
Abstract
BACKGOURND:
The pathophysiology of adhesive capsulitis may be associated with increased neural mechanosensitivity in upper limb neurodynamic test.
OBJECTIVE:
To investigate the findings of neurodynamic assessment in patients with more than four month history of adhesive capsulitis.
METHODS:
Thirty-five patients with more than four month history of adhesive capsulitis were participated in this study. A physiotherapist performed the Upper Limb Neurodynamic test 1 procedure on the participant’s upper limb. Elbow extension range of motion at the end of the Upper Limb Neurodynamic test 1 was compared with the participant’s elbow extension at the end of Upper Limb Neurodynamic test 1 performed on the opposite upper limb and to elbow extension on the symptomatic side performed with the arm by the side.
RESULTS:
The intensity of pain in Upper Limb Neurodynamic test 1 increased with lateral flexion of the neck to the unaffected side and eased with lateral flexion to the affected side in all participants. A marked restriction of the elbow passive extension range of motion in Upper Limb Neurodynamic test 1 on the affected side (–54.6±17.8°) compared to the unaffected side was found (–7.3±10.7°) (p < 0.001).
CONCLUSIONS:
Restriction of elbow passive extension range of motion at the end of the Upper Limb Neurodynamic 1 test reproduced patients’ familiar adhesive capsulitis associated pain and the pain changed with structural differentiation using cervical lateral flexion. Neurodynamic assessment may need to be considered to assess neural mechanosensitivity in patients with adhesive capsulitis.
In more than four month history of primary adhesive capsulitis: Altered neural mechanosensitivtity was found The elbow extension range of motion angle in Upper Limb Neurodynamic test 1 was restricted at least 10 degrees at the end of the neurodynamic test with no restriction in the neutral arm position. Neural mechanosensitivity may be a clinical finding of late phase of adhesive capsulitis population and may need to be considered in assessment of adhesive capsulitis.
Introduction
Neurodynamic assessment is based on the mechanical continuity of the nervous system and associated biomechanics that result in strain, tension and excursion of neural tissues in response to spinal and limb movements [1–4]. The aim of neurodynamic assessment is to detect increased mechanosensitivity during neurodynamic testing [5]. Biomechanical studies investigating upper limb neurodynamic tests (cadaver and in vivo) have demonstrated that neurodynamic tests produce strain, tension and excursion of upper limb neural tissue [4, 6] providing construct validity to their use for neurodynamic assessment. Evidence of concurrent validity has been shown by studies demonstrating that a combination of ulnar, median and radial nerve biased neurodynamic tests were able to help diagnose cervical radicular pain [7–9]. A positive ulnar nerve test was associated with increased odds of having radicular pain and combined negative ulnar, median and radial biased tests significantly decreased the patient’s odds of having cervical radicular pain.
As neurodynamic tests also affect non-neural tissues, differentiation between neural and non-neural responses is inferred through structural differentiation, where a proximal or distal body part is moved in isolation with the aim of increasing neural strain without adding further strain to the non-neural tissues in the area of symptom provocation [10]. A neurodynamic test is considered positive if the test reproduces the patient’s symptoms [11] and the response changes with structural differentiation [6, 10].
Adhesive capsulitis can develop spontaneously or following immobilisation post trauma. It is characterized by pain and restrictions in both active and passive range of shoulder motion [12]. Risk factors for developing adhesive capsulitis include female sex, aged between 40 and 60 years of age and type I diabetes [13]. The clinical features of adhesive capsulitis include spontaneous onset of symptoms with or without trauma, painful and limited shoulder range of abduction and external rotation, and sleep disturbance due to nocturnal pain [4]. Adhesive capsulitis has been described as having a natural course of recovery that broadly occurs through three stages [11, 14]. An increasingly painful shoulder, with pain on motion and nocturnal pain, is the main symptom in the painful, inflammatory (freezing) stage, which ranges from 10 to 36 weeks [13, 14]. Pain subsides gradually and restricted shoulder range of motion is the main symptom in the second (frozen) stage which ranges from 4 to 12 months [13, 14]. Finally gross shoulder range of motion restrictions resolve over 9 to 15 months (thawing stage) [13, 14]. The recovery course of adhesive capsulitis showed fast improvement of shoulder function and range of motion in early phase (until approximately three months) of adhesive capsulitis, and slow improvement of those in late phase of adhesive capsulitis, respectively [15].
