
Abstract
INTRODUCTION:
Low back pain (LBP) is a leading cause of disability worldwide. A spectrum of psychological conditions such as anxiety, fear, stress and low mood are often reported to co-occur in individuals with persistent back pain and are cited as reasons for the continued experience of pain. However, any potential causal effect of emotional distress on new onset LBP is understudied. Therefore, the aim of this review is to examine the impact of emotional distress as a risk factor for new presentations of acute low back pain.
METHODS:
A systematic review was performed in accordance with the PRISMA guidelines. The Medline, Embase and APA databases were searched for primary research articles exploring emotional distress and low back pain. Prospective studies that investigated subjects initially free from back pain, who also undertook some form of psychometric testing at baseline, were included in the review. In total, 6 studies were identified with a broad geographical spread and diverse population cohorts including pregnant women, forestry workers, nursing students, adolescents, individuals with medical comorbidities and adult population studies.
RESULTS:
The results from all six studies found a significant relationship between an initial presence of emotional distress and subsequent onset of acute low back pain.
CONCLUSION:
This review encourages the acknowledgement of underlying emotional distress as a risk factor in acute low back pain, and to address it as part of the overall management plan.
Introduction
Descartes is generally credited with dividing the mind and body into separate entities in a concept known as dualism. What is the relationship between the mind and the body? This separation of the mental and physical states is seen across medicine in the biological reductionism of disease, where there is a separate specialty for various systems within the body, and indeed the mind. This contributes to a disempowerment of patients and discouragement of thinking that focuses on the whole patient [1]. In this sphere, conditions such as low back pain are viewed as local, biological problems and generally managed as such. Indeed, investigations such as MRI scans can substantiate this position by revealing mechanical findings such as disc bulges or degenerative changes which can be used to explain symptoms and direct management. However, it is important to consider that no specific nociceptive cause is identifiable in 85% –90% of low back pain (LBP) presentations, [2, 3] and therefore the causation of LBP needs to be explored further. There is a need to broaden the lens when looking at the aetiology of physical pain complaints such as LBP.
Embodied mind
Some authors argue that the mind is a dynamic process of the brain, [4] leading to the neologism “embodied mind” from which the brain is viewed from a more biological, tangible perspective, “regardless, if there is a mind or a soul or not” [5]. There is evidence of the co-existence of emotional distress in individuals suffering with pain [6]. Interestingly, it is possible that pain may result from emotional problems, with a bidirectional relationship between physical and mental health identified in a 10-year longitudinal study on 504,365 subjects initially free from mental illness or pain [7]. This study found that emotional dysregulation often preceded subsequent reporting of physical pain.
Study aims
The lifetime prevalence of LBP is between 70% and 85%, [8] and causal effects of psychological distress on the genesis of acute low back pain is understudied. This study explores emotional distress in a more systematic way by looking at pain outcomes longitudinally, delving into the portmanteau embodied mind. If mental wellbeing can have a direct impact on the expression of low back pain symptoms, then this will need to be addressed in the clinical management of each patient.
The search strategy used investigated prospective studies specifically, looking at subjects initially free from LBP, who were later followed up and assessed for the incidence of new onset acute back pain. Prospective studies are ideal for use in questions on aetiology and consequences [9] and this was of key importance for this review in identifying a wider range of risk factors for new back pain presentations. Of particular interest in this review was the recording of baseline psychometric tests on initially asymptomatic subjects to assess any future correlation between the presence of emotional distress and the subsequent development of acute low back pain.
This review aims to address a current gap in the literature in relation to the potential causal effect of emotional distress on the longitudinal presentation of low back pain.
Method
Protocol and registration
This study protocol is registered with the Open Science Framework (OSF); https://doi.org/10.17605/OSF.IO/XF2J6. It is also registered with PROSPERO (CRD42022303715).
Inclusion and exclusion criteria
The inclusion criteria were (1) Studies on LBP published in English where full manuscript was available, (2) Published in peer reviewed journals, (3) Prospective studies only, (4) Subjects must be asymptomatic for LBP at baseline, and (5) Studies must include psychometric tests where emotional or mental stress is recorded.
Exclusion criteria were (1) Pilot or protocol studies, (2) Studies that did not have LBP as the dependent variable, (3) Studies looking exclusively at work related stressors, and (4) Studies where participants had any history of chronic back pain.
