
Abstract
BACKGROUND:
Although proprioceptive impairment is observed in about half of patients with stroke and is a factor affecting functional recovery and length of hospital stay, there is a discrepancy in terms of its measurement methods between physiotherapy research and the clinical field. This study aimed to examine the concurrent validity and reliability of knee proprioception using an electrogoniometer and a mobile app in patients with stroke.
METHODS:
In this cross-sectional study, we conducted proprioception tests with an electrogoniometer (custom-made device; Unimec, Japan) and an app (Goniometer Pro; 5fuf5, Bloomfield, NJ) in 28 hospitalized patients with stroke, with an average of 11.21 days (range 2–4 days) from the onset of stroke. Threshold to detect passive motion (TDPM), TDPM+muscle tendon vibration (MTV), and joint position sense (JPS) were used for proprioception tests. These tests were performed three times each in a random order, and the intraclass correlation coefficient, correlation, and absolute reliability for the electrogoniometer and the app were analyzed.
RESULTS:
Both TDPM and TDPM+MTV measured by the electrogoniometer and the app showed high correlation and “good” to “excellent” reliability regarding the variation in measured values, indicating that the two instruments are compatible, while JPS showed “poor” to “moderate” reliability and weak correlation for the electrogoniometer and the app.
CONCLUSIONS:
In conclusion, in patients with stroke, TDPM and TDPM+MTV measurements using the Goniometer Pro app can replace measurements with an electrogoniometer.
Introduction
Proprioception is the sense of the body’s movement and position in relation to space and is indispensable for coordinated movement and motor learning required for the performance of daily activities. Proprioception originates from stretch changes in muscle spindles and cutaneous receptors and is transmitted to the brain via the dorsal column medial lemniscus pathway and spinocerebellar dorsal tracts [1, 2]. Muscle spindles, the origin of proprioception, are activated by muscle tendon vibration (MTV), which induces a kinesthetic illusion (KI) [3]. A KI is a phenomenon wherein a muscle to which MTV is applied is stretched to produce the sensation of joint motion, and when MTV is applied to the quadriceps muscle, a KI of knee flexion is produced [4]. This phenomenon indicates activity not only in the primary somatosensory cortex but also in the primary and supplementary motor cortex [5]. Therefore, we believe that sensory perception and movement are inseparable and this phenomenon can be applied in physiotherapy aimed at the recovery of physical functions.
Proprioceptive impairment, in which physical therapists specialize, appears in about 60% of patients with stroke [6]. Stroke is recognized as the second leading cause of death [7], with approximately 12 million cases per year worldwide. Interestingly, persons with proprioceptive impairment are more likely to have balance impairment and experience falls [8, 9]. Thus, such impairments in proprioception have a negative impact on functional recovery [10], independence in daily living [11], and activity participation [12]. Hence, hospital stays tend to be prolonged beyond 3 months [13]. In clinical practice, more than 90% of physical therapists recognize the importance of sensory testing and frequently use proprioception tests [14], and more than half of physical therapists want to improve proprioception tests [15]. Based on these findings, we interpret the lack of a standard clinical assessment index and physiotherapy for proprioceptive impairment as an undefined problem.
One of the reasons for this is the evidence-practice gap between clinical practice and research on proprioception tests. In clinical practice, the Nottingham Sensory Assessment and Fugl-Meyer Assessment to screen for the presence of proprioceptive impairment have low responsiveness [16–18]. Therefore, it is difficult to describe the impact of proprioceptive impairment on activities of daily living, which can easily lead to judgments biased by empirical rules [15]. On the other hand, studies have reported testing methods, such as threshold to detect passive motion (TDPM) to detect and identify passive joint motion and joint position sense (JPS) to reproduce and match joint positions [19, 20], which use measurement tools, such as an electrogoniometer and dynamometer, and three-dimensional motion analysis to determine the degree of intrinsic sensation [21–23]. These measurement tools are provide high accuracy and responsiveness on a continuous scale, but the size and cost of the equipment are barriers and difficult to reproduce in clinical practice [24]. Therefore, we wanted to investigate a method that has clinical properties while being a proprioception test with high responsiveness that can be used in physiotherapy clinical practice [25]. Part of our plan was related to the findings of Kim et al. [26] and Meric et al. [27] regarding the concurrent validity of knee JPS using a mobile app and an electrogoniometer. However, the employed JPS method memorizes the 30°, 45°, and 75° flexion positions of the knee joint and reproduces them at the ipsilateral joint. Therefore, compared with TDPM, which investigates the minimum threshold that can be recognized after the knee joint begins to move, JPS has the weakness that the threshold is unclear and may have low responsiveness.
