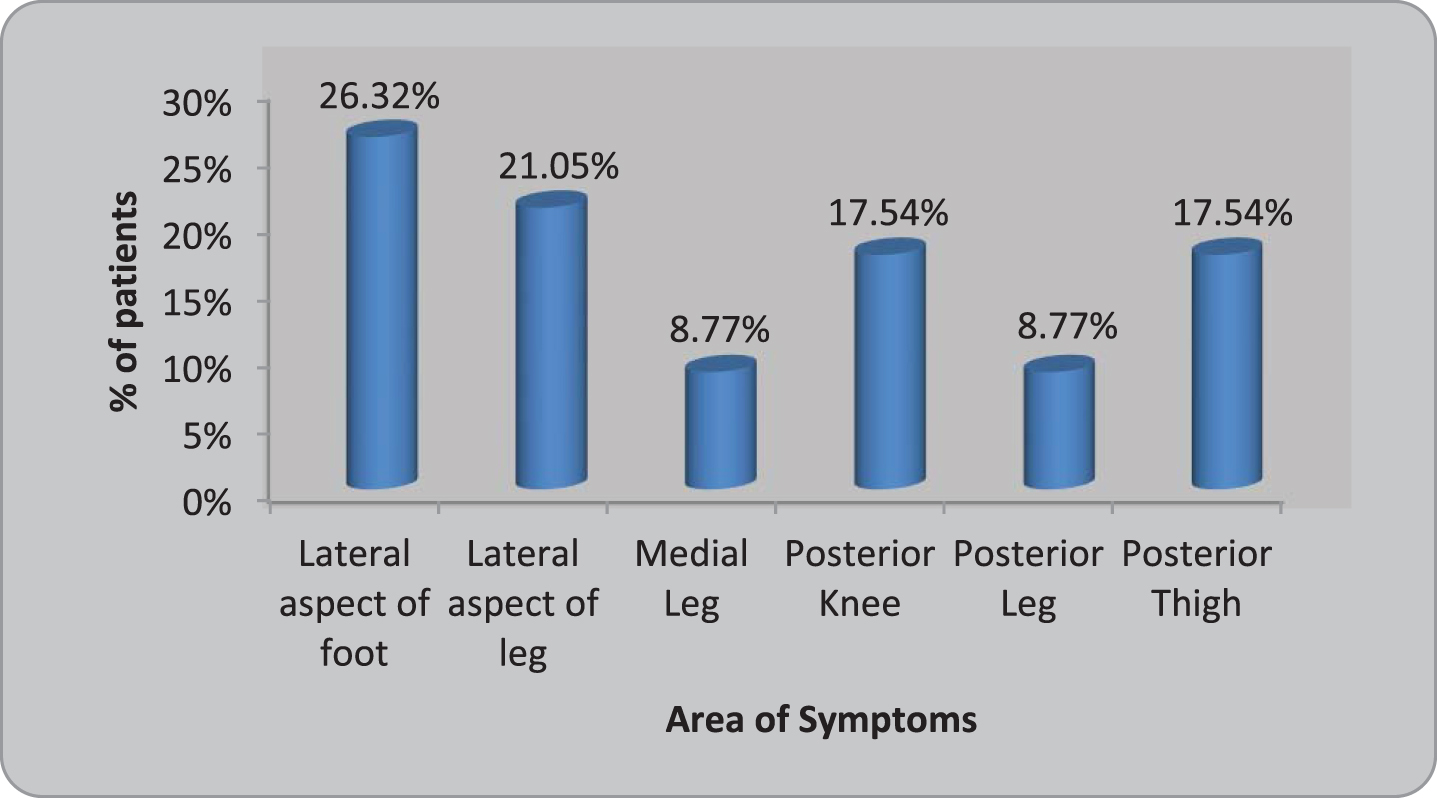
Distribution of patients according to area of symptoms.
It was found that the sensory responses were principally located at lateral aspect of foot (26.32%) followed by the lateral aspect of the leg (21.05%), posterior thigh (17.54%) and posterior knee (17.54%). Less commonly patients also reported symptoms in medial leg (8.77%) and posterior leg (8.77%). Percentages for each individual sensory response location are shown in Graph 2.
The mean range of motion for hip flexion for P1 was 51.87±8.58° and P2 was 74.42±9.06°. Hip flexion angle was significantly greater at P2 than P1 (mean difference: 22.54±3.73°; 95% CI: 21.55°, 23.54°; p < 0.0001).
Comparison of Hip Flexion angle of the affected limb at P1 and P2
The mean SNCV for affected limb was 52.38±4.17 m/s and for unaffected limb was 50.91±4.30m/s. On comparative evaluation, the data showed that the SNCV of affected limb was marginally reduced but not statistically significant as compared to unaffected limb (mean difference: –1.467±0.8013; 95% CI: –3.054, 0.1209; p = 0.0698).