Search strategy
A literature search was conducted of three major databases: Medline (1946 –Jan 2022), Embase (1974 –Jan 2022) and APA PsychInfo (1806 –Jan 2022). The search was conducted initially in January 2022 and subsequently updated on the 06/07/2023. The key search terms included are outlined in Box 1.
Box 1: Terms used in database search
*Emotional distress or *Stress, psychological
*Low back pain or *back pain or *Lumbago or *lumbosacral pain
*Prospective studies or *longitudinal or *Prospective Cohort study
Additionally, reference lists of the selected articles were searched manually for other articles which may have met the inclusion criteria.
Selection procedure
The selection procedure was carried out in line with PRISMA guidelines, which is outlined in Fig. 1. The initial search was carried out using a combination of the key words identified in the search strategy, box 1. All papers were screened initially by assessing the titles and abstracts, removing those studies that did not meet the inclusion criteria. Full text reviews of the remaining studies were carried out, and only those that satisfied the inclusion and exclusion criteria were retained for analysis.
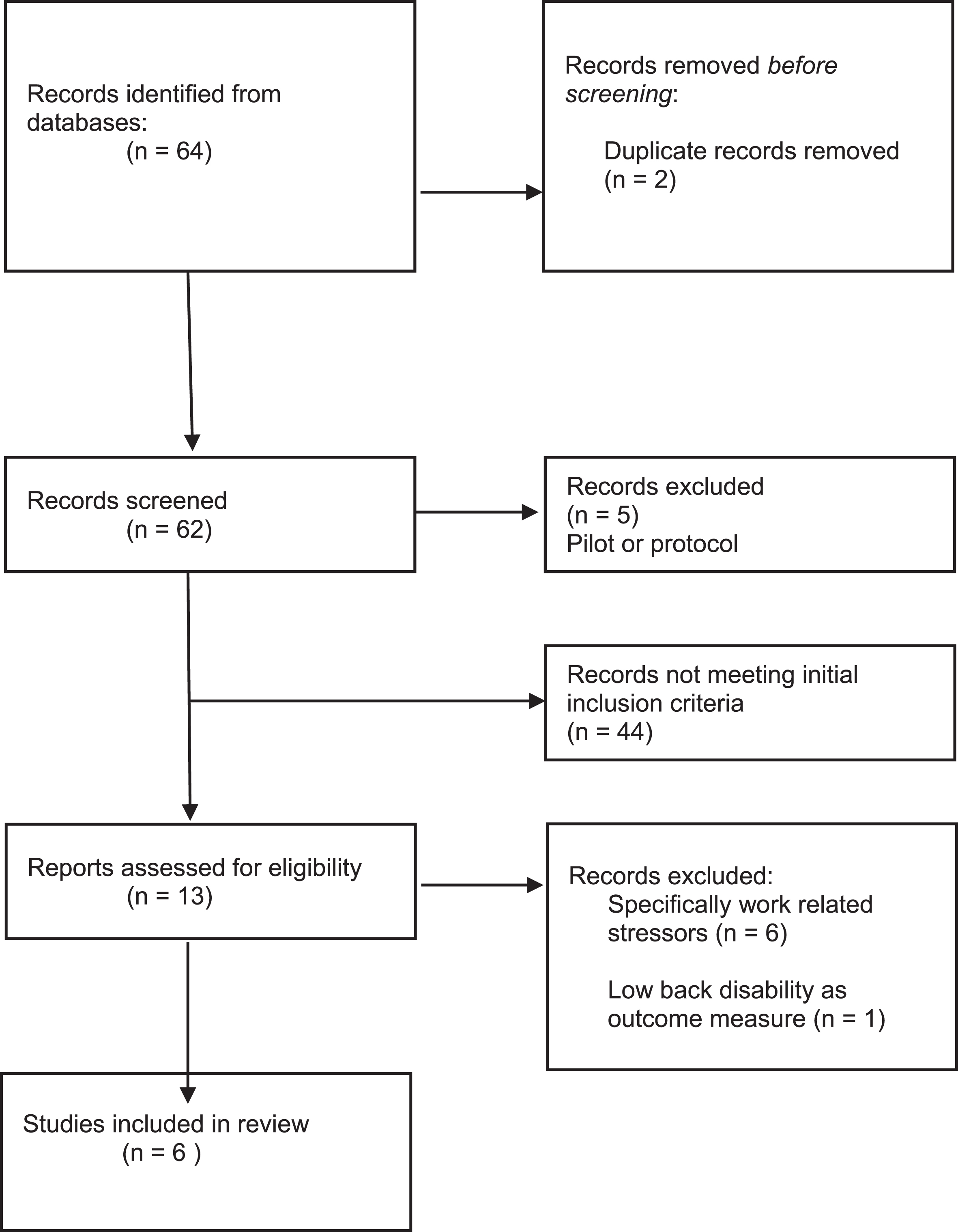
PRISMA flow diagram demonstrating flow of studies through the review.
