
Abstract
BACKGROUND:
Physical activity plays an important role in management and preventing complications of type 2 diabetes mellitus (DM). Effectiveness of Pilates on DM showed that there was improvement in glucose control. Presently, resistance training forms are becoming very popular for weight loss and DM. Calisthenics is a relatively new form of resistance exercise training that has been less studied in obese and diabetic individuals.
STUDY PURPOSE:
To evaluate and compare the effect of Calisthenics and Pilates training approaches on percentage body fat and glycemic control (HbA1C, Post Prandial Blood Glucose (PPBG)) in overweight individuals with type 2 Diabetes mellitus (DM).
METHODS:
Thirty (n = 30) over weight individuals with type 2 DM with HbA1C levels >6.5% were recruited for the study. The participants were randomly allocated to calisthenics (CG) and Pilates (PG) study groups who received respective exercise interventions for 12 weeks. The outcome measures were HbA1C, PPBG and percentage body fat assessed at pre and post intervention.
RESULTS:
Both CG and PG study groups showed statistically significant difference for glycemic control (HbA1C, PPBG) post 12 week intervention. However, significant improvement was noted in CG than PG in terms of HbA1c (p = 0.03), PPBG (P = 0.01) and body fat percentage (p < 0.0001).
CONCLUSION:
Calisthenics exercise training was more effective than the Pilates training in achieving long term (HbA1c) and post meal (PPBS) glycemic control with significant reduction in body fat percentage in overweight individuals with type 2 DM.
Introduction
Diabetes Mellitus (DM) is a heterogeneous condition categorized by hyperglycemia as a result of impaired secretion of insulin or body’s inability to use it effectively [1]. The American Diabetes Association defines DM as, “A condition characterized by high blood sugar levels caused by either lack of insulin or the body’s inability to use insulin efficiently” [2]. In 2020, World Health Organization (WHO) report suggests that among people diagnosed with DM, 422 million have Type 2 DM [3].
The etiology of Type 2 DM is believed to be multifactorial. Many individual-level, non-modifiable risk factors like genetic, age, ethnicity, and family history have been prospectively associated with type 2 DM. But the increase in prevalence in most populations has been driven by modifiable risk factors including sedentary lifestyle and/or lack of exercise, increased prevalence of overweight/obesity, unhealthy habits (smoking and alcohol abuse), mental stress and short sleep duration [4].
The prevalence of diabetes in India has risen from 7.1% in 2009 to 8.9% in 2019 [4]. According to a study done in 2017, prevalence of type 2 DM in the rural population was found to be 8.03% with higher prevalence during 5th decade of life and females (9.91%) were more prevalent than males (6.79%) [5]. Prevalence of men and women living with overweight/obesity having type 2 DM were observed to be 38.4% and 36.2% respectively [6].
Physical activity plays an important role in management and preventing complications of type 2 DM. The benefits of physical activity include increase in blood flow which enhances glucose uptake and reduction in abdominal fat that promotes insulin resistance [7].
Pilates exercises, is a type of physical and mental conditioning training [8]. According to previous studies, significant improvements were noted in glucose control, flexibility and HbA1C levels. Pilates is also known to have effect on overweight individuals by improving their overall health status along with reduction in risk factors of metabolic syndrome [9–11].
Calisthenic exercises are relatively newer form of resistance training in which individuals use their own bodyweight as resistance [12]. These exercises come highly suggested as part of a fitness program because they don’t require any special tools or gear to complete, they’re affordable, accessible to everyone. In the past, this form of exercise was famous among athletes, weight trainers and body builders. Recently, this has gained lot of popularity even in patient population and has been researched in conditions like Osteoarthritis [13], obesity [14, 15], shoulder conditions [16] and back pain [17].
As per the recommendations of American College of Sports Medicine (ACSM), accumulating 150 minutes of moderate intensity or 60 minutes of vigorous intensity aerobic exercise per week is sufficient to manage type 2 DM [18]. It also recommends performing 2 to 3 non-consecutive days of resistance training per week at intensities between 50% to 80% of 1-repetition maximum and targeting all major muscle groups using a scheme of 1 to 4 sets of 8 to 15 repetitions per exercise [18].
