
Abstract
BACKGROUND:
Running-related injuries (RRI) are common among recreational runners, but research exploring lived experiences of a RRI is limited.
OBJECTIVE:
This study aimed to explore the psychosocial aspects experienced by recreational runners hindered in usual running because of RRI.
METHODS:
Individual semi-structured interviews based on a qualitative phenomenological methodology explored injured recreational runners experiences, reactions, thoughts, and feelings. Systematic text condensation was used as the analysis method.
RESULTS:
Three main codes were identified: Reasons for running: ‘Calm for me is a feeling of my body just relaxing. It may sound a bit weird because you run, but it is kind of a feeling of just being able to unplug‘, Daily life during an injury - besides running: ‘When I couldn’t run at all, it was super annoying. Several months it was completely empty. It was like there was a hole. There seemed to be missing something because I usually ran‘, Running while injured: ‘Do I feel pain? Or is it something else? And should I navigate regarding the length of the route and where I run, how fast I run, and with whom I run? ‘.
CONCLUSION:
The recreational runners experiences explored in this study support the importance of bio-psycho-social awareness when physiotherapists meet runners hindered in usual running because of RRI.
Keywords
Introduction
Running-related injuries (RRI) are common among recreational runners, and evidence indicates that a musculoskeletal injury often extends beyond a biological aspect [1–4]. Published research regarding the psychosocial consequences of a RRI is limited in a recreational running population. Using questionnaires to collect data, a study by Chan et al. [5] found increased psychological symptoms in injured runners', such as depression, anxiety, mood disturbance, and lower self-esteem, consistent with psychological symptoms found during experimental exercise withdrawal [6]. More recently, Verhagen et al. [7] explored recreational runners perception of RRI and the occurrence and prevention of RRI and identified that by providing information, advice, and programs to injured recreational runners, self-regulation of RRI could be recommended. Other studies within this field have not included injured runners, and the data collection is primarily based on questionnaires [8–10].
Chan et al. [5] suggest that loss of consistent running due to a RRI may result in psychological distress when running is used as a coping strategy to reduce stress or to induce psychological reinforcement. The loss of frequent running may reduce the quality of life and make daily living less manageable [11]. Therefore, an injury may increase the risk of sick leave, as stress is one of the most typical reasons for absenteeism from work [12]. A prolonged RRI may also reduce overall physical activity or result in the discontinuation of running, thereby increasing the risk of lifestyle diseases [13–17]. Considering the number of adults participating in running worldwide and the risk of RRI, increased knowledge of the psychosocial consequences in injured runners is pertinent [2, 18].
Available knowledge primarily stems from other athletic populations [4, 19]. However, from a management and rehabilitation point of view, population-specific insight and knowledge of experiences and reactions resulting from a RRI are important. Otherwise, physiotherapists may not explore psychosocial issues relevant to rehabilitation when treating an injured recreational runner [20, 21]. One way of strengthening the competencies of physiotherapists working with injured recreational runners would be to increase the accessible knowledge concerning the psychosocial consequences resulting from a RRI.
Therefore, this study aimed to explore the psychosocial aspects experienced by injured recreational runners hindered in usual running because of RRI. A phenomenological approach was used to explore injured recreational runners’ experiences, reactions, thoughts, and feelings [22].
Methods
Design
This study applied a phenomenological psychological methodology described by Amedeo Giorgi [23]. Giorgi's methodology emphasizes the importance of rich, descriptive data and the need to preserve the unique and subjective nature of individual experiences. It also emphasizes the importance of the researcher's own subjective experience and intuition in the research process. Audio-recorded semi-structured individual interviews were used as empirical material, and the systematic text condensation (STC) by Kirsti Malterud was chosen for analysis [24, 25].
Participants
Participants were recruited using convenience sampling with Facebook as the communication platform. Recruitment posts were written in the authors‘ Facebook network and running-related Facebook groups. Interested participants contacted the authors by responding to the recruitment post. The inclusion criteria were≥18 years, recreational runner with a weekly frequency of 3-4 runs/week, hindered in regular running because of a RRI, and living in the Northern Region of Denmark. Participant demographics are presented in Table 1.
Participant demographics
Participant demographics
This study followed the Helsinki Declaration for ethical principles in medical research. All participants received written and verbal information on the aim and scope of the study and informed written consent was signed. Due to the nature of the study, no permission from the system of research ethics committees according to the Danish Act on Research of Health Projects, Section 14, no. 2 was required [26].