Data was extracted according to PRISMA guidelines, and placed into a prepared word document table, which was used as a reference throughout the review. This was used in the selection process to confirm that the inclusion criteria were satisfied, and in documenting the characteristics of the studies such as age, gender and location.
CASP outcomes
The selected studies were appraised using the CASP (Critical Appraisal Skills Programme) checklist for Cohort studies. This checklist was used to assess the validity and relevance of the studies and whether we can confidently apply the results to a wider population.
Results
Study selection
The initial database search yielded a total of 64 studies. Following removal of duplicates, pilot, and protocol studies (n = 7), a further 44 studies were excluded based on review of abstract and methodology. The most common reason for studies being discarded at this stage was the inclusion of participants with existing back pain related symptoms at baseline (usually the result of a chronic condition, n = 41). Further studies were excluded due to the use of non-validated psychometric tests (n = 3).
The remaining 13 articles were screened in full. One study measured low back disability as its dependent variable and when assessed by the second author was determined to be too divergent from the proposed subjective reporting of LBP outlined in this review’s inclusion criteria [10]. Six other studies were excluded due to specific, situated occupational outcome measurement or focus, where this review aimed to observe the effects of everyday emotional distress. This left 6 studies to be included in the review with the process outlined in the PRISMA diagram, Fig. 1.
Study characteristics
Location
A summary of the selected studies is presented in Table 1, with a wide geographical distribution shown {UK (n = 2), Netherlands, Australia, Finland and USA}.
Characteristics of selected studies
Characteristics of selected studies
Five studies included male and female participants, with one study having males as 74% of the selection owing to the setting within the forestry industry [11]. Another study included female only participants in a study on lumbopelvic pain in pregnant women [12]. Of note, one study carried out its research on 11–14-year-old schoolchildren representing a wide-ranging sample for the present systematic review [13].
Sample size
These were generally large cohort studies with 3 studies recruiting more than 1000 participants, two studies consisting of 217 and 694, while the final interventional study on discography had 96 recruits.
Theoretical underpinning of studies
All the selected studies looked at potential risk factors for the development of LBP. Physical factors such as mechanical loading and posture have been widely researched with mixed results. More recently, authors have investigated emotional stressors of musculoskeletal pain, particularly in relation to work environments where absenteeism can have such a negative impact. Interestingly, the inclusion parameters for the current review resulted in studies that had psychometric tests assessed almost as an adjunct which helped create a diverse demographic across the six papers. This diversity is highlighted through the different demographics investigated including lumbopelvic pain in pregnant women, [12] work factors as a contribution to back pain across the forestry industry, [11] the impact of nursing professions on LBP [14] and any potential clinical value of discography in predicting back pain onset [15]. Two papers were multi-factorial population studies looking at a battery of physical and mental characteristics [13,16, 13,16].
Duration of data collection
The selected studies were prospective in nature ranging from 24 weeks (pregnancy cohort) up to 10 years (population cohort studies)
CASP outcomes
Included studies were assessed using the CASP outcome tool and cross checked by the second author. The studies selected were of a high quality as outlined in Table 2. All studies had clearly focused research objectives, and specific population studies were chosen for each study with clear description of recruitment. One study used subjects who were identified from previous engagements with local medical centers which could be seen as contradictory to the strict exclusion criteria outlined in the current review. However, the authors do not state whether the subjects specifically reported with LBP, only mentioning previous neck surgery and psychosomatic pains in the history [15]. It could be argued that due to the history of pain, although not specifically LBP, could be a confounding variable in these subjects subsequently reporting pain. Nevertheless, the findings still show a strong relationship between emotional distress and future onset LBP.