Therefore, this study aimed to examine the concurrent validity and reliability of knee joint proprioception testing using an electrogoniometer and a mobile app in patients with stroke. Our hypothesis was that the app-based knee proprioception test would be equivalent to the electrogoniometer. This study is novel as it was a clinical study of stroke patients with fair subject selection; the concurrent validity of the app was verified based on an analog electrogoniometer, which quantitatively measures joint range of motion; TDPM and JPS were compared; and TDPM+MTV was adopted.
Methods
Design
This cross-sectional study examined the concurrent validity and reliability of an app and an electrogoniometer in proprioception tests among patients with stroke.
Participants
Characteristics of the participants with cerebral infarction at the time of the proprioception tests
Characteristics of the participants with cerebral infarction at the time of the proprioception tests
Values are mean±SD range or number; LI, lacunaer infarction; ATBI, atherothrombotic brain infarction; CE, cardiogenic cerebral embolism; ESUS, embolic stroke of undetermined source; ARWMC, Age Related White Matter Changes; NIHSS, National Institutes of Health Stroke; SSS, Scandinavian Stroke Scale; FMA-LE, Fugl-Meyer Assessment lower extremity; MAS, modified Ashworth Scale; mRS, modified Rankin Scale; MMSE, Mini-Mental State Examination; BI, Barthel Index; ROM, Joint range of motion; SLR, Straight Leg Raising.
Persons with acute to subacute cerebral infarction who were hospitalized between April and October 2021 were recruited Ohara General Hospital. The inclusion criteria were National Institutes of Health Stroke (NIHSS) score of 0, unilateral spatial neglect (determined by missing at least six items in the left or right half of the Bells test), attention disorder, and aphasia. Persons with cognitive impairment (Mini-Mental State Examination score≤24 points), impaired consciousness (Japan Coma Scale≥II digits), peripheral neuropathy, and knee joint disease (knee osteoarthritis, ligamentous damage, etc.) were excluded. The subjects were those who could not perceive the movement and position of joints over the entire range of motion, who had difficulty in sitting up, and who had a previous stroke. After screening, 28 cerebral infarction persons (16 males and 12 females) with a mean age of 70.54 years (range 44–89 years) who did not meet the exclusion criteria participated in the study. The cerebral infarction cases included 5 persons with lacunar infarction (0 right side and 5 left side), 14 with atherothrombotic brain infarction (9 right and 5 left), 5 with cardiogenic cerebral embolism (3 right and 2 left), 4 with embolic stroke of undetermined source (4 right and 0 left), and 4 with atherothrombotic stroke of undetermined source (4 right and 0 left). The number of persons with cerebral infarction who participated in the study was four (four right side and 0 left side). Table 1 shows the characteristics of the participants with cerebral infarction at the time of the proprioception tests. The proprioception tests were performed at an average of 11.21 days (range 2–34 days) after the onset of cerebral infarction.
This study was approved by the ethics committees of Iryo Sosei University and Ohara General Hospital (codes: 20–17, 231), and written informed consent was obtained from the participants in advance.