Interview procedure
All interviews were conducted face-to-face and lasted, on average, 40 minutes. Three interviews were conducted in an office at the university, and two were conducted at the participant’s homes.
M. K. Festersen (male) conducted all five interviews with A. M. Kloosterman (female) acting as co-interviewer. Both interviewers were inexperienced in qualitative research but had conducted several interviews related to their clinical practice as physiotherapists. No relationship between the two interviewers and any participants existed before the interviews. All interviews were recorded using a dictaphone.
A semi-structured interview guide was developed using open-ended questions to explore recreational runners’ experiences of being hindered in usual running because of a RRI.
The interview guide contained three steps: (i) Briefing; introduction to the study. (ii) The interview consisting of three parts. Part 1 focused on the participant and the running-related injury and aimed at familiarizing the participant with the interview situation. Part 2 focused on exploring phenomena experienced when being hindered in running. Part 3 focused on the psychological and social aspects of being an injured recreational runner. (iii) Closing remarks; an invitation to share experiences the participant values on aspects not covered by the interview guide. The interview guide was pilot-tested by a research group member and an eligible participant. Only minor changes were made to the interview guide based on experiences from the pilot interviews.
Analysis
Interviews were divided between all authors and transcribed ad verbatim. Another research group member validated the transcript, and discussion solved disagreements. STC was used for analysis [24] with NVivo 12 (QRS international, 2021) as a coding program. The analysis consisted of four steps (Table 2) [27–29].
An example of the analysis process
An example of the analysis process
Step 1: Themes, getting a sense of the empirical material, and identifying themes. Step 2: Codes, identifying and sorting meaning units. The aim was to transform themes into more broad codes. In pairs of two, the authors divided the material into meaningful units. Subsequently, the authors combined themes into codes, as seen in Table 2. Step 3: Subgroup - Condensation, aimed to branch codes into subgroups and condensing meaning from the material. The authors individually made subgroup suggestions for each of the three codes. The authors discussed the proposals, and subsequently, condensates were formed. Quotes of the condensates are written as an expression of the individual subgroup.
Step 4: Description – Synthesizing, transforming condensates into descriptions and concepts to understand the phenomena. The authors designed content descriptions with citations from the meaning units.
Three main codes were identified: 1) Reasons for running, 2) Daily life during an injury - besides running, 3) Running while injured. Figure 1 shows examples of participant quotes related to each main code. Subgroups were highlighted within each code.
