
Abstract
BACKGROUND:
The evaluation and treatment of patients with low back pain (LBP) often involve categorization based on movement direction. However, it is not certain whether the lumbar spine and hip motion angles are associated with movement direction in individuals with LBP.
OBJECTIVE:
The purpose of this study was to verify whether the motion angles of the lumbar spine and hip joint are associated with the movement direction in individuals with LBP.
METHODS:
Participants were recruited as volunteers at the authors’ institutions. In this cross-sectional observational study, participants were divided into two groups: those without LBP and those with LBP. To measure lumbar spine and hip motion angles in clinical movement tests (trunk forward bending and prone hip extension), those with LBP were divided into a flexion LBP group and an extension LBP group. Wearable sensors were used to measure lumbar spine and hip motion angles.
RESULTS:
Participants with LBP had a greater hip motion angle in the early stages of movement than that of those without LBP; this was associated with the movement direction in which pain appeared.
CONCLUSIONS:
In individuals with LBP, the motion angles of the lumbar spine and hip joint are associated with the movement direction. Therefore, this pain subgroup and associated movement direction should be considered when evaluating and treating individuals with LBP.
Introduction
Low back pain (LBP) has a lifetime prevalence of > 80%, making it a global problem that seriously affects the quality of life, daily living activities, and socioeconomic status of patients [1, 2]. Biomechanical factors as well as psychosocial factors have been cited as causes of LBP [3], and repetitive or sustained overloading of the lumbar spine can cause LBP [4].
Numerous studies have examined the kinematic characteristics of the lumbar spine in individuals with LBP to help in the improvement of biomechanical factors associated with it, but no consensus has been established. There is a trade-off between the motion of the lumbar spine and the hip joint [5], and many clinical movement tests are used to predict the mechanical load on the lumbar spine by evaluating the motion characteristics (i.e., motion angle and timing) of not only the lumbar spine but also the hip joint [6, 7]. The lumbar spine moves excessively in individual with LBP, as shown in the kinesiopathologic model [3, 7]. Conversely, other reports have indicated that individuals with LBP limit their lumbar movements to avoid pain [8, 9]. The difference between these contradictory results may be attributed to the evaluation of LBP as a single condition.
Therefore, evaluation in subgroups based on LBP characteristics is recommended [10–12]. Some LBP classification systems are based on the direction of movements associated with symptoms [13, 14]. Individuals with LBP who play trunk rotation-related sports have different kinematic characteristics from those without LBP in rotation-related clinical movement tests, indicating the importance of considering the direction of movement [7]. However, differences in lumbar spine and hip kinematics between subgroups based on the movement direction in which LBP appears have not been adequately examined. Furthermore, individuals with LBP may use a strategy of overall stiffening through simultaneous contraction to avoid pain, or the overall loosening of the lumbar region may result in hyper-/hypomobility of the lumbar region [15]. However, it is unclear whether this is also associated with direction of movement or whether there is a consistent response regardless of the movement direction.
Therefore, this study aimed to verify whether the motion angles of the lumbar spine and hip joint are associated with the movement direction in individuals with LBP. We examined whether there is a difference in the motion angles of the lumbar spine between a group of individuals without LBP and a group of individuals experiencing LBP due to different movement directions. We also explored the relationship between the movements of the lumbar spine between different movement directions.
Methods
A total of 62 individuals without LBP (29 men and 33 women, age 20.2±1.2 years, height 165.0±8.8 cm, weight 56.3±9.5 kg) and 31 individuals with LBP (11 men and 20 women, age 20.1±1.1 years, height 164.6±8.0 cm, weight 57.6±10.6 kg) were included in the study. The inclusion criteria were as follows: (1) individuals without typical physical functional disabilities, such as paralysis or arthropathy of the lower limbs, (2) those who did not experience any pain that could interfere with activities of daily living other than in the lumbar region, and (3) those who had not undergone surgery that affected the movement of the lumbar spine or hip joint, such as lumbar fusion surgery or artificial hip joint. Those with neurologic symptoms in the lower extremities and those with LBP in both lumbar flexion and extension were excluded. All measurements were conducted at Kyoto Tachibana University Yushinkan between October 2020 to November 2020.