Presently, resistance training forms are becoming very popular for weight loss as well as for DM [19, 20]. Calisthenics which is a form of resistance exercise training has been less studied in obese and diabetic individuals. Considering this, it was hypothesized to determine the efficacy of calisthenics exercises in individuals with DM type 2 with obesity on glycemic control and body fat reduction. Hence, the objective of the study was to evaluate and compare the effect of Calisthenics and Pilates training approaches on percentage body fat and glycemic control (HbA1C, Post Prandial Blood Glucose (PPBG)) in overweight individuals with type 2 DM.
Methods
The present randomized clinical trial was conducted on overweight type 2 DM individuals referred by an endocrinologist/physician in the physiotherapy outpatient department setting of a tertiary care centre. The ethical clearance was obtained by the Institutional Research Committee with approval number (KIPT/SI No.313/3.07.2019). The procedures followed during the study were in accordance with the Helsinki Declaration of 1975, as revised in 1983. The trial is prospective registered under clinical trial registry of India with trial number, CTRI/2021/01/030189. Forty (40) participants were screened out of which 10 participants were excluded as they did not meet the inclusion criteria (Fig. 1). Sample size calculated for the study was thirty based on the previous literature considering the effect size with α value 1.96 and β value 0.8416 [21].
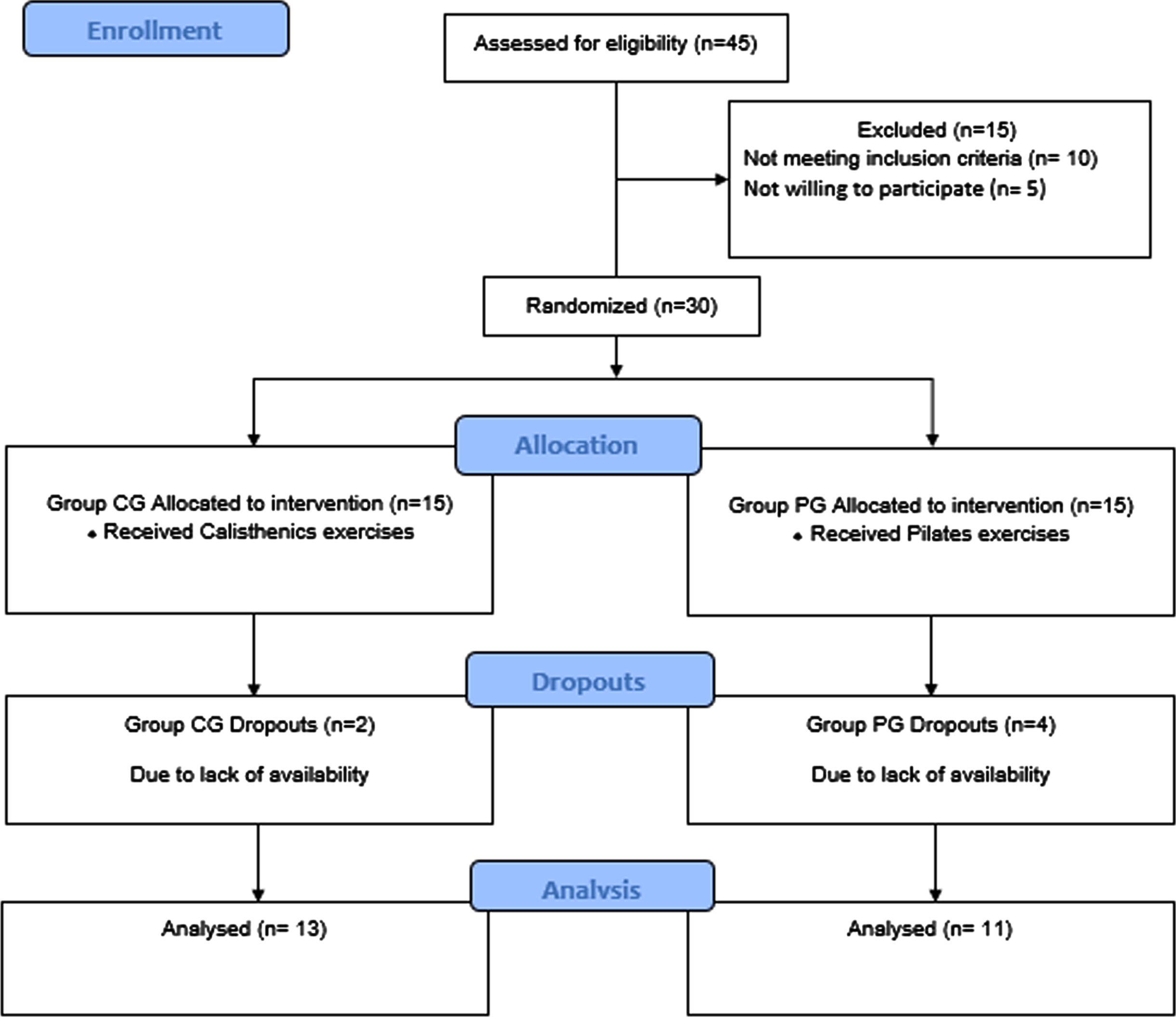
CONSORT flow diagram.