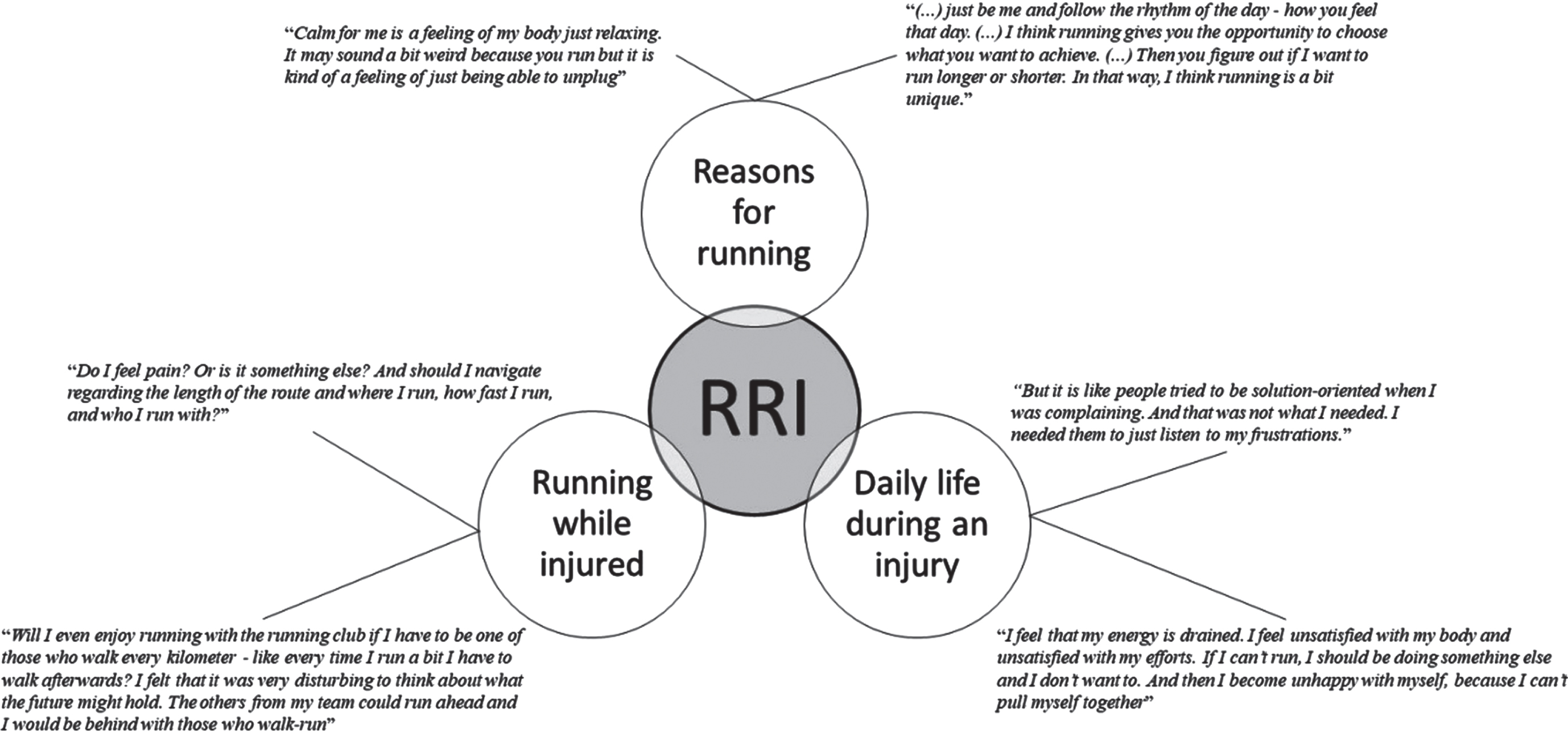
Participant quotes related to main codes. 1b. Alt text: An illustration of the three main codes; Reasons for running, Running while injured, Daily life during an injury, and their interacting with running-related injury. Each code is accompanied by quotes from the participants.
It became apparent during the analysis that the initial familiarizing questions explored several aspects of reasons for running.
Flexibility and community
The analysis shows that flexibility in running plays a significant role in the participant's choice of exercise. They express that running is easily accessible, requires no equipment other than a pair of running shoes, and can fit into a busy lifestyle where work, study, and family are a priority. The participants emphasize that they enjoy the many possibilities and the independence that running gives them. All express running as a good way to combine health with a busy life’s social and enjoyable aspects.
Running probably provides the participants with a solution to fulfill individual aspirations, such as a healthy lifestyle and a social life outside the family, with other important priorities such as work, spouses, and children.
‘(...) just be me and follow the rhythm of the day - how you feel that day. (...) I think running gives you the opportunity to choose what you want to achieve. (...) Then you figure out if I want to run longer or shorter. In that way, I think running is a bit unique.‘ - Participant 2.
The participants also express that the social communities they can combine with or obtain through running are very important. Two participants are involved in a running club but also run alone. The remaining participants run mainly alone but also enjoy running with their spouses or friends. Participants associate running with experiences that reinforce independence and flexibility.
Valuable
A feeling of mental calmness, therapy, or meditation while running, which provides energy and well-being, is mentioned by all participants. Furthermore, several participants mentioned the joy of running in nature, getting fresh air, and being alone with thoughts or not thinking at all.
‘Calm for me is a feeling of my body just relaxing. It may sound a bit weird because you run, but it is kind of a feeling of just being able to unplug‘ - Participant 1
Some participants describe being a runner increases their self-confidence, complacency, and self-acknowledgment. For some, this is explained by exercise, and appropriate body weight is related to a healthy lifestyle. Several participants mentioned that they started running as a means of losing weight but found new values along the way that they thought of from the beginning. Even though it can be hard to go for a run, all participants say that running is enriching on several levels, which cannot be achieved in any other way. The participants may highly value their identity as a runner and associate it with physical and psychological benefits. These benefits are, for some reason, considered unattainable without running, making running very valuable to the participants.
