
Abstract
OBJECTIVE:
To evaluate the literature on children and young people with symptomatic hypermobility using a developmental framework.
METHODS:
A search was conducted in EMBASE, Medline, CINAHL, Web of Science and grey literature. Full text articles reporting children and young people (birth to 24 years) with a confirmed diagnosis of symptomatic hypermobility (including Hypermobility Spectrum Disorder or hypermobile Ehlers-Danlos syndrome) using internationally recognised criteria or equivalent diagnoses were included. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews methodology was followed.
RESULTS:
Of the 1619 studies screened, 163 were included in the scoping review. Studies were published from 1967-2021, 30% were narrative reviews and 24% were case reports, from a range of journals. Musculoskeletal and cutaneous characteristics were common in all developmental stages. Cardiovascular characteristics including autonomic dysfunction, fatigue, and gastrointestinal issues were reported more frequently by adolescents. Young adult studies were scarce and included mostly case reports. Varied diagnostic criteria and assessment methods were identified. The Beighton Score was frequently used (93%), but rarely standardised (12%) and lacked consensus regarding the cut-off point of hypermobility.
CONCLUSIONS:
This novel systematic scoping review identifies the changing phenotype of symptomatic hypermobility from childhood to adolescence, and the unique stage of young adulthood. There is a lack of guidance regarding the utilisation of standardised tools to assess hypermobility in clinical practice and research. Numerous and inconsistent diagnostic criteria and assessment methods limit the data analysis. Case control and longitudinal studies using defined, bespoke criteria and assessments are needed.
Introduction
Joint hypermobility (JH) is present when a joint actively or passively moves beyond its normal range of movement [1]. It is not a diagnosis but describes a continuum and varies with age, requiring clinicians to take age-related normative data into consideration [1]. A recent systematic review reported prevalence rates of between 3.3%–65% [2]. JH also varies with gender, ethnicity, strength training, or previous injuries, which further challenges the clinician [2, 3]. JH may be present at a few joints or many which is termed generalised JH. It is often screened using the Beighton score, which is validated in children using a standardised protocol [4–6].
The terminology used to define JH with symptoms is variable and controversial. Terms used include Hypermobility Syndrome and Joint Hypermobility Syndrome (JHS), thought to be overlapping with Ehlers-Danlos type 3 (EDS type III) and Ehlers-Danlos syndrome hypermobility type (EDS-HT) [7]. In 2017, new nosology was developed by international consensus and the term ‘hypermobile Ehlers-Danlos syndrome (hEDS)’ and ‘Hypermobility spectrum disorder (HSD)’ were proposed [3, 8]. Recent guidelines from the British Society for Adolescent and Paediatric Rheumatology (BSPAR) use the term ‘symptomatic hypermobility’ to define symptoms understood to be related to being hypermobile [9]. The term ‘symptomatic hypermobility’ will be used in this review as an overarching term. Children and young people are defined as those from birth to 24 years of age [10].
While the association of JH with musculoskeletal symptoms was first described by rheumatologist Kirk and colleagues in 1967 [11] other symptoms, including functional gastrointestinal disorders [12], fatigue [13], cardiovascular dysautonomia [14] and headaches [15] have since been reported. The diagnosis of symptomatic hypermobility in children and young people is a clinical diagnosis of exclusion as no specific gene has been linked to HSD or hEDS [1] and there is no specific diagnostic test. Assessments must be interpreted in the context of normal variants and symptoms, such as pain [16, 17], that may be common in the general paediatric population [18].
The literature uses varied terminology, spans medical domains and settings, and includes adult and paediatric populations [19], making its interpretation difficult. This scoping review aims to systematically explore and summarise the literature reporting symptomatic hypermobility in children and young people. The objectives are to report (i) study designs and settings; (ii) population characteristics; (iii) diagnostic criteria and measurement approaches and (iv) to identify clinical characteristics in the context of developmental stages (childhood (0-9years), adolescence (10-19years), and young adulthood (20-24years)). Using a developmental framework, this review will provide clarity for clinicians and researchers assessing and managing patients.
Methods
A systematic scoping review (ScR) approach was used to identify and map the available evidence using an established framework [20], that was updated [21] and further clarified [22]. The research was systematically reviewed, and results presented descriptively.