Summary of CASP outcome tool
Summary of CASP outcome tool
A point of interest arising from the CASP tool was the selection of outcome and exposure measurements. For example, three studies used LBP of more than one day as their independent outcome variable, one study used back pain of more than 7 days and two studies used scales which assessed pain reporting, medication usage and medical visits. Psychometric testing for mental distress was also assessed differently in each study, reflecting the broad spectrum of mental distress. This is acknowledged as a potential confounding variable, but only scientifically validated psychometric tests were included in this review, as outlined in Table 1.
Finally, in relation to the applicability of the findings presented in this review, it could be argued that some of the studies had narrowly focused cohorts making it difficult to generalise to the wider population. For example, one study focused on a specific cohort of pregnant women in their investigation into lumbopelvic pain lasting 24 weeks [12]. Another population study looked specifically at children aged 11 to 14 years [13]. However, it could be argued that the consistency of findings across the diverse populations only serves to strengthen the overall results of this review, highlighting that emotional distress can have an impact on acute LBP in any demographic.
A brief overview of the findings from this systematic review are outlined in Table 3.
Summary of Findings, including significant and non-significant predictors of LBP
Summary of Findings, including significant and non-significant predictors of LBP
Undoubtedly, there were two factors that consistently preceded new onset LBP: emotional distress and history of back pain. Smoking had a significant association, while mechanical factors, physical activity/BMI and demographics had inconsistent or weak association.
A major strength of this review is the consistency of findings across all the studies in relation to the presence of initial mental distress and subsequent longitudinal findings of low back pain. This causal effect of emotional wellbeing on physical health occurred across a diverse range of participants including pregnant women, [12] forestry workers, [11] nursing students, [14] adolescents, [13] men and women followed in long term population studies [16] and subjects recruited from previous medical studies with musculoskeletal dysfunction [15]. The studies included examined a wide range of variables for LBP including physical loads and body morphology, as well as multiple psychometric evaluations.
Interestingly, emotional distress as a risk factor for new onset LBP was never the sole focus of the studies included, but part of a number of factors investigated, giving confidence to this review around any unintended bias. For example, one study looked specifically at discography injections in which the authors hypothesized that a painful response to discography might contain pre-clinical clues to future back pain [15]. Although this hypothesis proved unfounded, the authors discovered a significant correlation between emotional distress at baseline and subsequent acute onset LBP. This finding of mental stress as a risk factor for future onset LBP was found in each of the six studies, despite the varying populations and methodologies and adds considerable strength to the relationship postulated in this review around the link between emotional distress and musculoskeletal pain.
A limitation of this review identified in the CASP appraisal was the way emotional distress is captured. Psychometric tests differed across the studies with variations in the specific domain targeted i.e., low mood, stress, anxiety and coping skills. It is certainly possible that reports of anxiety, depression or general stress could have different impacts on physical wellbeing. There may also be issues with self-reported questionnaires in relation to well-being including problems relating to definition, introspection, memory, and insight [17]. However, when taken as a whole, the convergence of the relationship between some form of emotional distress or mood affect, and the reporting of LBP across all the studies gives confidence that the overall findings have applicability to the wider population.
Mental health and physical pain: Evidence to date
Emotional distress has been reported in the acute stages of LBP [18] and some authors recommend screening for depression in the early stages to prevent progression of acute LBP into a more chronic pain state. These findings suggest that targeting emotional issues early in back pain presentations could mitigate against future costly and potentially inappropriate healthcare use for individuals with chronic LBP [19]. This review aimed to investigate the causal effect of mental wellbeing and LBP from an earlier timeline and to assess the possibility that emotional distress could precede the onset of acute LBP. Viewed solely from a mechanical standpoint, it is easy to see why LBP would be investigated radiologically and managed by medication. However, very few interventions for acute pain show any clinically significant differences from no treatment [20]. This uncomfortable truth challenges us to rethink the factors contributing to the presentation of LBP. Indeed the high placebo effects seen across various medical trials demonstrate the need to improve our understanding of the psychosocial context of how pain is experienced and expressed [21].