Daily life during an injury: Besides running
Social relations and relatives
When asked which changes the participants’ experience related to their social relations and relatives, the answer was none. However, after some elaboration, some experience an adverse change in temper, which they say could have been avoided if they had been able to go for a run to regain mental calmness. The participants experience a lack of understanding from their relatives and social relations, who mainly tend to be solution-oriented by suggesting alternatives to running rather than listening to the runner's frustrations. The runners are upset and turn to relatives or close social relations for compassion but are met with an un-compassionate solution-oriented focus from the runners' perspective. Which probably reinforces the negative change in temper and maybe unwarranted tension in their social life.
‘But it is like people tried to be solution-oriented when I was complaining. And that was not what I needed. I needed them to just listen to my frustrations‘ - Participant 5
Dealing with injury
When asked about changes to everyday life caused by their injury, the participants expressed that they didn’t experience any. However, their descriptions during the interviews do show that they experience some changes. During the day, they have become more aware of their body signals, thinking of how they use their body, using different footwear, or using sports tape as support. The participants also tend to seek alternative activities instead of running but are not obtaining the same satisfaction. Despite not considering injury as something which affects everyday life, the participants continuously deal with it by making small adjustments to their life.
‘I am working on going for walks and trying to like it. But it does not give me the same feeling of having exercised‘ - Participant 5
All participants consult a physiotherapist because of their running injury, which provides confidence for several participants. They all listen to their recommendations, do daily recovery exercises, adjust their running habits, or have a total break from running. All these initiatives related to running are possibly considered a normal part of dealing with injury. However, considering the other smaller adjustments also made to every day-life by the participants, a considerable amount of time and resources are spent dealing with the injury. Some participants tend to end up on their couch more often regardless of advice and effort to deal with injury and experience their everyday life as more inactive. This can also negatively influence their eating habits, which they relate to boredom or lack of energy.
Emotional response to RRI
Many participants mentioned that they do not think about being hindered in usual running during their everyday life. Still, they become more aware of the situation when they see runners outside or on social media. The most dominant feeling described during the interviews is turmoil due to being hindered in usual running. One informant mentions a feeling of loneliness because a large part of the social network is related to the running club, and another feels a “void in everyday life.
‘When I couldn’t run at all, it was super annoying. Several months it was completely empty. It was like there was a hole. There seemed to be missing something because I usually ran.‘ - Participant 3
The participants worry if they will be physically capable of running again and be able to enjoy running again. Waiting during recovery causes frustration, and they are uncertain of how to self-manage their injury to reduce recovery time. As a result of their injury, general thoughts like the uncertainty of being physically capable of carrying out their work and their possibilities of exercising in the future start to emerge. A feeling of failure and dissatisfaction with their efforts or being less attractive because of bodily changes are described during the interviews as a result of being hindered in their usual running.
‘I feel that my energy is drained. I feel unsatisfied with my body and unsatisfied with my efforts. If I can’t run, I should be doing something else, and I don’t want to. And then I become unhappy with myself because I can’t pull myself together‘ - Participant 5
Running while injured
New thoughts and habits
Being injured is described as a normal part of running for some, while this is entirely new for others. Most participants feel frustrated and irritated because of their limited autonomy regarding running. Several participants felt divided between wanting to run and respecting the physical limitations caused by their injury.
‘Do I feel pain? Or is it something else? And should I navigate regarding the length of the route and where I run, how fast I run, and who I run with?‘ - Participant 2
The participants experience increased respect and attention towards body signals. They are more careful during runs now than they used to be. The concerns that have arisen are challenging for the participants to navigate. For one, being injured is “normal”; for another, it is a new world to navigate. For one of the participants, the worries have filled them to such an extent that they have not yet started running again. For others, the increased respect for the body’s limitations has created greater attention and caution while running to avoid further or future injury. Injury has changed running for the participants, and the focus during running has shifted. Previously positive psychological benefits of mental calmness are challenged by a bodily focus and limitations in the valued flexibility of running.
‘Then I think that I have overrated my skills through time. In the future, I might be more careful and not be stupid because now I know that you can end up sitting on the bench for a long time if you do not think and hold yourself a bit back as they recommend.‘ - Participant 4
Community
The participants, who usually run in a community or with partners, experience a loss of social connectivity. Some become even more aware of the risk of never being able to regain their physical level before the injury and how this can affect their relations and self-image regarding running.
‘Will I even enjoy running with the running club if I have to be one of those who walk every kilometer - like every time I run a bit, I have to walk afterward? I felt that it was very disturbing to think about what the future might hold. The others from my team could run ahead, and I would be behind with those who walk-run. -Participant 4
Some participants describe a positive outcome, such as not being expected to participate in social running events. This new experience and knowledge about running injuries can contribute to new initiatives, for instance, exercises to prevent injuries in the running club.