Protocol and registration
The ScR protocol [23] was written using the PRISMA Extension for Scoping Reviews (PRISMA-ScR) and was registered with the Open Science Framework on 20th September 2021 (https://osf.io/m2h6q).
Search Strategy. Search conducted on 01/12/20. Number of results from all searches = 4168. After deduplication = 1619
Search Strategy. Search conducted on 01/12/20. Number of results from all searches = 4168. After deduplication = 1619
The Joanna Briggs institute recommended framework Population, Concept and Context (PCC) was used to formulate the research question and determine the inclusion and exclusion criteria [20]. This review was guided by the research question “What are the presenting clinical characteristics of children and young people diagnosed with symptomatic hypermobility (including HSD and hEDS and other equivalent diagnoses)?” Literature on children and young people, with a clinical diagnosis of symptomatic hypermobility, HSD, hEDS or equivalent diagnoses (EDS-HT, EDS type III and JHS) using internationally recognised criteria was included. Randomised and non-randomised controlled trials, intervention, observational studies and case reports were included. Review articles were also included when they met the inclusion criteria and captured data not seen in original articles. Bibliographies of included papers were hand searched to capture previously unidentified studies [22]. Editorials, opinion papers, abstracts, posters and papers not in the English language were excluded.
Search strategy
A systematic search was carried out from inception to June 2021. Specific search terms for each database were used so that historical articles, including seminal papers, would be included. The search strategy was drafted by an experienced subject librarian (DM) using Boolean Operators across the Cumulative Index of Nursing and Allied Health Literature, PubMed, Embase and Web of Science (Table 1). Grey literature and targeted websites were manually searched (www.opengrey.eu; www.ehlers-danlos.com; www.hedstogether.com; www.hypermobility.org). The Google search engine (www.google.com) was searched without date restriction. The first 20 hits were screened. Review articles references were hand searched to identify papers not yet captured. The final search was uploaded into Endnote and duplicates removed.
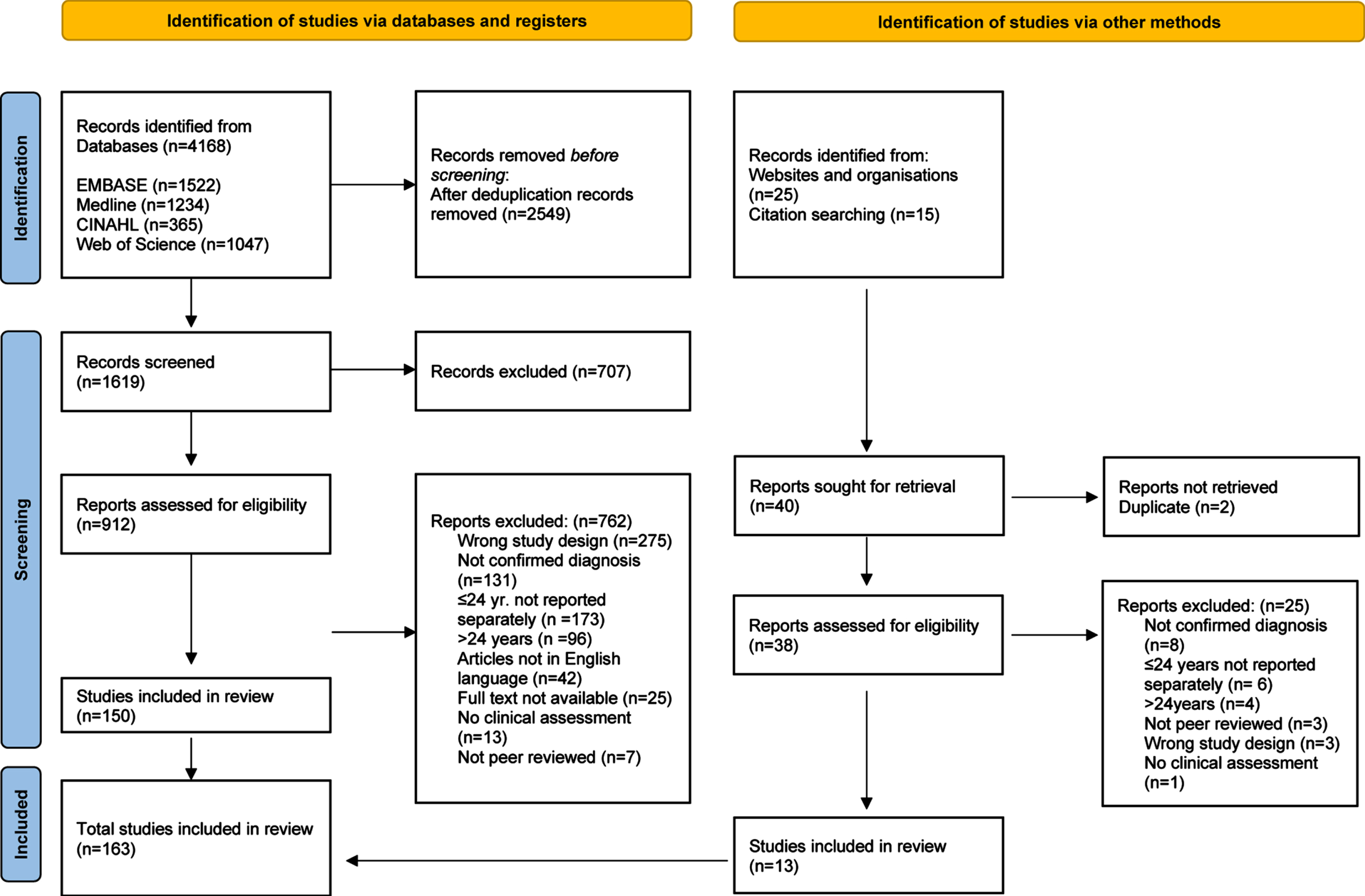
PRISMA-ScR flow diagram of study selection process.