The pathophysiological findings of adhesive capsulitis have been investigated by a number of authors. A decrease of joint capacity in chronic adhesive capsulitis was reported in an arthrographic study [15, 16]. A significantly greater thickening of the synovium and axillary recess capsule was apparent on magnetic resonance imaging in patients with adhesive capsulitis compared to asymptomatic shoulders [18]. McKean [19] highlighted capsuloligamentous contracture of the rotator interval evident on ultrasound and Kanbe [20] reported that synovitis was observed in their adhesive capsulitis arthroscopic findings. A histological study reported an increase of fibroblasts in the capsuloligamentous structures of adhesive capsulitis [21].
As described, pathophysiological descriptions in adhesive capsulitis have identified capsular inflammation and fibrosis/contracture, with recent research also highlighting increased muscle guarding as a component is some shoulder range of motion restrictions [21, 22]. Less is known about nerve involvement in adhesive capsulitis associated symptoms and shoulder range of motion restrictions. Xu et al. [24] demonstrated abnormal nerve growth factor present in the glenohumeral capsule in adhesive capsulitis. A histological study by Hand, Athanasou and Mattheews [25] demonstrated fibroblasts in nerve tissue in patients with chronic adhesive capsulitis. This raises the potential that peripheral nerve or the surrounding, paraneural tissue might be affected during and after the inflammatory phase in adhesive capsulitis, which may lead to some of the clinical findings often found in more than four month history of adhesive capsulitis patients. The pathophysiology of adhesive capsulitis may also be associated with increased neural mechanosensitivity, as reflected in a positive neurodynamic test. The peripheral nerves are sensitized by mechanical elongation and angulation after inflammation [26] which may contribute to the pain and restricted movement found in adhesive capsulitis. Neurodynamic tests may be able to detect a neurodynamic mechanosensitivity to the restriction of shoulder movement after the inflammatory phase in adhesive capsulitis. The purpose of this study was to investigate the findings of neurodynamic assessment in patients diagnosed with adhesive capsulitis on the involved side compared to the uninvolved side.
Methods
Participants
Volunteer patients with adhesive capsulitis were recruited from two institutions through direct contact. All patients who presented at the outpatient department with a diagnosis of adhesive capsulitis were invited to participate in this study. Inclusion criteria included: duration of symptoms greater than four months, i.e. expected to be out of the first inflammatory stage [14], greater than 50%of shoulder range of motion restriction in external rotation at arm by the side of the body compared to the unaffected side [27] greater than 25%of shoulder range of motion restriction in at least two of three directions (i.e. abduction, external or internal rotation) [27] no cervical spine pain, and no restriction of passive elbow range of extension with the arm by the side compared with the other side.
Exclusion criteria included: Adhesive capsulitis due to a traumatic injury [23], Present history of bilateral shoulder disorders, Any history of physiotherapy treatment to the shoulder for this condition [23], and History of disease (e.g. rheumatoid arthritis, osteoarthritis, and malignancy) involving the shoulder, cervical spine, elbow, wrist or fingers [26].
Outcome measure
The Upper Limb Neurodynamic test 1 procedure, developed by Elvey [28] and described by Butler [29], was performed on the participants. The position for Upper Limb Neurodynamic test 1 (i.e. maximum abduction and external rotation of the shoulder, forearm supination and wrist dorsiflexion) [29] was taken and the range of passive elbow extension at the end of range of motion (EEROM) was measured with the arm in this position. EEROM was defined as when further elbow extension was limited by pain in Upper Limb Neurodynamic test 1 [27]. The positive finding of pain was defined as their familiar adhesive capsulitis associated pain with elbow extension of their affected side during the Upper Limb Neurodynamic test 1 [11]. The procedure was performed by two qualified physiotherapists experienced in the performance of this assessment. The reliability of EEROM by two physiotherapists were assessed beforehand (Appendix). Excellent reliability of ICCs (1, 2) were confirmed with 0.95 and 0.97, respectively and ICC (2,2) were confirmed with 0.96.
