
Abstract
BACKGROUND:
Chronic low back pain (CLBP) significantly impairs function and productivity, emphasizing the need for effective solutions, with virtual reality (VR) emerging as a novel alternative for management.
OBJECTIVE:
The aim of this systematic review and meta-analysis was to examine the effects of VR interventions on pain, disability and kinesiophobia, compared with other therapeutic interventions in CLBP patients.
METHODS:
In July 2023, we searched PubMed and PEDro databases for studies that examined the effects of VR interventions on pain, disability or kinesiophobia in adults with CLBP. Using a meta-analysis with a random-effects model, we derived the standardized mean difference as the pooled effect.
RESULTS:
We found 33 studies, 22 of which were eligible for meta-analysis. Most studies were of good quality, with 12/22 reaching a score between 6 and 8 points on the PEDro scale. VR demonstrated superior results compared to placebo (SMD = –1.90; 95% CI = –3.60 to –0.20; p = 0.03), no intervention (SMD = –1.66; 95% CI = –2.49 to –0.83; p < 0.001), exercise (SMD = –0.61; 95% CI = –1.06 to –0.16; p = 0.008), and VR combined with physical therapy showed greater efficacy than exercise combined with physical therapy (SMD = –1.42; 95% CI = –2.33 to –0.52; p = 0.002) in pain intensity outcome. However, no significant differences were found for disability outcome.
CONCLUSION:
VR interventions are superior to non-VR interventions in terms of improving pain intensity in CLBP patients, but not also for disability outcomes. Further research is needed for conclusive insights into VR’s efficacy.
Introduction
Low back pain (LBP) is one of the most common reasons for which patients seek medical attention [1] and is defined as chronic when lasting longer than three months or exceeds the expected duration of tissue healing [2]. In most cases, it is not possible to identify the specific nociceptive cause of CLBP, which is why it is classified as nonspecific [4]. The economic impact of CLBP results from the gradual loss of function that leads to decreased work productivity, treatment costs, and disability payments [5]. Given this high burden of care, it is important to develop effective treatment options for patients with CLBP. There are numerous conservative treatment options for the management of CLBP, including: cognitive behavioural therapy, patient education, McKenzie exercises, yoga, aerobic exercise, manual therapy, and analgesic drugs [6, 7]. However, because of the multifactorial aetiology of CLBP, treatment of this condition is difficult, and many interventions have limited efficacy [8]. In addition to these non-surgical options, virtual reality (VR) is a new alternative for the management of CLBP [7].
VR technology allows the user to feel a sense of presence in a computer-generated three-dimensional virtual world in such a way that the user feels as if he is a part of that world [9–11]. The simulated environments created by VR can give a varying illusion of presence and realism. The more real the virtual environment appears to the user, the greater the so-called immersive experience. The immersive experience is proportional to the number of stimulated physiological senses, the extent of interaction with the virtual environment and the isolation from external stimuli (e.g., light) [12]. In healthcare, VR has been shown as an effective treatment option for managing acute pain, while the body of research for chronic pain is still in the early stages [13]. For chronic patients, VR technology can be used both for cognitive rehabilitation, providing a medium for transferring the principles of cognitive behavioral therapy or pain neuroscience education [62], and for physical rehabilitation, where the patient performs exercises in a virtual environment [63]. Patients can benefit from VR technology, due to its distraction mechanism which is leaving less cognitive capacity available to process pain signals [14]. Furthermore, with involving patients in their recovery in a fun, attractive, and interactive way, VR contributes to motivation and adherence in the rehabilitation process [15–17].
In the field of CLBP, previous systematic reviews showed promising results for the use of VR technology in CLBP rehabilitation. Brea-Gómez et al. [6] found that VR interventions can significantly reduce pain intensity and kinesiophobia (i.e., excessive and irrational fear of physical activity, caused by fear of re-injury) in patients with CLBP in the short and long term compared to no VR interventions. However, they found no significant differences in disability outcome [6]. A more recent systematic review of randomized and quasirandomized controlled trials conducted by Choi et al. [60] focused only on pain outcomes and found that VR-based interventions had moderate to strong evidence for pain reduction compared with conventional interventions. However, research on VR in CLBP is growing rapidly, and recent reviews have not included the latest research or did not analyse the effects of VR on a broader range of outcomes such as disability and kinesiophobia. Therefore, the novelty of our systematic review with meta-analysis lies in its inclusion of the latest studies and its comprehensive analysis of VR effects on pain, disability, and kinesiophobia. In accordance with previous studies, we hypothesised that VR would show a positive effect on pain intensity and kinesiophobia compared with other interventions, while we anticipated no significant differences in disability outcomes. This review aims to build upon previous papers by providing a current and extensive evaluation of VR’s efficacy, thereby contributing to the body of evidence supporting its use in CLBP management.