Papers were uploaded to Covidence software, 2016 (www.covidence.org). Title and abstract screening and full text reviewing were conducted by two independent reviewers (SW and SD). Inter-rater reliability was tested at both title and abstract and full text stages to substantial agreement (Cohen’s Kappa = 0.7) [24]. Any disagreements regarding interpretation of the criteria were discussed with the research team and clarified. Conflicts following each stage were resolved with a third independent reviewer (JD).
Data charting process
Data extraction templates for empirical studies (author, year, country, participants, methods, relevant findings), narrative reviews (author, year, diagnostic criteria, relevant findings) and systematic reviews (author, year, number of studies, relevant findings) were created. These were later categorised into clinical domains, and where possible, developmental stage. A pilot data extraction was conducted with 20 randomly selected articles between two independent reviewers (SW and SD). When consensus was achieved, one reviewer (SW) completed the data extraction process [21]. Principal authors were contacted if there was missing data, or where further information was required.
Results
The original search generated 4168 papers. Following deduplication, 1619 titles and abstracts were screened, and 912 full text articles were reviewed of which 150 were included in the analysis. An extended search was carried out in June 2021 and yielded a further 13 papers. The study selection process is presented as a PRISMA-ScR flow diagram (Fig. 1). In total, 163 papers were included in the scoping review and summaries of all papers, categorized by study design are presented in Appendices 1, 2 and 3.
Context
Publication dates spanned from 1967 to 2021, with 74% (n = 120) of papers dating from 2010. Journal types spanned over 25 different clinical domains including medical, surgical, psychosocial, general and specialised topics. Empirical studies (n = 108) were conducted in 26 different countries, but nearly 50% were carried out in the US (29%) or UK (20%). Italy had the most publications in Europe (9%). There was only one international collaboration, [25] and only one systematic review specific to children, but it included only two papers [26]. Of the empirical studies, 94% (n = 101) were conducted in clinical sites, mostly in specialist settings, and 6% (n = 7) were conducted in school settings. In total n = 4444 participants were included (children n = 847; adolescents n = 2553; young adults n = 50; not specified n = 994). Although critical analysis of studies was not performed [27], study designs were plotted in terms of levels of evidence. Using a simple hierarchical approach [20], study designs were predominantly of a lower level of evidence with narrative/literature reviews and case series/reports accounting for 88 (54%) of the included studies (Table 2).