This study was conducted according to the Declaration of Helsinki. The purpose and methods of the study were explained orally and in writing, and written informed consent was obtained from the participants before their participation in the study. This study was conducted with the approval of the Ethics Committee of Kyoto Tachibana University (approval no. 20-09).
Participants with LBP were asked to rate the intensity of LBP using the Numeric Rating Scale. As in a previous study [16], LBP was defined as pain localized below the costal margin and above the inferior gluteal folds at the time of measurement and which had persisted for more than 3 months.
For subgrouping in the direction of movement associated with pain, participants with LBP were classified into two groups: individuals who experienced pain during movements associated with lumbar flexion (flexion LBP group) and those who experienced pain during movements associated with lumbar extension (extension LBP group). Only the flexion LBP group and extension LBP group were included in this study because no one had pain with lumbar lateral flexion or rotation alone.
To evaluate kinematic characteristics, the motion angles of the lumbar spine and hip joints were measured using clinical movement tests. Accordingly, a wearable sensor (TSND151, ATR-Promotions, Sagara, Japan) and a receiving software (Sensor Controller, ATR-Promotions) were used [17]. Three wearable sensors, placed on participants’ thoracolumbar transition, lumbosacral transition, and right thigh, were used. The upper edge of the sensor on the thoracolumbar transition was placed at the upper edge of the first lumbar vertebra, and the upper edge of the sensor on the lumbosacral transition was placed at the upper edge of the sacrum (see Fig. 1a and 1b). The thigh sensor was placed on the posterior thigh at the midpoint of the sciatic tuberosity and the popliteal fossa (see Fig. 1c). Sensors on the thoracolumbar and lumbosacral transitions were positioned at the midline on the frontal plane of the body, and sensors on the thigh were placed at the midline on the frontal plane of the right thigh. The sensor was sufficiently fixed with tape or an elastic band to prevent position changes during measurement. In addition, the locations of the sensors were marked and checked after each measurement. The sensor settings for the measurement were as follows: acceleration range,±8 G; angular velocity range,±1.000 dps; and sampling frequency, 100 Hz. The motion angle of the lumbar spine was defined as the angular difference between the sensor on the thoracolumbar transition and the sensor on the lumbosacral transition, and the motion angle of the hip joint was defined as the angular difference between the sensor on the lumbosacral transition and the sensor on the thigh. Motion angles in the sagittal plane of the lumbar spine and hip joint were extracted from the sensor data.
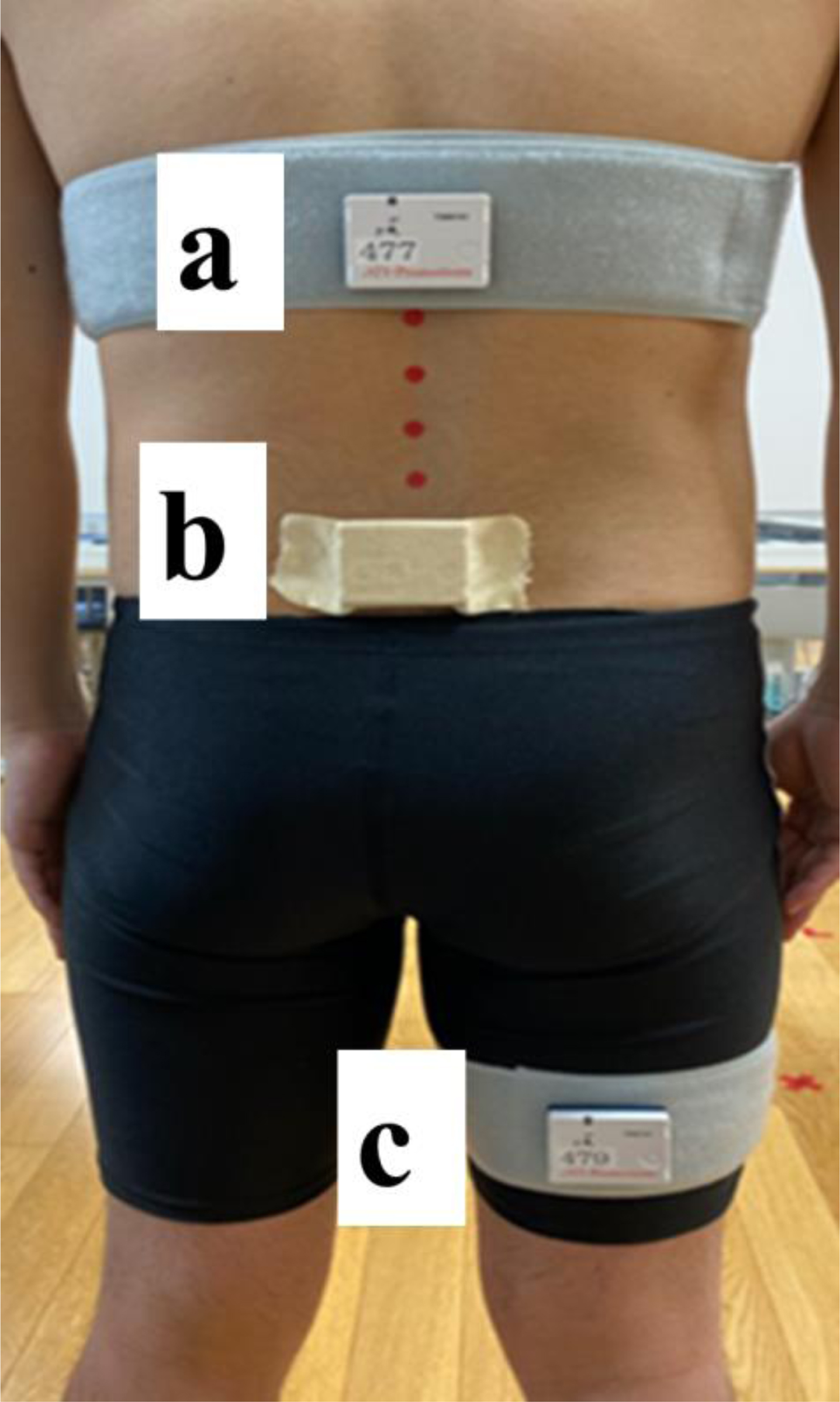