Methods
Search strategy and inclusion criteria
The literature search was performed in July 2023. Three authors independently performed all search steps, and any disagreements were resolved by discussion, with D.M.I. (supervising researcher) having the final say. We searched the PubMed and PEDro databases. For PubMed, we used the following search strategy: (“virtual reality” OR “video games” OR “wii” OR “horse simulator”) AND (“back pain” OR “lumbar pain”). For PEDro, individual combinations of words, such as “virtual reality back pain”, “video games back pain”, “horse simulator back pain” and “wii back pain” were used. In addition, we reviewed the reference lists of identified systematic reviews on the topic and performed an additional non-systematic search of the GoogleScholar database. The records were imported into Mendeley (version 1.19.8) to remove the duplicates, and then exported into Microsoft Excel software for further examination.
The inclusion criteria, structured according to the PICOS tool [18], were determined as follows.
Data extraction
The data extraction was carried out independently by all authors and disagreements were resolved through additional discussion. The extracted data included: (a) baseline, post-intervention and follow-up data (means and standard deviations (SD)) for all eligible outcome measures for both VR and control groups (percent changes were considered instead of pre-post data when available) (b) baseline demographics of patients (gender, age, body height, body mass, body mass index); (c) intervention characteristics (VR intervention description, duration of the intervention, weekly frequency, volume (number of exercises, sets, and repetitions), breaks, and supervision). Data were collected into Microsoft Excel 2016 (Microsoft, Redmond, WA, USA). If the data were presented in a graphical form, we used GetGraphDataDigitalizer software (version 2.26.0.20) to obtain the means and SD. In case of missing data, the authors of the articles were contacted via e-mail and/or ResearchGate. A reminder was sent after 14 days, and if no reply was received after the second inquiry, the data was considered irretrievable.
Assessment of the quality of the included studies
All authors evaluated the quality of the studies included in the meta-analysis using the PEDro scale which assesses study quality based on ten items [19] and potential disagreements were resolved by discussion. Studies scoring from 9 to 10 were considered as “excellent,” 6 to 8 as “good,” 4 to 5 as “fair,” and <4 as “poor” quality. The PEDro scale was selected as it was specifically developed to evaluate the quality of clinical trial studies investigating PT interventions [20].
Data analysis
The meta-analysis was carried out in Review Manager (Version 5.3, Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, London, UK). Since there is still no consensus on the minimal number of studies required for a meta-analysis [21], we performed the analyses when two or more studies could be included. Before the results were entered into the meta-analytical model, the pre-post differences and pooled SD were calculated according to the following formula
Results
General overview of the search results
We found 33 studies that were included in the review, 22 of which were eligible for the meta-analysis. The detailed summary of the search process is shown in PRISMA flow diagram in Fig. 1. Due to the lack of studies that observed changes in kinesiophobia that had comparable study design (i.e., the same intervention or combination of interventions in experimental and control groups) meta-analyses were performed only for disability and pain intensity outcomes. However, the effects of VR interventions on kinesiophobia were included in the narrative review.