Emotional disorders such as anxiety and low mood are often reported in patients with chronic pain explained by the negative impact of pain on mental wellbeing. However, the findings of this review suggest that mental distress may precede the physical symptoms of pain and may itself be an independent genesis of the physical pain presentation, as in the case of LBP. This requires a reframing of how pain is viewed to address the “deep fault line that separates ideas about the workings of the body from those about the workings of the mind” [22]. The argument proposed by this review is that depression may not be strictly a disorder of the mind or that specifically, LBP may not be strictly a disorder of the back. It is prudent to avoid a single story around pain and consider the embodied mind to help us improve our understanding of the individual pain experience. This review has shown comprehensively that emotional health is a significant risk factor in the output of LBP.
How can we explain the relationship between emotional distress and pain?
In relation to the lumbar spine, disc herniation is considered a major contributor to pain despite the reported presence of disc pathology in 30–40% of asymptomatic subjects [23]. Inflammation may account for pain in symptomatic cases of LBP as seen in the phagocytic activity of macrophages in the nucleus pulposus of surgically removed herniated discs on subjects who were positive for pain and had failed to respond to conservative treatment [24]. This inflammation could be explained as the result of the interaction between the physical elements, namely the herniated disc and the surrounding tissue. However, it is also possible that any inflammation observed may be secondary to an underlying auto-immune response [25]. This concept that the immune system could trigger an inflammatory reaction opens the possibility that any agitation of the immune system, physically or mentally, could result in an inflammatory expression of physical pain elsewhere in the body, such as in the lumbar spine.
Inflammation could be a key player in the onset and perpetuation of depression, [26] and mental stress could trigger an inflammatory response leading to depression [22]. A large birth cohort study in New Zealand showed that children who had experienced abuse or adversity by age 8 had increased levels of inflammatory proteins in their blood at age 21 [27]. Some studies have demonstrated that even modest amounts of sleep loss can cause the presence of inflammatory cytokines [28]. Therefore, it is possible that disturbances of emotional and mental processes can increase the levels of inflammatory markers in our bodies. This inflammation may provide the ideal environment for pain to prosper through the sensitisation of our nervous system, with pro-inflammatory cytokines known to be contributors to inflammatory and neuropathic pain [29]. Therefore, it is reasonable to consider that the origin of these cytokines, whether from physical or mental stress have the capacity to result in the expression of physical pain for the individual involved.
Sleep and physical health
There is further evidence in relation to sleep and how it affects our mental and physical health. Sleep complaints may be among the more robust prodromal symptoms reflecting partial depressive or anxiety symptoms [30]. One prospective study suggests that sleep problems precede LBP [31] and poor sleep has been described as a potent predictor of LBP in healthcare workers which agree with the findings of this review that emotional states can influence the onset of LBP [32].
Future research
There are a number of avenues for future research which arise out of this systematic review. First, nonpharmacological treatments such as CBT for LBP warrant further investigation. Physiotherapists can play a key role in integrating some CBT concepts in the management of LBP using graded activity and operant conditioning [33]. Inclusion of strategies to improve emotional distress in the management of pain has been hypothesised as essential in the development of future interventions for pain [20, 34], and our review supports the need for inclusion of emotional distress as an intervention target going forward. This is supported by a systematic review looking at CBT for LBP with five of the six studies included showing significant improvements in back pain [35].
Secondly, cortical changes in the primary somatosensory cortex have been identified in individuals with chronic LBP. Investigating changes in the brain may prove useful in understanding why some people move from the acute to chronic states of LBP, or even from low mood to major depressive episodes.
Conclusion
Mood disorders are recognised by the WHO (World Health Organisation) as the leading cause of disability worldwide. There is growing scientific evidence that these disorders may precipitate a kaleidoscope of physical symptoms, such as LBP in some cases. This review suggests that heightened or prolonged exposure to emotional distress could contribute to an entropic-like deterioration into dysfunctional states including LBP.
The evidence found in this review unequivocally supports the theory that emotional distress is a significant risk factor in the onset of acute LBP. Mental health awareness and education needs to be brought into greater focus to help prevent the onset of intractable chronic conditions such as musculoskeletal pain. Healthcare professions such as Physiotherapy and Psychology are ideally placed to target this gap in the understanding of back pain, working as part of multidisciplinary teams. The Cochrane database is turning towards increased mining of individual patient data from existing trials highlighting the need for a more individual approach when managing pain [20]. The recommendation from this study and shared by the current review, is to broaden the story around the aetiology of LBP to include emotional and mental wellbeing, facilitating the implementation of timely and appropriate individual treatment strategies.
Footnotes
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
None.