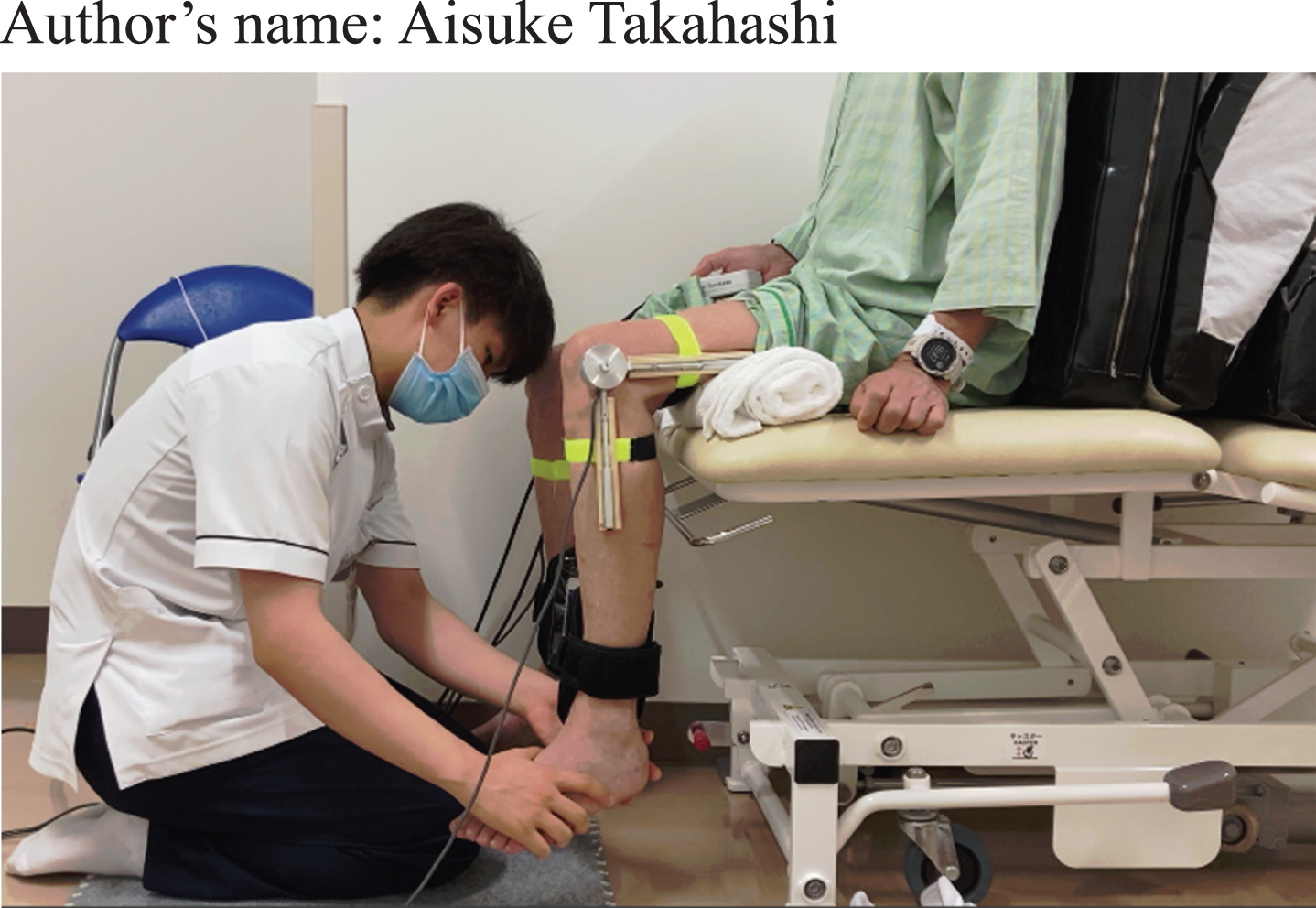
In this study, only one physical therapist with 5 years of clinical experience was used as the examiner, considering the burden on cerebral infarction persons. The participants were placed in a relaxed back-rested sitting posture with the knee joint flexed 90° and with the plantar surface of the foot raised off the floor, and an eye mask was used to block visual information. The electrogoniometer (custom-made device, sampling frequency: 100 Hz; Unimec, Japan) used to measure the knee joint angle was mounted so that the basic axis and the axis of movement were aligned and corresponded to the axis of rotation of the knee joint, in accordance with the joint range of motion display and measurement methods of the American Academy of Orthopaedic Surgeons. A versatile bioinformation analysis program (BIMTUS II, Kissei Comtec, Nagano, Japan) was used for sampling the knee joint angle via an A/D converter. In addition, Goniometer Pro (5fuf5, Bloomfield, NJ), which has been shown to have cocurrent validity with a constant velocity dynamometer [27], was used as the app. iPhone 11 (Apple, Inc., Cupertino, CA) with this app was aligned with the fibula and attached to the distal part of both lower legs with arm bands (Performance Gear, Fukushima, Japan) (Figs. 1 and 2).

Scene of measurement. A. Electrogoniometer B. iPhone11 (App: Goniometer Pro).

Goniometer Pro.