Placement of wearable sensors: (a) thoracolumbar transition, (b) lumbosacral transition, and (c) right thigh.
Two clinical movement tests were performed: the trunk forward bending (TFB) test, which is frequently used to assess motion in the flexion direction, and the prone hip extension (PHE) test, which is frequently used to assess motion in the extension direction (see Fig. 2). In the TFB test, participants held the resting position (standing position with the lower limbs shoulder-width apart) for 5 s and subsequently performed the task to the final position in active movements over 3 s to a 60 beat/min (bpm) metronome. In the TFB test, participants performed TFB movement upon hearing the instruction “please bend forward” from the free-hanging upper-limb position. The PHE test was performed with participants in the prone position on a bed, and they were instructed to “lift the lower limb” for 3 s to a metronome of 60 bpm, and the movement was performed in active movement to the maximum hip extension position. Each measurement was performed in triplicate, and the mean value was used. For the TFB test, the tilt angle of the sensor on the thoracolumbar transition was used as the index angle of the task (e.g., 50° of trunk forward bending); by contrast, the tilt angle of the thigh sensor was used as the index angle of the task for PHE. The TFB test may be used to analyze up to 50° of trunk forward flexion; however, many participants could not perform movements beyond 50°. Therefore, for TFB, data for each 20° from 10° to 50° and data at the maximum position were used. For the same reason, for PHE, we used the data of the 10° task index angle and data of the maximum position and extracted the lumbar spine and hip motion angles. Furthermore, the angular difference between hip and lumbar motion (ADLH; hip motion angle – lumbar motion angle) was calculated from the obtained lumbar spine and hip motion angles to provide an index of the contribution of lumbar motion to the hip motion.
SPSS, version 28 (IBM SPSS Statistics, Japan IBM, Tokyo, Japan) was used to perform the statistical analysis. One-way analysis of variance and chi-square tests were performed to compare the general characteristics between groups. One-way analysis of variance and multiple comparisons (Tukey) were used to compare motion angles between groups. The relationship between ADLH in TFB and PHE was examined using Pearson’s correlation coefficient. Values of p < 0.05 were considered significant, and data are presented as mean±standard deviation.
The general characteristics of each group are shown in Table 1. Thirty-one participants had LBP, of which 15 belonged to the flexion LBP group and 16 to the extension LBP group. No significant differences were found among the groups in terms of sex, age, height, and weight. The NRS of LBP was not significantly different between the flexion LBP and extension LBP groups (see Table 1).