Procedure
Participants lay supine on a treatment plinth and one of physiotherapists performed passive elbow extension with the arm by the side of the body to ensure full painfree range of motion. The physiotherapist then performed the Upper Limb Neurodynamic test 1 procedure on the participant’s upper limb. The elbow passive extension range of motion was measured using a universal goniometer at the end point of the elbow passive extension range of motion in Upper Limb Neurodynamic test 1. The shoulder and arm position were held constant while the participants were asked to actively laterally flex their neck to both sides for structural differentiation. Participants were asked what effect the neck lateral flexion had on their symptoms (e.g. increased, decreased, no change). The assessment was then performed on the participants’ opposite upper limbs.
Statistical analysis
Sample size estimation to compare two independent groups was undergone according to Hickey et al. [30] and previous Neurodynamic test study [31]. The values of α and β set at 0.01 and 90 %, respectively. The values of Z1-α/2 and Z1-β for sample size estimation were determined according to Hickey et al. (2018) [29]. Sample size in this study was given by,
The number of participants was determined by the sample size estimation with 10 %of the sample size, possible exclusion criteria.
The profile of participants and defferences of the elbow passive extension range of motion between genders were compared using unpaired t-test. Differences of the elbow passive extension range of motion between affected and unaffected sides compared using independent two sample t-test. The restriction of EEROM in Upper Limb Neurodynamic test 1 on the affected side was compared with that of unaffected side using independent two sample t-test. The difference of EEROM in Upper Limb Neurodynamic test 1 was compared between genders. Statistical significance was set at p < 0.01.
Results
At least 23 participants were needed for this study. Thirty six participants with adhesive capsulitis who had volunteered were randomly recruited in this study. One volunteer did not meet the inclusion criteria, the minimum 50%loss of external rotation range of motion in their symptomatic side compared to their asymptomatic side. Thirty five patients with adhesive capsulitis participated in this study (Table 1). There were no significant differences in age or duration of adhesive capsulitis onset between males and females (p > 0.01). All participants reported no resting symptoms. The passive elbow extension range in all patients was not restricted or painful in both affected and unaffected sides when tested with the arm by the side (p = 0.40629) (Table 1). The intensity of pain in Upper Limb Neurodynamic test 1 increased with lateral flexion of the neck to the unaffected side and eased with lateral flexion to the affected side in all