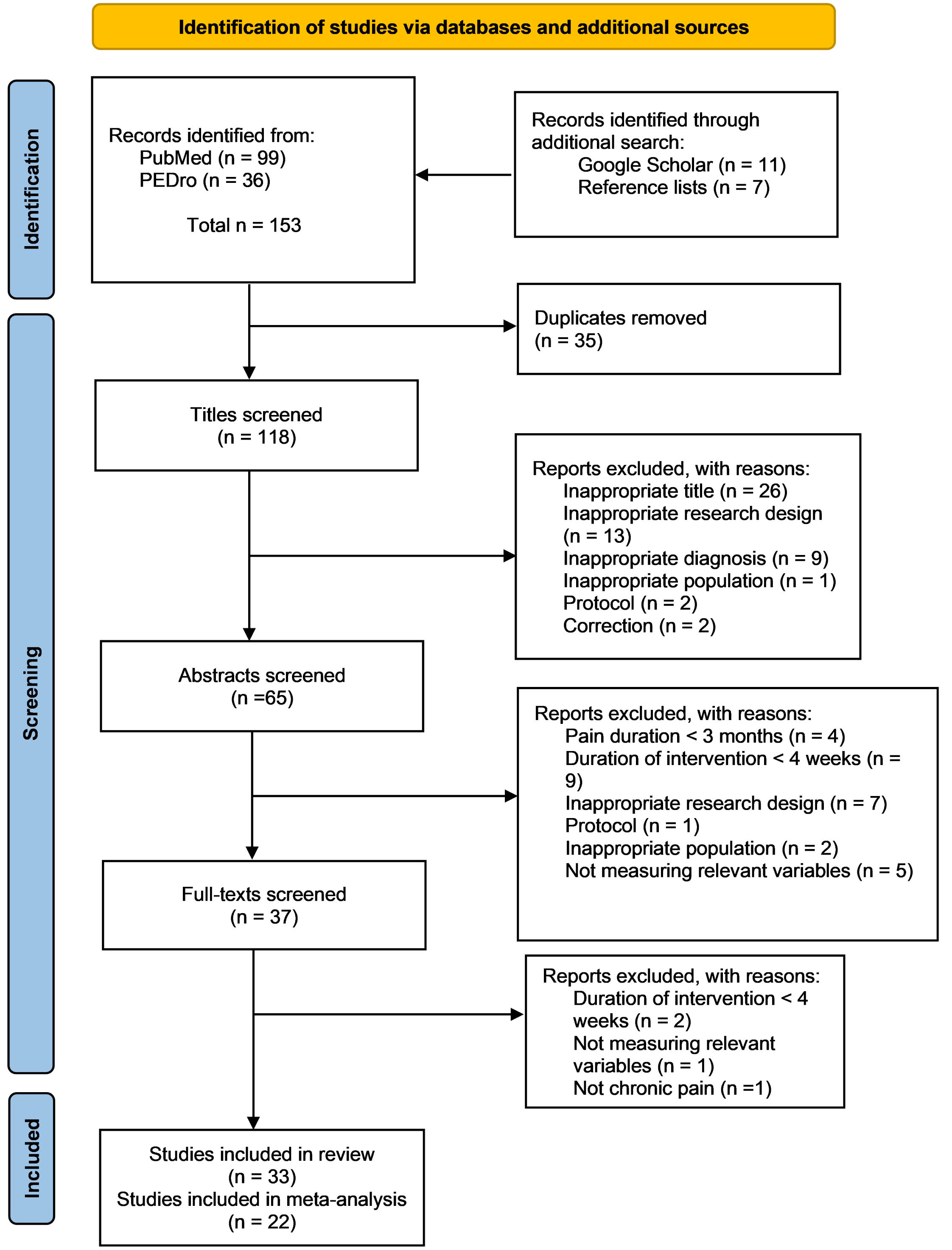
Overview of article search and study selection.
Both men and women participated in most studies included in our review. However, eight studies [22–29] included male patients only, while four studies [30–33] included exclusively female patients. Two studies [34, 35] did not specify the gender of the patients, and for one [36] only abstract was available in which gender was also not mentioned. Although all studies examined adult patients, some included younger adults (under 30 years of age) [22–27, 34] and some older adults (older than 60 years) [30–32, 37]. Due to unavailability of the full text, the age range of patients in the study by MacIntyre et al. [36] is considered to be unknown.
Interventions
The duration of interventions in the studies ranged from four to 18 weeks and the weekly frequency of sessions from two to seven. In most studies, patients were included in a non-immersive VR training intervention. VR has been used in various forms: Nintendo programs and consoles [30, 39], horse simulator riding [27, 40], VR programs with VR glasses [28, 41–44], other systems similar to VR, but without video games, based on biofeedback [45] and other types of video games with sensors and a monitor [22, 46–49]. When the intervention was carried out on a horse simulator, participants sat on an indoor riding machine, that simulated riding a real horse and looked at a screen displaying the visual information of riding a real horse. In studies where exercises were performed with a VR, the VR game was usually controlled by moving the trunk in all possible movements. When VR involved cognitive behavioural therapy, pain neuroscience education or biopsychosocial education was delivered through VR glasses or a monitor. In experimental groups, VR was either a sole intervention or combined with standard PT or exercise interventions. Standard PT included a combination of some of the following methods: hot pack therapy, therapeutic ultrasound, interferential electrotherapy, exercise program, manual therapy and pain neuroscience education. In studies where VR was compared to placebo VR, placebo meant either a non-immersive 2D VR or, if the experimental intervention was training on the horse simulator, placebo meant that the participants sat on the horse and just watched the video without training. In all studies, patients had to report the presence of LBP for at least 12 weeks. However, to provide a comprehensive review, we also included studies in which the duration of LBP was described as chronic only [30, 46]. The details of each study are shown in Table 1.