Tables 2 and 3 show group comparisons of lumbar and hip motion angles for each clinical movement test. In TFB, the hip flexion angle was significantly higher in the 10° TFB-only flexion LBP group than in the non-LBP group (see Table 2). In PHE, the lumbar spine angle was significantly lower in the extension LBP group than in the non-LBP group at the 10° position, and the hip angle was significantly higher (see Table 3). The maximum position was significantly lower in the lumbar-only extension LBP group than in the non-LBP group (see Table 3). Table 4 shows the correlation coefficients for ADLH in TFB and PHE. The ADLH in TFB and PHE was not significantly correlated at any angle.
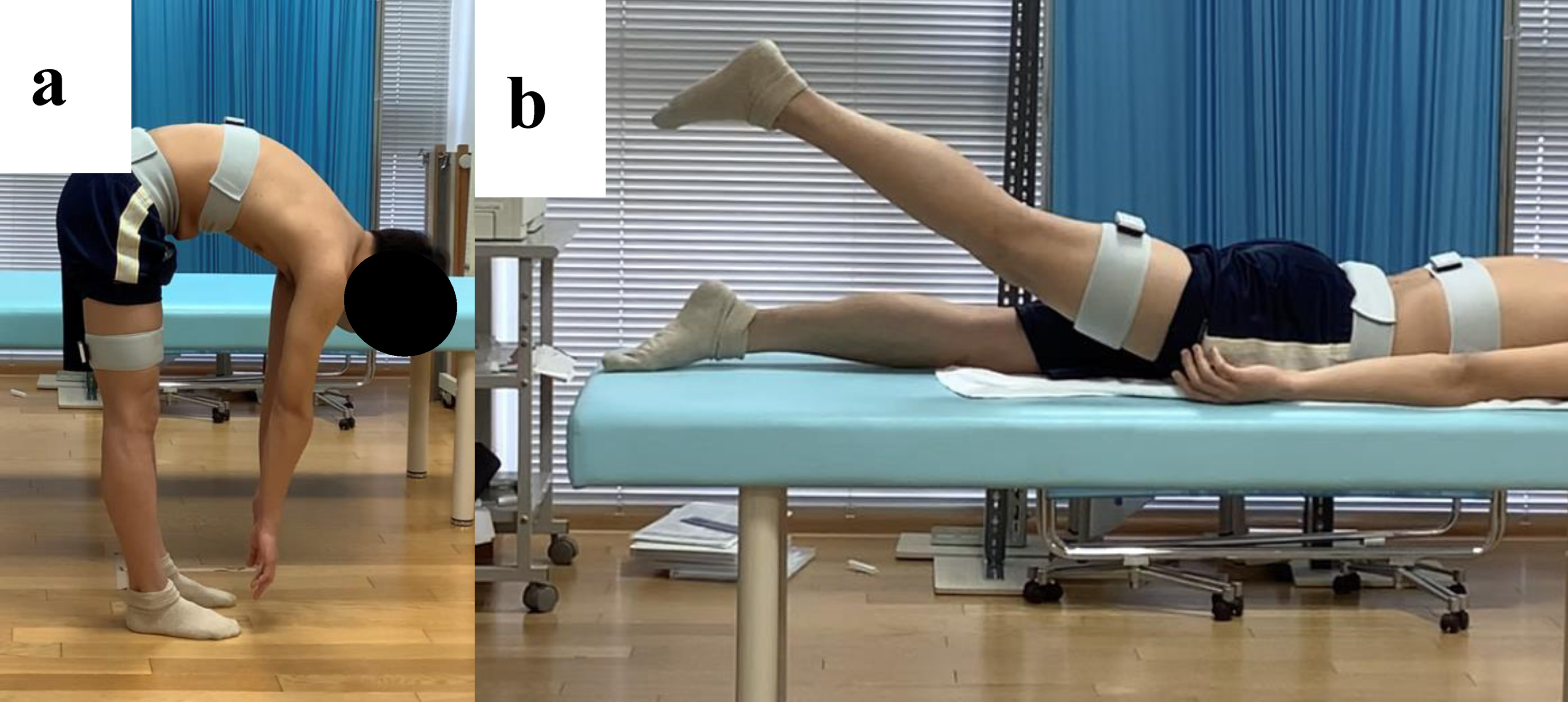
Clinical movement tests: (a) trunk forward bending and (b) prone hip extension.