Thirty participants were randomly allocated into two groups with the help of envelop method with 15 participants each included in Callisthenic group (CG) and Pilates group (PG). Inclusion criteria was individuals aged between 30 and 65 years, diagnosed with of type2 DM with HbA1C levels >6.5% and overweight participants as defined by body mass index (BMI) >24.9 kg/m2. The participants who are involved in regular physical exercise, with severe comorbidities or complications like with cardiovascular diseases/cancers/ischemic heart disease/ neurological impairments and pregnancy were excluded from the study.
Demographic details such as age, gender, height, weight and BMI of the subjects were recorded and tabulated following which, the outcome measures including HbA1C levels and PPBG and body fat % using body composition analyser (Maltron BF 906) were noted at baseline and 12 weeks post intervention. HbA1c and PPBG investigation were carried out in a NABL approved laboratory, where the tests were carried out by a qualified pathologist. 10 ml of blood was drawn from the central vein of the arm by a certified lab technician and samples were sent to laboratory [22]. For the PPBS levels, blood test was done 2 hours after the breakfast to check the concentration of glucose levels in blood post meal [22]. Body composition for body fat percentage was done using Matron bioimpedance apparatus, model BF-906 manufactured from Maltron, UK, based on the bioelectric impedance analysis. In this method, the placement of adhesive electrodes in silver solution gel were as follows: right foot, the distal electrode at middle toe base and proximal electrode between middle and side malleoli, and for the right hand, the distal electrode on middle finger base and proximal electrode matching styloid process. Above 5-cm distance was kept between electrodes, with the subject lying supine with right foot and hand slightly apart from the body and an electric current was passed through the body and the resistance the tissue applies to this current was measured [23].
Procedure for intervention
The exercise intervention: Both the groups received intervention twice weekly for 12 weeks which were performed under supervision in the physiotherapy outpatient department by a qualified physiotherapist and then the patients were asked to continue the same exercises at home for remaining three days of the week.
Each session was of 45 minutes including warm up exercises for 10 minutes, followed by 30 minutes of callisthenic exercises/ Pilates exercises respectively and cool down exercise of 5 minutes. In warm up, the participants were made to walk on treadmill at 5 km/hour for 5 minute with 0% elevation in both CG and PG. In cool down exercises the patients received stretching exercises for trapezius, triceps, forearm flexors and extensors, hamstring, quadriceps and TA with 30 sec hold each in both the CG and PG.
Along with the physiotherapy intervention, the participants in both the groups continued undertaking the oral hypoglycemic drugs and low carbohydrate-low fat diet as prescribed by the physician.
Calisthenics Group (CG) (n = 15): Table 1 presents with the details of the calisthenics exercises prescribed as per the frequency, intensity, time and type of exercise along with progression. The participant was explained about the calisthenic exercises on the first session. The difficulty level of exercises was increased with every session by increasing the number of repetitions and by adding a new set of exercises (Fig. 2).

Calisthenics exercises.
Exercise chart
reps: repetitions; sec: seconds.
Pilates Group (PG) (n = 15): Table 1 presents with the details of the Pilates exercises prescribed as per the frequency, intensity, time and type of exercise along with progression. The participants were explained about the basic principles of Pilates exercises on the first day. Each session a new set of exercises was added along with the previously taught exercises (Fig. 3).

Pilates exercises.
Dosage: In both the groups, the intervention was given for 2 days /week for 12 weeks. Each session was of 50 mins including 5 minutes warm-up exercises, followed by basic callisthenic exercise /Pilates training respectively for 40 minutes and cool-down for 5 minutes in each supervised exercise session.
Statistical analysis was done using SPSS version 23. For this purpose, the data was entered into an excel spreadsheet, tabulated and subjected to statistical analysis. Data were summarized as mean±standard deviation for continuous variables. The between group analysis was done using paired t-test. The within group analysis was done using independent t-test. The p-value <0.05 was considered as statistically significant.