In this study, to verify the concurrent validity and reliability, the electrogoniometer and the app were used concurrently for proprioception tests. The order wherein the TDPM and JPS measurements were obtained was randomized. In addition, since it is believed that the time interval between measurements does not affect positional accuracy [28], in this study, measurements were taken three times with an interval of at least 5 s. We set up a tripod (Trail, Tokyo, Japan) 1.6 m away from the participants and took videos of these measurements with an iPhone SE device (Apple, Inc.) to confirm the results. To minimize the influence of diurnal variation in proprioception perception among subjects, all proprioception tests were conducted in the afternoon (between 16 : 00 and 17 : 00).
A pre-practice was conducted to press a switch (custom-made device; Intercross, Tokyo, Japan) synchronized with the electronic angle meter at the point where the participant first recognizes the knee joint motion by the examiner’s manipulation. Regarding the app, the TDPM knee joint angle was measured by reading the angle displayed on the app at the point where the participant pressed the switch and a sound was generated (Fig. 3).
The measurement of TDPM.
For TDPM+MTV, the examiner provided MTV to the medial hamstring with the Handy Massager MD-001 (Thrive, Osaka, Japan) while manipulating the participant’s knee joint in the same way as that for TDPM. Among the frequencies up to 120 Hz at which group Ia fibers are excited [29], a frequency of 60 Hz was set in this study. Since MTV was provided even before the knee joint movement was performed, the participants were found to press the switch before the appearance of KI in the pre-exercise period. Therefore, the participants were informed that KI may occur even before they perform the knee joint motion, and the knee joint angle at the point where the participants pressed the switch during the examiner’s manipulation was recorded.
The onset of knee joint motion in TDPM and TDPM+MTV was set at a random time interval of 5 s or longer so that participants could not predict the timing. In addition, the guided velocity of the knee joint was set to 5.00°/s as much as possible to avoid the possibility of overshoot errors at 2.50°/s and undershoot errors at 10.00°/s due to the tau effect (a change in sensory perception depending on the time of guided motion). Therefore, it was recommended that the examiner should use a manual knee joint movement rate of 5.00°/s as much as possible [30]. We conducted a preliminary analysis with healthy participants by standardizing the body part grasped by the examiner. The mean measured value was 4.99±1.02 (min-max: 2.25–7.66).
For JPS, the examiner guided the participant’s knee joints altruistically, and the participant reproduced the other knee joint angle by active motion based on the guided knee joint angle (Fig. 4). The absolute error between the reference and reproduced knee joint angle was calculated to determine the accuracy of the proprioception with respect to the reference position. Since the JPS task involves recreating the knee joint on the contralateral side based on the proprioception of the induced knee joint, the side on which the examiner induced the knee joint was designated as the “paralyzed side JPS”. In addition, the referenced knee joint angle was set at 40°, 60°, and 80°, which is near the middle of the knee joint range of motion based on previous studies on reproducibility [31], one time each for a total of three times. These joint angles were randomly presented to each participant, and the participant held the reproduced angle for 5 s.

The measurement of JPS.
Intraclass correlation coefficients (ICC) were obtained, and correlation and absolute reliability analyses were conducted to verify the concurrent validity and reliability of TDPM, TDPM+MTV, and JPS for the electrogoniometer and the app.
For the ICC model, intra-rater reliability was calculated using ICC(1.1) and ICC(1.3) and the 95% confidence intervals (95% CI) [32]. In addition, Cronbach’s alpha coefficient was used for the analysis of internal consistency. The reliability levels of ICC were interpreted as follows: less than 0.50, low; between 0.50 and 0.75, moderate; between 0.75 and 0.90, good; and above 0.90, excellent [33]. The minimum sample size was calculated as 24 (minimum acceptable ICC: 0.50, expected ICC: 0.90, significance level: α= 0.05, power: 80%, number of measurements: 3) [34].
Kendall’s (τ) and Spearman’s rank correlation coefficient (rs) were used to evaluate the correlation between angles obtained from the electronic angle meter and the app for TDPM and JPS. When τ>0.1, the data were considered to show heteroskedasticity and were log-transformed to log10. The magnitude of rs was interpreted as follows: 0.00–0.10, none; 0.10–0.39, weak; 0.40–0.69, moderate; 0.70–0.89, strong; and 0.90–1.00, very strong [35].