participants. Fourteen participants demonstrated restriction of the elbow passive extension range of motion of the unaffected side in Upper Limb Neurodynamic test 1, which ranged from –5 to –30°. A marked restriction of EEROM in Upper Limb Neurodynamic test 1 in the affected side compared to the unaffected side was found (p < 0.001) (Fig. 1), with no statistical differences between genders (p = 0.705 on affected side, p = 0.364 on unaffected side).
Patients’ profile (mean±standard deviation). NRS: Numerical Rating Scale
Patients’ profile (mean±standard deviation). NRS: Numerical Rating Scale
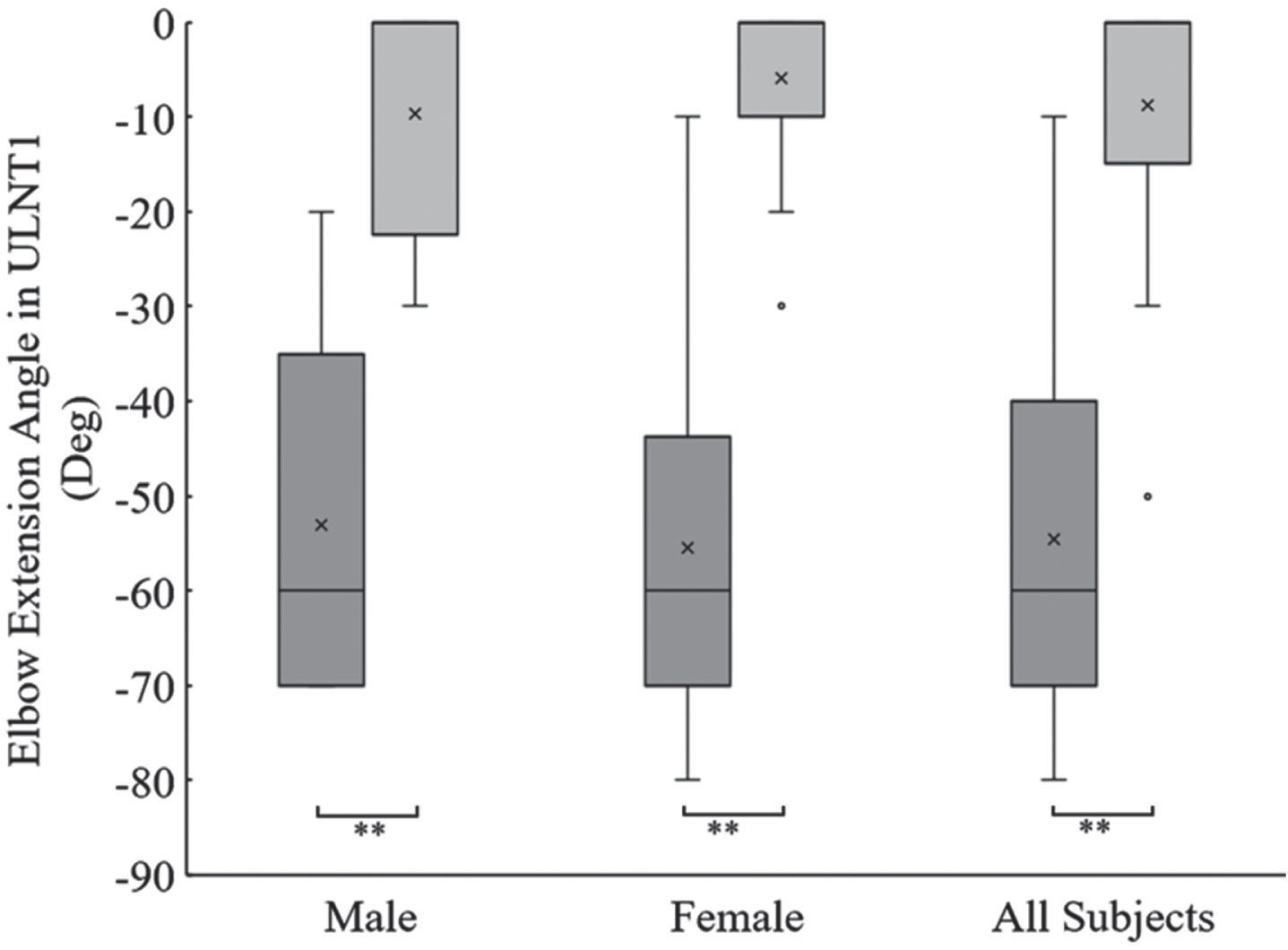
The elbow passive extension range of motion in Upper Limb Nurodynamic test 1 (**: p < 0.01). Dark gray colored box plots represent the elbow passive extension range of motion in affected side. Light gray colored box plots represent the elbow passive extension range of motion in unaffected side. Dots represent outlier of the findings.
Upper Limb Neurodynamic test 1 is common test to assess nerve mechanosensitvity and restriction of neural mobility in neurodynamic test [32] although the test is regarded as testing for median nerve bias. This study aimed to investigate the impairment of neurodynamics, as measured through the use of Upper Limb Neurodynamic test 1, in patients with more than four month history of adhesive capsulitis. During Upper Limb Neurodynamic test 1, the elbow passive extension range of motion of the affected side was restricted compared with that of the unaffected side in all more than four month history of adhesive capsulitis patients. Furthermore, structural differentiation indicated altered mechanosensitivity of the neurodynamic test in the affected upper extremity implicating potential increased neural sensitivity in adhesive capsulitis patients.
EEROM of the affected side in Upper Limb Neurodynamic test 1 was relatively more restricted than EEROM of the unaffected side in adhesive capsulitis patients. Elbow passive extension range of motion is reported as an appropriate outcome in Upper Limb Neurodynamic test 1 [33] and previous studies have indicated that a 10° difference in range was needed to detect a change of range of motion [34]. Our results showed that EEROM differences between the affected and the unaffected side in the Upper Limb Neurodynamic test 1 end position ranged from 10 to 70 degrees for adhesive capsulitis patients. The restriction of EEROM in Upper Limb Neurodynamic test 1 was confirmed regardless of genders. All subjects demonstrated no restriction of passive elbow range of motion when tested with the arm by the side, and response to structural differentiation by which their symptom aggravated and eased when tested with contralateral and ipsilateral cervical flexion, suggesting that the elbow passive extension range of motion differences may indicate increased neural mechanosensitivity.