Results
All the demographic characteristics were compared between the two groups and there was no statistical significance observed indicating homogenous group characteristics (Table 2).
Demographic characteristics of participants
Demographic characteristics of participants
Kgs: kilograms; cms: centimeters.
In the CG, the mean HbA1c and PPBG values significantly decreased from baseline to post-intervention at 12 weeks (p < 0.0001). Similarly, in the PG also all the outcomes showed significant changes from pre to post intervention timelines (p < 0.0001). The mean body fat percentage value at baseline significantly decreased in the CG (p = 0.001) as well as PG (p < 0.0001) at post intervention 12 weeks (Table 3).
Comparison of pre and Post values in Calisthenics & Pilates group#
*Statistical significance (p < 0.05); # Paired t test; SD: Standard Deviation; HbA1c: Hemoglobin A1C; PPBG: Post Prandial Blood Glucose; % : percentage.
The between group analysis showed statistically significant reduction in HbA1c levels with mean difference of 2.42±0.52 in CG and 1.64+0.35 in PG, suggesting after the intervention CG had a greater reduction in HbA1c levels as compared to PG (p < 0.03).Similarly, the mean difference for PPBG in the CG was 32.23+11.94 and PG was 29.18+4.27 with CG being superior to PG (p = 0.01).When comparing the mean difference for body fat percentage in the CG (5.84+1.21) and PG (2.64+0.57), the results indicate that CG displayed greater fat reduction than PG with 95% confidence interval (p < 0.0001) (Table 4; Graph). Thus, it can be inferred that Calisthenics training is superior to Pilates training in terms of better glycemic control and fat reduction.
Graph: Graphical representation of between group comparison of pre and post value.

Between group comparison for outcomes#
*Statistical significance (p < 0.05); #Independent t test; HbA1c: Hemoglobin A1C; PPBG: Post Prandial Blood Glucose; % : percentage.
The present randomized clinical trial was conducted to compare the effect of 12-week Calisthenic exercises and Pilates training in overweight type 2 DM individuals on glycemic control (HbA1C, post PPBG) and percentage of body fat assessed at baseline and post intervention. The results of this study support alternative hypothesis since CG was better than the PG in terms of long term and post meal glycemic control and body fat reduction in overweight Type2 DM.
In the current study, post 12 weeks of intervention Pilate’s group showed improvement in glycemic control evaluated by glycated hemoglobin and post meal blood glucose levels. It can be attributed to the enhancement of insulin sensitivity with increased muscle GLUT-4 expression which is a conceivable mechanism connected with the working of Pilates [18, 24]. Various studies have also shown beneficial effects of Pilates on blood glucose regulation, that occur through AMP-activated protein kinase which is a probable key signaling intermediary in the regulation of exercise-induced changes in glucose and subsequent translocation of GLUT-4, where blood glucose uptake happens regardless of insulin action due to a cascade of intracellular processes [25, 26]. A study done on Pilates training significantly reduced the postprandial blood glucose level and HbA1c levels by 20–30% which is in accordance to findings in our current study [27]. A systematic review done in 2021, on effect of Pilates in glucose and lipids found that Pilates combined with medications and dietary treatments has a greater reduction in PPBG and HbA1C in individuals with DM [28]. Pilates intervention also resulted in significant reduction of body fat percentage in the present study. Our results supported the other studies carried out on overweight and obese population [29, 30]. A study by Raziye et al. supports the positive impact of Pilates on various body composition parameters including body fat percentage. This study also maintained the patients on a low carb diet along with the intervention [31]. The possible reasoning behind the benefits of reduction of body fat could be due to the sufficient training stimuli provided during the Pilates intervention as literature states that intervention types required for positive change on body composition for energy expenditure were defined as 60 minutes, 5 times/week (intervention type I), which is consistent with the intervention given in the present study [32].