Regarding absolute reliability, the standard error of the mean (SEM = SD√1 – ICC) of the measurement was calculated [36]. A lower value of the SEM indicates less intra-inspector variability. Bland-Altman analysis was performed using the limits of agreement (LoA) (LoA = mean of the differences±1.96×SD of the differences) to evaluate the systematic error, which consists of proportional and fixed errors between the app and the electrogoniometer. The proportional error was calculated by correlating the data groups of the difference and the mean of the measured values of the corresponding electrogoniometer and app. Fixed errors were evaluated based on whether or not the LoA contained 0. If the LoA contained 0, it was considered that there was no significant fixed error. If no fixed error was found, the minimum detectable change (MDC) (MDC = SEM×√2×1.96) at 95% CI was calculated. If the mean difference (MD) between the measurements of the electrogoniometer and the app was lower than the MDC, the electrogoniometer and the app were considered to becompatible.
The significance level was set at p < 0.001. All data were analyzed using Microsoft Office Excel 2016 (Microsoft Corp., Redmond, WA) and SPSS version 25 (SPSS Inc., Chicago, IL).
Results
Table 2 shows the intra-rater reliabilities of TDPM, TDPM+MTV, and JPS measured with the electrogoniometer and the app. TDPM showed “good” to “excellent” reliability, with ICC(1.1) = 0.85 (95% CI: 0.75–0.92) and ICC(1.3) = 0.95 (95% CI: 0.90–0.97), for the paralysis side electrogoniometer, and showed “good” to “excellent” reliability, with ICC(1.1) = 0.88 (95% CI: 0.80–0.94) and ICC(1.3) = 0.96 (95% CI: 0.92–0.98), for the app (p < 0.001). Therefore, the app showed the same intra-rater reliability as the electrogoniometer, and the same trend was observed for TDPM+MTV. The alpha coefficients of TDPM and TDPM+MTV were greater than 0.8, indicating the tendency of internal consistency. On the other hand, JPS showed “poor” to “moderate” intra-rater reliability for both the electrogoniometer and the app (p < 0.001).
Intraclass correlation coefficients for proprioception tests measured by Electrogoniometer and App
Intraclass correlation coefficients for proprioception tests measured by Electrogoniometer and App
Values are number; ICC (95% CI), Intraclass correlation coefficients (95% Confidence Interval); TDPM, Threshold to detect passive motion; TDPM+MTV, Threshold to detect passive motion+ muscle tendon vibration; JPS, Joint Position Sense.
Table 3 shows the correlations and absolute reliability of each measurement by the electrogoniometer and the app. Regarding Spearman’s rank correlation coefficient, on the paralyzed side, TDPM had a coefficient value of 0.79 and TDPM+MTV had a coefficient value of 0.70, indicating “strong” correlation (p < 0.001). The SEM showed a difference of less than 0.1 between the electrogoniometer and the app and showed similar values between the paralyzed and non-paralyzed sides. On the other hand, JPS showed “weak” correlation, with rs = 0.32 (p > 0.001). Bland-Altman analysis showed a proportional error in JPS on the non-paralyzed side, but no fixed errors were found in all groups, and the MD showed lower values than the MDC, indicating that the agreement between the electrogoniometer and the app tended to be high (Table 3; Fig. 5). However, the accuracy of the agreement for JPS between the electrogoniometer and the app was low because JPS showed a wider LoA than the values for TDPM and TDPM+MTV. Therefore, TDPM and TDPM+MTV measured using the app showed comparable variation in measured values, although there were some differences from the values of the electrogoniometer, and the results were interchangeable.