This study used a universal goniometer for the elbow passive extension range of motion as this method of measuring range of motion has been shown to have high reliability, with a range of motion error of between six to nine degrees [31, 32]. We therefore judged a greater than ten degree restriction in elbow extension as positive during the Upper Limb Neurodynamic test in this study.
The positive findings were defined as a reproduction of their familiar shoulder pain associated symptom and change of their symptom with structural differentiation during Upper Limb Neurodynamic test 1 [11]. This study confirmed provocation of the associated shoulder symptom and the positive finding of structural differentiation on the affected side in all patients. Structural differentiation was carried out to minimise the potential for a false positive finding with neurodynamic assessment performed without differentiation [27, 34]. All patients in our study demonstrated altered mechanosensitivity with structural restriction. Neurodynamic tests are not utilized in adhesive capsulitis while the other non-neural disorders are assessed using neurodynamic tests [3, 35]. In chronic stage, the neurodynamics changes in neck pain without neuropathic condition [3, 31]. It is presumed that neurodynamics is restricted in adhesive capusulitis, non-neural disorder, even more if passed inflammatory stage. The altered neural mechanosensitivity was reported as a result of four week immobilized period in healthy participants [36]. The neural mechanosensitivity in patients with adhesive capsulitis could be changed as resulted of less shoulder motion due to the glenohumeral joint contracture although adhesive capsulitis is non neuropathic disorder. The results of this study suggest that the restriction of the elbow extension range of motion, neural associated symptom provocation and change of this symptom with structural differentiation were positive findings for patients with adhesive capsulitis in the neurodynamic test.
Limitations of this study included the lack of reliability testing of the performance of the Upper limb Neurodynamic test 1. This study omitted repeated neurodynamic testing for reliability to avoid aggravation of the patients’ symptoms. Moreover, the elbow passive extension range of motion angle might differ with repeated Upper Limb Neurodynamic testing as the testing maneuver could mobilize the tissue restricted and alter mechanosensitivity. Although this study did not confirm the reliability of the elbow passive extension range of motion, a significant decrease of the elbow passive extension range of motion in Upper Limb Neurodynamic test 1 was demonstrated on the affected side. A previous study demonstrated that the elbow passive extension range of motion in Upper Limb Neurodynamic test 1 was reliable as an outcome measure [33]. The differences of the elbow extension angle in this study could indicate nerve involvement (e.g. mechanosensitivity) in more than four month history of adhesive capsulitis.
This study assessed the results from a neurodynamic test, the Upper Limb Neurodynamic test 1, in patients with more than four month history of adhesive capsulitis. The findings suggest that there may be altered neurodynamic mechanosensitivity in these patients. The pathological course of adhesive capsulitis affects the tissues surrounding the shoulder, including the capsule, bursa and muscle, and, possibly also neural structures.
Conclusion
This study confirmed the presence of altered neurodynamic mechanosensitivity in the affected side in more than four month history of adhesive capsulitis patients. The elbow passive extension range of motion in Upper Limb Neurodynamic test 1 was restricted by at least 10 degrees whilst passive range of elbow extension with the arm by the side was not restricted. Lateral cervical flexion away from the affected side aggravated their familiar adhesive capsulitis pain and lateral cervical flexion toward to the affected side eased their pain supporting a neurodynamic mechanosensitivity component to their clinical presentation. Neurodynamic testing may need to be considered to assess the possible neural mechanosensitivity in patients with more than four month history of adhesive capsulitis. Further work is required to investigate the repeatability of this finding in a larger population and the effect of neural mobilization treatment for this impairment in patients with adhesive capsulitis.
Footnotes
Acknowledgments
We would like to give my gratitude to the patients who agreed to participate this study, our colleague who took part in the blinded analyzer for statistical analysis, and Nobuhara hospital and Pixy orthopaedic clinic who provided the opportunity to do this study.
Conflict of interest
All authors declare that there are no conflicts of interest which may affect the results of this study.
Ethical considerations
The study was approved by the Human ethics research committee of the Nobuhara hospital (Approval no.2401).
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.