Studies by study design and date of publication
Studies by study design and date of publication
Diagnostic criteria used to define symptomatic hypermobility varied. Early studies reported children who presented to rheumatology clinics with ‘musculoskeletal complaints which at the time were considered due to generalised joint laxity’ [11] or were ‘subsequently determined to have hypermobility’ as a basis for their symptoms [28]. Later studies referred to specific criteria, revised at time points over decades [29]. However, studies often differed in their interpretation of symptomatic hypermobility, for example, ‘arthralgia for three preceding months or more’ [30], ‘presence of JH and musculoskeletal pain’ [31], ‘lower limb pain and/or fatigue in the previous 4 weeks’ [32], ‘presence of multiple joint pain’ [33], and ‘musculoskeletal symptoms (arthralgia in 2 joints for 12 weeks), exercise induced pain and exercise intolerance’ [34].
Measurement approaches
More than 75 different measurement approaches were reported across 15 different clinical domains (Table 3). Hypermobility screening assessments were reported in 62% (n = 101) of studies. Of these, the Beighton score was most commonly used (93%, n = 94), however only 12 studies reported evidence of standardisation (goniometry or standardised positioning). Additionally, the cut-off point to determine presence of JH, was not consistent, as Beighton scores of 4 [15, 35–37], 5 [38], and 6 [32, 39] were reported.
Measurement approaches reported in studies on children and young people with symptomatic hypermobility
Measurement approaches reported in studies on children and young people with symptomatic hypermobility
MSP Musculoskeletal Pain, VAS Pain Visual Analogue Scale, NRS Pain Numerical Rating Scale, Peds-QL Pain Paediatric Pain Questionnaire, BAPQ Bath Adolescent Pain Questionnaire, PFSD Pain-Frequency-Severity-Duration Scale; CMAS Childhood Myositis Assessment Scale, FPI Foot Posture Index, FDI The Functional Disability Inventory, 6MWT six-minute-walk-test, YBT Y-Balance Test, BOT-2 Bruininks-Oseretsky test of motor proficiency, M-ABC Movement Assessment Battery for Children, KTK Korperkoordinationstest fur Kinder PODCI The Pediatric Outcomes Data Collection Instrument, DASH Disabilitites of the Arm, Hand and Shoulder Questionnaire, ECG Electrocardiogram, ECHO Echocardiogram, CT Computed Tomography, VCUG Voiding Cysto-Urethrogram, PEDS QL Pediatric Quality of Life Inventory, CHQ Child Health Questionnaire, BIPQ Brief illness Perception Questionnaire, FPQ Frequency of Participation Questionnaire, PAQ Physical Activity Questionnaire, PROMIS Patient-Reported Outcomes Measurement Information System, SRBD Sleep-Related Breathing Disorder Scale, ESS Epworth Sleepiness Scale.
Assessments in the musculoskeletal domain included pain (14%, n = 23) [15, 38–54] and function (9%, n = 14) [30, 55–58]. Cardiovascular assessments were reported in 12% (n = 19) papers [13, 59–75]. Other clinical domains included cutaneous, genetic, urogenital, gynaecological, and gastrointestinal. Assessments relating to quality of life were reported in 8% (n = 13) of studies [15, 76] and fatigue was assessed in 6% (n = 9) of studies [13, 77].

Studies reporting clinical characteristics for each developmental stage.
Of the 108 empirical studies, only 89 presented clinical characteristics stratified by age. Primary data were analysed with respect to developmental stage (childhood, adolescence, young adulthood) and clinical domain. A summary of findings is presented in Fig. 2.
Clinical characteristics in children were reported in 16 studies [53, 95–100]. Musculoskeletal characteristics were reported in 75% (n = 12) of these studies, including pain [53, 100], exercise-induced pain [75], myalgia [71], and arthralgia [75]. Other characteristics included hyperextensible joints [79, 98], joint subluxations [79], reduced balance [57], low muscle tone [57], unstable gait [99], weakness [55], and decreased exercise capacity and participation in exercise compared to peers [55]. Cutaneous features were reported in 31% (n = 5) studies. Reports included unusually soft or velvety skin [72, 100], skin extensibility [75, 79], and easy bruising [79]. Three studies reported neurodevelopmental features including gross motor delay [100], co-ordination difficulties [53] or gross and fine motor, social and literacy problems [83]. Two studies reported cardiovascular clinical characteristics: aortic root dilatation and mitral valve prolapse [71, 72]. Two studies reported fatigue [57, 100]. One of these studies, a large retrospective review (n = 318), found 89% of participants reported a ‘sense of fatigue during or after activity’[100].