The results of the present study demonstrated significant improvement in values of glycated hemoglobin and PPBG with calisthenics training. Calisthenics exercises are a type of resistance exercises in which we use one’s body weight to perform the exercises. Since there is lack of supporting evidence where calisthenics are prescribed for overweight diabetic individuals, calisthenics can be compared to resistance exercise forms for its effect as calisthenics is a form of resistance training. Several studies have proven for resistance training to have a positive effect on reducing the HbA1C and post prandial blood glucose levels [20, 33, 34]. The possible reasoning behind these findings could be explained by: firstly, as resistance training significantly improves muscle mass, overall cross-sectional area of muscle and oxygen uptake, it has proved to have a positive effect on glycemic control due to increased capillary to muscle fiber ratio and increased storage of glycogen which can be associated in the reduction of HbA1c levels seen in our intervention of callisthenic training [12]. Secondly, previous research has found that resistance exercises alter metabolic activity by increasing heat production and oxygen consumption in skeletal muscles [35]. These exercises can improve the insulin-signaling system by increasing protein kinase B expression. This further regulates GLUT-4 activity, resulting in increased translocation at the cellular level [33, 36, 37]. Finally, as muscle strength, bone mineral density and lean body mass significantly improves after resistance exercises, it enhances the insulin-mediated glucose uptake in skeletal musculature and also increases the capacity of these muscles to oxidize fat and glucose in the postprandial state [38]. This might explain the mechanism behind the reduction in post-prandial glucose levels following callisthenic exercises.
Callisthenic exercises demonstrated a significant reduction in body fat in the present study. This finding has been supported by various studies conducted in the past [39, 40]. The reduction in fat can be explained by the fact that these exercises induce specific adaptations required for high intensity exercise training that resulted in reduction of body fat. Another study stated that following resistance training program there is improvement in muscle hypertrophy that helps in accelerating the basal metabolism [41], which is positively correlated with lean body mass, thereby decreasing the percentage of body fat [42].
When comparing between both the intervention groups, Callisthenic exercises proved to be more effective in reducing HbA1c levels, post prandial blood glucose levels and body fat percentage as compared to Pilates exercises in overweight individuals with type 2 DM. Calisthenics exercises involves whole-body strengthening, targeting major muscle groups of the body whereas, the Pilates exercises are core targeted exercises focusing on core muscle strengthening which could be the reason as to the superior effect seen in the callisthenic group.
Literature review suggested no studies comparing resistance training with Pilates training on glycemic control. However, a study compared core resistance training over Pilates on balance and body composition parameters which reported core resistance training to be more effective than conventional Pilates training [43]. The combined effect of brisk walking had a greater effect over only Pilates training on blood glucose level among middle-aged women [44]. The effect of eight-week cyclic exercises and Pilates exercises in women on blood lipids found both the exercises to have the same effect [45].
A meta-analysis done in 2021 on effectiveness of resistance training in patients at risk for type 2 DM showed significant reductions in HbA1c in individuals undergoing resistance training compared to the control group, demonstrating the potential of resistance exercises to improve glycemic control and prevent hyperglycemia-associated complications [46]. These results are consistent with a number of previous reports of resistance training compared with aerobic training / passive stretching/ control groups decreasing HbA1c in those with Type 2 DM [33, 47, 48].
Moreover, the current study showed that effects of calisthenics in terms of body fat percentage was highly significant than Pilates group. A study was done to compare calisthenics versus Yogasana Pilates exercises among metabolic syndrome diagnosed individuals and showed calisthenics to be more effective in reducing body fat percent than Pilates exercises [49]. The superior effect seen in calisthenic group can be attributed to moderate intensity resistance exercise training program. A study evaluated the effectiveness of moderate intensity training on the body composition parameters in overweight females concluded that there was significant reduction seen in body fat mass following moderate intensity resistance exercise program [50].
The study had a few limitations which include higher drop outs due to the ongoing COVID-19 pandemic. Due to the pandemic, less number of supervised sessions and more home exercise sessions were given so as to reduce the exposure. Diet was not monitored for compliance. However, they were advised to follow the dietary modifications as advised by their physician/endocrinologist/dietician. In further studies, controlled trials comparing different exercise intervention can be considered. Standard outcome measures like Dual energy x-ray absorptiometry can be used for better evaluation of body composition.
Conclusion
In conclusion, although both interventions (Calisthenics & Pilates) were effective at 12 weeks, Calisthenics training had superior effect than the Pilates training protocol in reducing the glycated Hemoglobin value for glycemic control (HbA1C), post meal blood glucose levels (PPBG) and body fat percentage in overweight individuals with type 2 DM.
Footnotes
Acknowledgments
We thank Prof. Dr. Javali for helping us with statistical analysis.
Conflict of interest
The authors have no conflict of interest to report.
Funding
Self-Funded.