General characteristics of the participants
LBP, low back pain; NRS, Numeric Rating Scale. Data are presented as mean±standard deviation unless indicated otherwise.
This study investigated whether there were differences in lumbar spine motion angles between the non-LBP group and the group with different movement directions in which LBP appeared, as well as the relationship of lumbar spine motion angle between different movement directions.
Karayannis et al. [18] examined the relationships among subgroups of a well-known classification system and showed that the subclassification of individuals may enable better targeted treatment. Therefore, the results of the present study may contribute to the selection of evaluations and training that considers the patient’s characteristics in the treatment of LBP.
The results of this study indicate that participants with LBP are more likely to have greater hip motion and less lumbar motion in the early stages of movement than those without LBP. Several previous studies [19–21] have reported that individuals with LBP have decreased motion in the lumbar spine and increased motion in other regions, such as the hip and thoracic spine. Particularly, Porter et al. [21] reported that the contribution of the lumbar spine decreases compared with that of the hip in the early phase of the TFB movement in individuals with LBP, and the present study showed similar results. Furthermore, in the present study, not only in TFB but also in PHE, lumbar spine motion was smaller and hip motion was greater in the early phase of movement in participants with LBP than in those without LBP.
Lumbar spine and hip joint flexion angles for each group in the TFB test
LBP, low back pain; TFB, trunk backward bending; ADLH, angular difference between hip and lumbar motion; max, maximum. Data are presented as mean±standard deviation unless indicated otherwise. *Significant difference compared with the non-LBP group.
Lumbar spine and hip joint extension angles for each group in the PHE test
LBP, low back pain; PHE, prone hip extension; ADLH, angular difference between hip and lumbar motion; max, maximum. Data are presented as mean±standard deviation unless indicated otherwise. *Significant difference compared with the non-LBP group.
ADLH correlation coefficients for the TFB and PHE tests
ADLH, angular difference between hip and lumbar motion; TFB, trunk backward bending; PHE, prone hip extension; max, maximum.
Fear of pain associated with movement [22] and protective mechanisms against tissue damage [23] increase muscle activity and limit movement. Additionally, individuals with LBP have delayed postural adjustment mechanisms during movement [24, 25]. Therefore, defensive muscle activity in the lumbar spine could continue after starting the movement and delayed adaptation of the muscle activity, resulting in a decrease in the motion of the lumbar spine in the early phase of the movement and a compensatory increase in the motion of the hip joint. Therefore, intervention in the early phase of movement may be key to LBP treatment.
Furthermore, the present results showed that the tendency of participants with LBP to have less lumbar motion and more hip motion was also related to the movement direction, with flexion (TFB) influencing the flexion LBP group and extension (PHE) influencing the extension LBP group. In support of the above, ADLH was not correlated with TFB and PHE at any angle in the participants with LBP. Nelson-Wong et al. [26] examined the prediction of LBP using the active straight leg-raise test, which is a sagittal motion, and the hip abduction test, which is a frontal motion. They reported that problems in one plane do not always affect other planes, and the combination of the two tests is more useful than the use of either of the tests. Therefore, participants with LBP are suggested to make adaptations related to the movement direction in which the pain appears. Moreover, evaluation and treatment of persons with LBP should consider the direction of movement.
A limitation of this study is that the participants were limited to young adults. Future validation should be conducted with other age groups, such as middle-aged and older adults. Although the lumbar spine was analyzed as a single segment in this study, Kuai et al. [27] stated that lumbar segmental evaluation is important. Future research should also investigate interspinal segmental movement, as more detailed trends can be captured by assessing interspinal segmental movement.
In conclusion, in this study, in addition to the presence or absence of LBP, participants were classified according to the movement direction associated with pain, and the lumbar spine and hip motion angles of each group were compared. The results showed that the lumbar spine motion in the early phase of movement was lesser in the LBP group than in the non-LBP group. The tendency was related to the direction of motion in which the pain appeared and was direction-specific. Therefore, this pain subgroup and associated movement direction should be considered when evaluating and treating individuals with LBP.
Funding
This research was funded by JSPS KAKENHI Grant Number JP19K24181.
Conflict of interest
The authors declare no conflicts of interest.