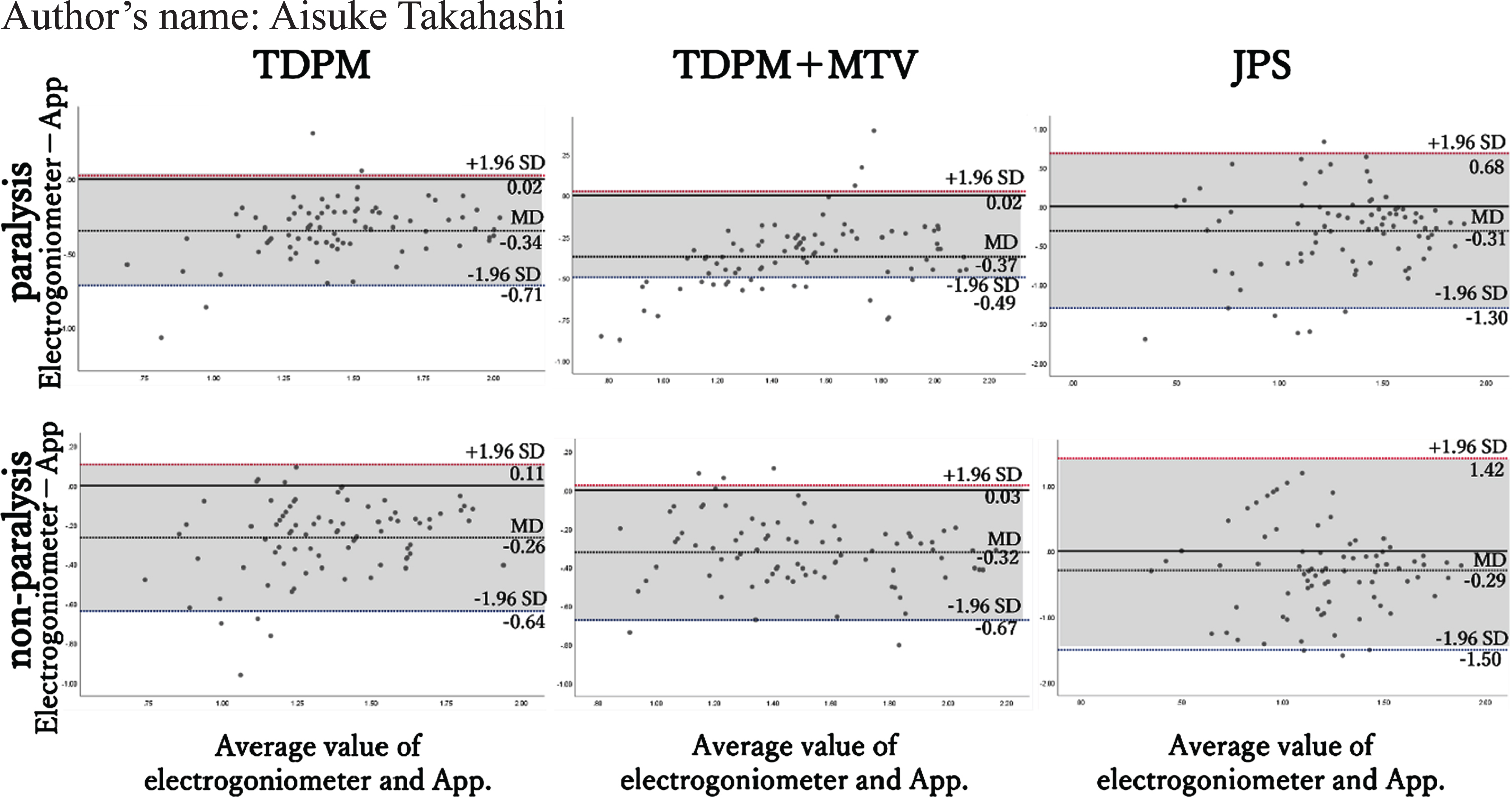
Bland-Altman plots of proprioception test using electrogoniometer and App.
Correlation and absolute reliability for proprioception tests measured by Electrogoniometer and App
Values are number; SEM, standard error of the mean; MDC, minimum detectable change; rs, Spearman’s rank correlation coefficient; MD (LoA), mean difference (limits of agreement); TDPM, Threshold to detect passive motion; TDPM + MTV, Threshold to detect passive motion + muscle tendon vibration; JPS, Joint Position Sense.