Discussion
This study aimed to explore the psychosocial aspects experienced by injured recreational runners hindered in usual running because of RRI.
In 1979 JE Nash argued that running has two functions; promoting individual health and giving meaning to runners life [30]. The participants in the current study describe individual health as an important reason for running, a finding which resonates with the literature on reasons for running [7, 31]. Two perspectives on individual health are described, mental and physical. Running is for all the participants included in a healthy lifestyle as the preferred type of exercise. Running also provided participants with a meaningful social aspect, providing a way to stay in touch with friends while physically active. To all participants, running is also a way to gain mental calmness and relaxation in an otherwise sometimes chaotic and ever-changing daily life.
From the study findings, it became clear that all participants' greatly value participation in running and that RRI, on a psychosocial level, negatively impacts the participants everyday lives and their lives as recreational runners. The participants experienced a feeling of turmoil and a negative mood change, increased inactive everyday life, and a feeling of being less attractive because of bodily changes, which influenced their self-image by threatening the “running body” and a loss of social connectivity to the running community [32, 33]. These findings provide contemporary insight into injured recreational runners’ experiences, which may have important implications for clinical practice and physiotherapists managing injured runners. All participants consult a physiotherapist because of their injury. The physiotherapists provide recommendations regarding exercise therapy and modification of running habits, which provide confidence. However, the feeling of turmoil is present in all participants and is described as dominant. So, despite ongoing physiotherapeutic management of the participants RRI, potential psychosocial aspects of the injury are left unresolved. Therefore, it may be crucial to the injured runner that the physiotherapist not only acknowledges the psychosocial aspects of being injured but also explores how the injured runners manage these [34]. The biological part of physiotherapeutic management is still of great importance and relevance. Still, the following discussion will address the importance of a concurrent focus on the psychosocial aspect when working with alternatives to running, load modification, self-management strategies, and prognosis [35–37].
A drop in the level of physical activity has been reported among injured runners, and the participants in the current study also described an experienced increased level of inactivity [38]. This influences the physical aspect of individual health but may also be closely related to the psychosocial aspects [39]. Participants engage in alternative forms of exercise on their own initiative when unable to run. However, they do not experience the desired acute mental calmness and relaxation when participating in alternative exercise instead of running [40]. The combination of running and being out in the environment, by yourself or with others, seems important for the runners to experience the mental state they strive for. Reductions in running or discontinuation from running during a specified period of time is often part of the physiotherapeutic management of RRI. However, a relationship has been found between running and increases in good mood and decreases in bad mood [33]. Injured runners prevented from running experienced both negative mood changes and increased symptoms of psychological distress compared to injured runners who, despite injury, continued to run [5]. Therefore, physiotherapeutic management could possibly also be a source of a negative mood change when advising against running as part of a load management strategy. This is crucial for the healthcare provider to understand and consider in a patient-therapist relationship [41].
Further, the participants experience a change in their attention to bodily signals. Due to the RRI, they become increasingly aware of their body, perceiving bodily signals with increased caution. When running, the participants experience an internal conflict between the reasons for running and the perceived bodily signals. This may be another enabling part of the dominating feeling of turmoil. To positively influence the feeling of turmoil, physiotherapists could help injured runners understand their perceived bodily signals and provide strategies for self-regulation related to running and running-related injury symptoms [7].
Thoughts and attitudes among runners related to developing and preventing RRI are plentiful. Participants in the current study may have shared some of these thoughts and attitudes [8, 9]. Because when in need of treatment, they engaged in different strategies in an attempt to self-manage their RRI by changing running shoes or applying tape to support the injured tissue. But, most often, a feeling of insecurity accompanied these choices related to self-management strategies. In the clinical setting, this may be addressed by providing accounts for the clinical actions and relating these accounts to the runners’ concerns, as accounts have been shown to foster mutuality and may enhance the therapeutic relationship [42]. Therefore, engaging in an open-minded conversation about the embodied experience of injury, instead of a singular biological approach, providing the runner with the opportunity to express how they feel, and using timely produced accounts can be of great importance [42, 43]. The experiences of a lack of success with alternative exercise forms and the insecurity related to the different strategies for self-management may enable the dominating feeling of turmoil. As a physiotherapist, attention to these experiences is important. By providing acknowledgment and accounts during the exploration of these experiences, the physiotherapist may strengthen the therapeutic relationship and educate by including runners in the reasoning process and increasing self-confidence [42]. A because-account, defined as causes or needs related to existing matters, may be provided as a reason why the physiotherapist asks for insecurities related to strategies for self-management. An in-order-to-account, defined as aims, aspirations, purposes, and things that will be achieved or avoided as a result of the action, may address the importance of exploring multiple aspects in relation to the physiotherapeutic examination and treatment. During the exploration, adjustments to the runners, self-management strategies can be proposed, and potential concerns can be addressed within the interaction [42].