Adolescence
Clinical characteristics in adolescents were reported in 54 studies [13, 101–117]. Musculoskeletal characteristics were reported in 85% (n = 46) of studies and included, chronic recurrent pain [34, 118] and joint instability, sprains and dislocations [42, 118]. Clinical characteristics from the cardiovascular domain were reported in 37% (n = 20) of studies, including valve prolapse and greater aortic root [59, 89] and dysautonomia including orthostatic intolerance [13, 117]. Cutaneous features were reported in 35% (n = 20) studies [13, 119] notably easy bruising [40, 76], hyperextensibility [64, 89], soft velvety skin [87, 108], delayed wound healing, easy scarring [35, 87], and striae [101]. Fatigue was reported in 24% (n = 13) of papers [13, 118]. Gastrointestinal characteristics were reported in 22%, n = 12 [15, 118]. Clinical characteristics included chronic gastritis [118], constipation [78], recurrent abdominal pain and chronic diarrhoea [35, 87], and vomiting [52]. Urogenital features were reported in 15% (n = 8) [15, 110] including primary nocturnal enuresis and daytime symptoms of urinary urgency [64]. Sleep disorders were reported in 11% (n = 6) of studies [52, 110] including insomnia [52, 54], obstructive sleep apnoea, circadian rhythm disorders, periodic limb movement disorder, and hypersomnia [54, 94]. Psychosocial features were reported in 11% (n = 6) of studies [15, 104]. Characteristics included anxiety and depression [15, 104] and eating disorders [104]. Neurodevelopmental characteristics were reported in 7% of studies [78, 110] including relatively higher rates of learning difficulties, dyslexia and dyspraxia [78] and an association between neuropsychiatric conditions, such as attention deficit hyperactivity disorder (ADHD) and children diagnosed with HDS and hEDS [110].
Young adulthood
Nineteen studies included participants between 20 and 24 years [37, 120–131]. Musculoskeletal characteristics were reported in 95% (n = 18) of studies, with the exception of one study [85]. Characteristics included arthralgia [41, 128], joint instability, dislocation [43, 128] and reduced dynamic balance [37]. Cutaneous features were reported in 42% (n = 8) of studies [41, 130]. Characteristics included easy bruising [41, 92], soft skin [129] and striae [130]. Psychological features were reported in 26% (n = 5) of studies [41, 129] including depression [80, 129] and anxiety [125]. Gastrointestinal characteristics were reported in 21% (n = 4) of studies, all of which were single case reports [41, 128]. Two studies reported urogenital characteristics: stress incontinence and dysuria [80, 128].
Discussion
This is the first scoping review to explore the literature on children and young people with symptomatic hypermobility with a unique focus on developmental context. This review systematically clarified and interpreted the considerable quantity of diverse literature to make it more accessible to researchers and clinicians. Research on those with symptomatic hypermobility was more prolific in the last 12 years, extends over many different clinical domains, and consists largely of narrative reviews and case studies. The level of evidence of the literature on symptomatic hypermobility is predominantly of a lower hierarchy [132]. Case reports and series may represent more extreme clinical cases but were included due to the objectives of this scoping review to explore the full extent of the literature. The Beighton score was the most commonly used tool to screen for hypermobility, but there were limited details regarding how it was used. Similarities and differences in the presenting clinical characteristics across the developmental stages were identified.
This review found that musculoskeletal symptoms are the most prevalent clinical characteristics, and akin to cutaneous features, were reported across all developmental stages. Neurodevelopmental clinical characteristics were more common in children [53, 100]. In adolescents, dysautonomia, fatigue, sleep issues, and symptoms from urogenital and gastrointestinal domains were reported more frequently. Dysautonomia is also common in those with chronic functional pain conditions and might not be a primary indicator of symptomatic hypermobility [16, 63]. The onset of puberty was reported to be associated with a worsening of symptoms in only one study [93]. Of interest, psychological characteristics such as anxiety and depression were reported in over a quarter of all young adult studies [41, 129].