In this study, we examined the concurrent validity and reliability of knee proprioception using an electrogoniometer and an app in patients with stroke. Results showed that TDPM and TDPM+MTV measured using the app had concurrent validity with the values obtained with the electrogoniometer, which was partially consistent with our hypothesis. In clinical practice, despite the opportunity for physical therapists to provide exercise therapy with the goal of improving proprioceptive impairment in stroke patients, studies on proprioception tests (TDPM, JPS, and Active Movement Extent Discrimination Assessment for orthopedic diseases, such as anterior cruciate ligament injuries and knee osteoarthritis, have mostly been conducted [22, 37–39]. Therefore, we did not find any reports examining the clinimetric properties of TDPM or JPS with an app in stroke patients, and these results cannot be accurately compared. Factors that influence the clinimetric properties of the measurement conditions include subject and examiner factors. In terms of subject factors, the setting of the starting posture has been reported in the supine, seated, standing [40], and prone positions [31], with all showing “moderate” to “strong” inter-rater reliability. In the setting of the starting knee joint angle, TDPM has been reported at 20° and 40°and JPS has been reported at 30°, 40°, 50°, 70°, and 100° [31, 41, 42], and the intra- and inter-rater reliabilities for each angle were different. In addition, reports on examiner factors have compared the direction (flexion and extension) and velocity (2.50°/s, 5.00°/s, and 10.00°/s) of guidance for each knee joint [30, 43, 44]. Although these factors have not been standardized, in our study, we tried to unify these factors as much as possible and standardize the measurement methods, which we believe resulted in sufficient intra-rater reliability for TDPM and TDPM+MTV. Similar results have been obtained in a previous report that verified the reliability of proprioception tests using an electrogoniometer, and the authors considered that the same examiner may be able to accurately and consistently fit the electrogoniometer [40]. However, in our study, JPS showed “poor” to “moderate” intra-rater reliability and “weak correlation” in all groups, which contradicts the results of TDPM. One of the possible reasons for this is the difference in the conditions of joint angles in TDPM and JPS measurements. In this study, the participants had an Straight Leg Rising of 65.56±15.36°, range of knee extension of –3.15±4.12°, and Modified Ashworth Scale of 0.88±0.61. Although they had somewhat inflexible hamstrings, they generally had no or mild spasticity and no significant structural characteristics of the joints. In this situation, for the electrogoniometer, the TDPM of the paralyzed side was 7.64±5.64, which corresponded to about 12% of SLR and about 9% of knee joint extension range of motion. On the other hand, since the JPS knee joint angles were set at 40°, 60°, and 80° three times each, the presented joint angles were different compared with the findings for TDPM. Therefore, it is considered that the variation in the firing of muscle spindles affected proprioception, since the hamstring stretch induced by the knee joint was superior to that induced by TDPM in JPS [45]. In addition, since the reproduction method of JPS employed in this study was set to active motion, it is possible that the participant’s effort was affected by the degree of motor impairment and induced a sense of fatigue related to errors in proprioception [46]. Bland-Altman analysis showed no fixed errors in all test methods, but the app tended to provide higher readings than those obtained with the electrogoniometer. This result was similar to the finding in a previous report on the concurrent validity of proprioception testing using an app and a dynamometer in healthy subjects [27]. There are some differences between the Goniometer Pro app and the electrogoniometer. First, the app measures the angle to gravity. Second, the Appcannot display decimal point measurements. Third, there is an effect of moment arms due to differences in the attachment points of the devices. However, no systematic errors were found for TDPM and TDPM+MTV, and the ICC and SEM showed comparable values for the electrogoniometer and the app, indicating that the intra-rater reliability and variability of measurements for both were comparable [47]. Therefore, TDPM and TDPM+MTV measurements using the app were compatible in terms of measurement accuracy, although there were differences from those obtained using the electrogoniometer, and the findings may be more applicable to stroke patients with any degree of motor impairment compared with JPS.
In our study, we attempted to test proprioception in stroke patients under a limited set of measurement conditions that affect clinimetric properties, including the starting limb position and guidance method. At present, the appropriate measurement conditions for proprioception testing in stroke patients are unknown. Therefore, the relationship between the lesion site and motor impairment cannot be fully considered, and the obtained SEM and MDC should be interpreted with caution. In addition, the app showed higher readings than the electrogoniometer, which may differ from the original measured range of motion of the joint. In any case, since the results of this study have indicated the possibility that the app can replace the electrogoniometer, the next task is to verify the inter-rater reliability of the app by comparing each measurement condition in stroke patients. Furthermore, the number and location of lesions and the degree of motor impairment should be strictly defined and their characteristics should be extracted.
Conclusion
In conclusion, in patients with stroke, TDPM and TDPM+MTV measurements using the Goniometer Pro app can replace measurements using an electrogoniometer, but the obtained measurements should be interpreted with caution. Compared with TDPM, JPS has less concurrent validity for an electrogoniometer, and its use is limited by the degree of motor impairment in stroke patients. In the future, it is necessary to examine and validate the measurement conditions, lesion sites, and motor impairments in order to consider the necessity of using these proprioception tests together and to generalize the use of these tests in rehabilitation.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.
Funding
No funding was received for this article.