A prolonged injury period made some participants experience their injury period as both frustrating and unmanageable. Participants express fear of being unable to run as they did pre-injury, and some are afraid that it may affect their work capabilities in the future. Among injured participants from different sports and activities with a specific musculoskeletal injury, feelings of frustration and fear of the future are common findings [44, 45]. These findings highlight a need for strategies to manage the psychosocial aspects of a RRI among recreational runners and prevent the development of a misdirected problem-solving approach or fear avoidance of running [46, 47]. If not managed, the psychosocial aspect of a RRI may result in discontinuation of running despite biological recovery. Findings from the present study highlight the importance of physiotherapists making time to listen and engage with the injured runner beyond a biological perspective. An experienced lack of understanding from their surroundings, including physiotherapists, resulted in frustration among the participants, which Turner et al. [45] also describe among recreational runners with Achilles tendinopathy. Clement et al. [48] found that a health professional’s diagnosis made injured athletes situation more manageable and reduced their frustration. Likewise, a study by Wadey et al. [49] found the utilization of goal setting to be an effective coping strategy in athletes with high hardiness. Therefore, physiotherapists treatment may benefit from communicating the examination and treatment process to align expectations and by making time for conversation in consultations [50, 51].
The findings discussed were based on phenomenological reduction, non-value-based inquiry, and a search for descriptions instead of explanations. However, some methodological choices should be considered as they may have influenced the findings. The convenience sampling method may have increased participant diversity and reduced the risk of selection bias introduced by authors’ sampling based on specific characteristics [52]. Nevertheless, selection bias might have been unintentionally introduced by including more resourceful recreational runners, as participants had to contact the authors themselves.
Theoretical saturation was not sought because of the phenomenological nature of the study. Instead, data saturation was sought on an individual level – per interview – in accordance with Giorgi's focus on rich, descriptive data and the unique and subjective nature of individual experiences. In practice, this meant that interviews were completed when the interview team (M. K. Festersen and A. M. Kloosterman) felt they had fully understood the participant's perspective [53]. However, data saturation was not achieved on the level of the data set as a whole. Ideally, the recruitment would have continued until data saturation to explore the psychosocial aspects experienced by injured recreational runners hindered in usual running because of RRI [29, 54].
Both interviewers were inexperienced in qualitative research but had conducted several interviews related to their clinical practice as physiotherapists. However, being novices in the field may have limited the exploration of relevant aspects and their descriptions and left narratives unspoken. To increase the credibility and trustworthiness of the study, participant validation could have been used. The method used did, however, manage to create confidence and an informal, relaxed setting in the interview situation as participants, when evaluating their experience participating, expressed it as a safe and comfortable experience.
STC by Malterud was used as a strategy for analysis and was inspired by Giorgi’s Descriptive Psychological Phenomenology method. STC’s deviation from its inspiration might have conflicted with the descriptive phenomenological approach as junking meaning units during analysis may have disrupted the phenomenological reduction and a preconception-free approach to the empirical material. According to Giorgi, the analysis is not phenomenological if the phenomenological reduction is not maintained [23]. However, the STC strategy is described in more detail and has a more systematic approach to the empirical material, which the authors view as increased transparency. During the data preparation and analysis, dialogical validation through reflective dialogue and a between-authors independent transcription of interviews followed by cross-validation of transcriptions were used to ensure validity. However, the risk of disruption of the phenomenological reduction existed. The authors worked methodically with preunderstandings to increase awareness of potential preconceptions, as described by Tufford & Newman [55]. This was complemented by including authors, both present and not present, at the interviews in all parts of the study, including the transcription and analysis process [56].