Despite the Beighton score being commonly used (n = 94), evidence of reporting of standardisation (positioning or goniometry) was documented in only 12 studies. This affects our confidence interpreting prevalence of hypermobility across different studies. A further issue of concern is that different Beighton score cut-off points were used. A large UK population study (n = 6,022) using a Beighton score cut-off point of 4/9 reported a high prevalence of hypermobility in girls (27.5%) and boys (10.6%) [133], while a study of Danish school children using a cut-off point of 6/9 resulted in a lower prevalence (9.4%) [95]. A standardised Beighton protocol has been proposed and validated in school-aged children [6] but only reported in one study in this review [57]. Barriers to its use may be a lack of awareness, equipment, or time. However, in order to accurately assess joint hypermobility, to avoid over or under diagnosis, the utilisation of standardised tools using validated protocols in clinical practice and research isessential.
Seven different assessments of function, and 11 different assessments of motor control were identified in this review. Assessments to determine cutaneous features appear to be mostly subjective. There were six different types of cardiovascular assessments, including use of echocardiography, which was recently investigated in a retrospective chart review of paediatric patients with a diagnosis of some type of EDS [69]. Authors report substantial use of echocardiography in patients with suspected hEDS but found that once other genetic conditions were ruled out, children with hEDS did not have significant aortic disease, and mitral valve prolapse occurred at the same incidence as the general population [69]. The variety of reported assessments for children and young people with symptomatic hypermobility may reflect the growing awareness of clinicians regarding the spectrum of symptoms. However, it also reflects the lack of guidance and use of specific standardised outcome measures. Additionally, it limits comparisons between studies.
Previous studies have suggested that there is a changing phenotype, characterised by a progressive worsening from childhood to adulthood [134]. One of only two longitudinal cohort studies identified in this review reported that an increased incidence of multisystem complaints was more predictive of functional decline [35]. This ScR categorised clinical characteristics according to specific developmental stages, comprehensively reporting evidence of a changing clinical presentation. However, to advance our understanding of children and young people with symptomatic hypermobility, future well-designed case control and longitudinal cohort study designs are required to observe such clinical characteristics that develop and/or change with age, so that health care professionals will be able to offer them optimum care over their lifespan.
Unlike systematic reviews, scoping reviews can be used when literature exhibits a heterogenous nature which is not as amenable to a systematic review [36]. The broad systematic search strategy was conducted by an experienced librarian and guided by expert clinicians and research team members with expertise across clinical and research spheres. There was an attempt to reduce some of the methodological heterogeneity by scrutinising literature, in particular the definitions of diagnosed symptomatic hypermobility, to ensure that studies of children with asymptomatic hypermobility were not included. Extraction of data for participants who were 24yrs presented significant challenges in the review and there were studies whereby data could not be extracted, which could be seen as a limitation.
Conclusion
This review presents a synthesis of the diverse research on symptomatic hypermobility in children and young people in a developmental context. Given the changing temporal pattern of symptoms, longitudinal studies and large case control studies are warranted to provide better understanding of symptomatic hypermobility in this population. Such studies should have bespoke criteria and use standardised assessment protocols so that findings from different studies can be compared and data can be pooled for analysis.
The comprehensive reporting of symptoms, extending beyond the musculoskeletal system into wide-ranging clinical domains presents the consideration of alternative care pathways for children and young people, whereby not all require referral to traditional settings of tertiary rheumatology and genetic clinics. With clearer guidance for health care professionals, patients with clinically relevant hypermobility could be recognised earlier and managed locally, to address the broad symptomatology with appropriate support. Those who require onward assessment and referral to tertiary services could be identified. This can only be achieved if clinicians in primary and community care are guided regarding bespoke assessment and diagnostic criteria with a background knowledge of paediatric conditions which present similarly.
Author contributions
SW, SD, JD, JS and EMD conceived the study, and formulated the research question. The search strategy was drafted by DM. SW and SD conducted screening and reviewing, whilst conflicts were resolved by JD. SW and SD drafted the review. All authors were involved in the revisions to the paper and approved the final text for submission.
Conflict of interest
The authors have no conflict of interest to report.
Funding
Supported by the National Children’s Research Centre (NCRC), Dublin, Ireland (grant number –D/19/5 to SW). The NCRC has been in existence for more than 50 years and has been funded since its inception by the Children’s Health Foundation Crumlin, Dublin, Ireland. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplementary materials
Appendices 1, 2 and 3 are available in the electronic version of this article: https://dx.doi.org/10.3233/PPR-220699.