Comparison of Nerve Conduction Velocity of peroneal nerve of affected and unaffected limb
Comparison of Nerve Conduction Velocity of peroneal nerve of affected and unaffected limb
The current study was conducted to evaluate the sensory responses of the neurodynamic test of the peroneal nerve in patients with lumbar radiculopathy. Most commonly sensory response occurred in the lateral aspect of the foot and the nature of the response was mainly tingling sensation. The mean of the hip angles at which the symptoms were produced at P1 was 51.87±8.54° and at P2 was 74.42±9.06°. The mean sensory nerve conduction velocity of the affected limb was 52.38±4.17 m/s and that of the unaffected limb 50.91±4.30 m/s. The SNCV of the affected limb was marginally reduced but not statistically significant when compared with unaffected limb and they were between the normal ranges of SNCV.
Neurodynamic test causes a relative increase in the length of anatomic structures through which various peripheral nerves travel. Normal nerve trunks are quite capable of complying with such length changes. Sensitization by a pathologic condition of neural tissues or peripheral nerves that are influenced by the relative length increasing during the SLR test causes non-compliance to the test, with the onset of pathologic pain along the course of the peripheral sciatic and peroneal nerve [19]. Moreover, NDT causes nerve root irritation and possible entrapment with decreased nerve excursion [20]. In regard to the quality of sensory responses “tingling” and “pain” were the most commonly reported descriptor and these results were similar to those of the previous studies done by G M Bove (2005). This type of response occurs when the neural mechanical interface affects the neural structures [21].
The most common location of sensory responses reported by patients during the neurodynamic test nerve of the peroneal was the lateral aspect of the foot (26.32%). It was found that the sensory responses were along the sciatic and peroneal nerve distribution because it is a common finding that the sensory responses during neurodynamic testing tend to localize along the distribution of the evaluated limb [22]. A similar sensory response along the lateral aspect of the foot was seen in the study done by E. Bueno-Gracia (2019). In the present study, sensory responses were mainly referred to in the distal part of the lower limb, along the peroneal distribution [14]. These findings also suggest that the neurodynamic test of the peroneal nerve quite specifically. The presence of positive NDT does not enable the clinician to identify the specific site of neural tissue injury; it merely indicates the entire neural tissue tract loaded during the test is exhibiting an increased amount of mechanosensitivity. In a non-uniform fashion, the neural tissues respond to movement through the development of strain, excursion, and stress [8]. Hence the sensory response may differ in different persons. Hence, we got other sensory responses in the lateral leg (21.05%), medial leg (8.77%), posterior knee (17.54%), posterior leg (8.77%), and posterior thigh (17.54%).
Hip ranges obtained in this study ranged from 36° to 83° for P1 and from 56° to 105° for P2. These angles of hip at which the symptoms are produced in this study were consistent with the previous findings of the SLR response to the sciatic nerve at ranges between 30° and 150° [9, 24]. A difference of more than 20° was observed between P1 and P2 which has been found in similar studies done on asymptomatic individuals [14, 24]. Differences in ROM may be obtained by the sensitization maneuvers used, that is, plantarflexion and inversion performed in the present study. These sensitization maneuvers may cause an increase in nerve tension [15]. Hence a significant difference between P1 and P2 should be taken into account when diagnosing a neural disorder, and the clinician should assume a higher ROM when using P2 as a reference point to stop the test.
To check the integrity of the sensory nerve fibers, a sensory nerve conduction study was evaluated in patients with lumbar radiculopathy. The mean SNCV for the affected limb was 52.35±4.17 m/s and for the affected limb was 50.91±4.30 m/s. The SNCV obtained for both the limbs was within normal ranges. The normal value of SNCV of the peroneal nerve ranges from 41 to 60 m/s [25]. When the comparison was done between the affected limb and unaffected limb, it was found that SNCV of the affected limb was marginally reduced as compared to the unaffected limb, but it was not statistically significant. It is said that SNCV is not affected in patients with lumbar radiculopathy [26]. A study done by Plastaras and Joshi (2011) has found similar results. It is said that sensory parameters remain within normal range, as the symptoms of pain are typically mediated by C–fibers, which are too small to be accessible for standard electrodiagnosis techniques. Moreover, in radiculopathy, the lesion is proximal to the dorsal root ganglion, and degeneration occurs centrally rather than peripherally [27].
In conclusion this study describes the hip angle at which symptoms are reproduced, nature and distribution of sensory responses to the neurodynamic test of peroneal nerve in patients with lumbar radiculopathy. However, the sensory nerve conduction velocity of affected limb was reduced marginally but not statistically significant as compared to unaffected limb.
This study presents several limitations. In relation to the neurodynamic test of peroneal nerve performance ankle plantarflexion and inversion were not measured in the present study that could influence the results. Another limitation is that hip flexion achieved at P1 and P2 during neurodynamic test of peroneal nerve was considered as a reflection of pain tolerance of the subjects, influenced by subject characteristics. As a result, the willingness to endure more pain before calling the test off could have influenced the results. Finally, Nerve conduction velocity is an expensive electrodiagnostic investigation. Further studies are needed to evaluate the sensory responses of sciatic, tibial and sural nerves to check whether the similar responses are seen in patients with lumbar radiculopathy. The results of this study suggests that neurodynamic test of peroneal nerve and nerve conduction velocity should be incorporated while assessing the patients with lumbar radiculopathy in clinical practice. This data will help in clinical evaluation and effective treatment of patients with lumbar radiculopathy.
Conflict of interest
The authors have no conflict of interest to report.