This study does not show the development of phenomena over time. The injury duration differentiated between the participants, and this study made no attempt to separate or focus on rehabilitation phases. The responses to the phenomena present may be linked to different rehabilitation phases, as described by Clement et al. [48] he prominence of the phenomena present may vary between injury phases, time spent injured, and the influence of injury on physical ability [48]. In conclusion, the recreational runner's experiences explored in this study support the importance of bio-psycho-social awareness when physiotherapists meet runners hindered in usual running because of RRI. RRI negatively impacts everyday life on both a psychological and social level. The most influential phenomena were an experienced lack of mental calmness, increased body awareness, a feeling of lack of social connectivity, and a general frustration with the situation. Attempts to substitute activity do not negate these experiences, highlighting a need for strategies to manage the psychosocial aspects of a RRI among recreational runners to increase the quality of patient-centered rehabilitation.
Footnotes
Acknowledgments
We thank the participants of this study - this would not have been possible without them. We also thank the Department of Physiotherapy, University College of Northern Denmark, for making this possible. No funding was received for this work.
Conflict of interest
The authors have no conflict of interest to report.
Appendice 1 Consolidated criteria for reporting qualitative research checklist [ 57 ]
|
|
|
|
|
|
|
|||
| Personal characteristics | |||
| 1. | Interviewer | Which author/s conducted the interview | 4 |
| 2. | Credentials | What were the researcher’s credentials? E.g. PhD, MD | NA |
| 3. | Occupation | What was their occupation at the time of the study? | 4 |
| 4. | Gender | Was the researcher male or female? | 4 |
| 5. | Experience and training | What experience or training did the researcher have? | 4 |
| Relationship with participants | |||
| 6. | Relationship established | Was a relationship established prior to study commencement? | 4 |
| 7. | Participant knowledge of the interviewer | What did the participants know about the researcher? e.g. personal goals, reasons for doing the research | 4 |
| 8. | Interviewer characteristics | What characteristics were reported about the interviewer/facilitator? e.g. Bias, assumptions, reasons and interests in the research topic | 4 |
|
|
|||
| Theoretical framework | |||
| 9. | Methodological orientation and Theory | What methodological orientation was stated to underpin the study? e.g. grounded theory, discourse analysis, ethnography, phenomenology, content analysis | 3-4 |
| Participant selection | |||
| 10. | Sampling | How were participants selected? e.g. purposive, convenience, consecutive, snowball | 3 |
| 11. | Method of approach | How were participants approached? e.g. face-to-face, telephone, mail, email | 3 |
| 12. | Sample size | How many participants were in the study? | 4 – Table 1. |
| 13. | Non-participation | How many people refused to participate or dropped out? Reasons? | NA |
| Setting | |||
| 14. | Setting of data collection | Where was the data collected? e.g. home, clinic, workplace | 4 |
| 15. | Presence of non-participants | Was anyone else present besides the participants and researchers? | 4 |
| 16. | Description of sample | What are the important characteristics of the sample? e.g. demographic data, date | Table 1 |
| Data collection | |||
| 17. | Interview guide | Were questions, prompts, guides provided by the authors? Was it pilot tested? | 4 |
| 18. | Repeat interviews | Were repeat interviews carried out? If yes, how many? | NA |
| 19. | Audio/visual recording | Did the research use audio or visual recording to collect the data? | 4 |
| 20. | Field notes | Were field notes made during and/or after the interview or focus group? | NA |
| 21. | Duration | What was the duration of the interviews or focus group? | 4 |
| 22. | Data saturation | Was data saturation discussed? | 10 |
| 23. | Transcripts returned | Were transcripts returned to participants for comment and/or correction? | 10 |
|
|
|||
| Data analysis | |||
| 24. | Number of data coders | How many data coders coded the data? | 4-5 |
| 25. | Description of the coding tree | Did authors provide a description of the coding tree? | 5 |
| 26. | Derivation of themes | Were themes identified in advance or derived from the data? | 4-5 |
| 27. | Software | What software, if applicable, was used to manage the data? | 4 |
| 28. | Participant checking | Did participants provide feedback on the findings? | 10 |
| Reporting | |||
| 29. | Quotations presented | Were participant quotations presented to illustrate the themes / findings? Was each quotation identified? | 5-7 |
| 30. | Data and findings consistent | Was there consistency between the data presented and the findings? | 5-7 |
| 31. | Clarity of major themes | Were major themes clearly presented in the findings? | 5-7 |
| 32. | Clarity of minor themes | Is there a description of diverse cases or discussion of minor themes? | 5-7 + 9-10 |