Characteristics of included studies
Characteristics of included studies
n: numerus; EG: experimental group; CG: control group; VR: virtual reality; SD: standard deviation; PT: physical therapy; ODI: The Oswestry Disability Index; VAS: The visual analog scale; NPRS: The Numeric Pain Rating Scale; RMDQ: Roland-Morris Disability Questionnaire; TSK: Tampa Scale of Kinesiophobia. *Only abstract available.
The assessment of study quality according to PEDro Scale is shown in Table 2. Most studies were of good quality, with 12/22 reaching a score between 6 and 8 points on the PEDro scale. One additional study was of poor quality (3 points) and 9 were of fair quality (4-5 points).
Assessment of study quality with Pedro Scale
Assessment of study quality with Pedro Scale
Two studies compared VR with a placebo VR for ODI outcome (54 and 57 patients in VR and placebo VR groups, respectively). The pooled effect strongly favoured VR (SMD = –3.12; 95% CI = –8.14 to 1.90), but the two studies were highly heterogenous (I2 = 98%) and the effect was not statistically significant (p = 0.220).
Two studies compared VR with no intervention, one for ODI and one for RMD outcome (44 and 39 patients in VR and control groups, respectively). The pooled effect favored VR (SMD = –0.24; 95% CI = –0.68 to 0.19; I2 = 0%) but was not statistically significant (p = 0.270).
Three studies compared VR with exercise for ODI outcome (67 and 69 patients in VR and exercise groups, respectively). The analysis indicated no difference between the two interventions (SMD = –0.05; 95% CI = –0.57 to 0.48; I2 = 58%; p = 0.860).
Pain intensity – VR vs. Placebo VR
Three studies compared VR with a placebo VR (143 and 147 patients in VR and placebo VR groups, respectively) for pain intensity outcome (studies used NRS, VAS and DVPRS measures). The pooled effect was statistically significant and strongly favoured VR (SMD = –1.90; 95% CI = –3.60 to –0.20; p = 0.03), however, the studies were highly heterogenous (I2 = 96%).
Pain intensity – VR vs. no intervention
Six studies compared VR with no intervention (110 and 103 patients in VR and control groups, respectively). Included studies used NRS and VAS measures for pain intensity. The pooled effect strongly favoured VR (SMD = –1.66; 95% CI = –2.49 to –0.83; p < 0.001). However, the heterogeneity between the studies was high (I2 = 84%).
Pain intensity – VR vs. exercise
Five studies compared VR with exercise (98 and 100 patients in VR and exercise groups, respectively). Included studies used NRS and VAS measures for pain intensity. The effect favoured VR interventions over exercise (SMD = –0.61; 95% CI = –1.06 to –0.16; p = 0.008) for pain intensity, with moderate heterogeneity between the studies (I2 = 57%). Two studies also compared VR with exercise at eight weeks and six months follow-up period (35 and 35 patients in VR and exercise groups, respectively). In this case, the overall effect still favoured VR, but was not statistically significant (SMD = –0.84; 95% CI = –3.07 to 1.39; p = 0.460).
Pain intensity – VR combined with exercise vs. exercise alone
Two studies compared VR interventions combined with exercise therapy with exercise interventions alone (26 and 23 patients in each group, respectively), one for VAS and one for NRS outcome. The pooled effect indicated no difference between the interventions in pain intensity (SMD = –0.08; 95% CI = –0.78 to 0.62; I2 = 32%; p = 0.820).
Pain intensity – VR combined with PT vs. exercise combined with PT
Seven studies compared VR interventions combined with PT with exercise therapy combined with PT for VAS outcome (142 and 142 patients in VR combined with PT and exercise groups, respectively). The effect strongly favoured VR combined with PT over exercise combined with PT (SMD = –1.42; 95% CI = –2.33 to –0.52; p = 0.002), with moderate to high heterogeneity between the studies (I2 = 88%). Four studies also compared VR combined with PT with exercise combined with PT during a follow-up (71 and 72 patients in VR combined with PT and exercise combined with PT groups, respectively). In this case, the overall effect was still very large and favoured VR (SMD = –2.01; 95% CI = –2.42 to –1.60; p < 0.001; I2 = 0%).
Discussion
The aim of this systematic review with meta-analysis was to investigate the effects of VR on pain, disability, and kinesiophobia compared with other therapeutic interventions in CLBP patients. Thirty-three studies were included in this review and twenty-two were eligible for meta-analysis. In meta-analyses, VR was compared to placebo VR, no intervention, exercise, or PT combined with exercise. The experimental groups included stand-alone VR interventions or combined VR interventions with exercise or PT. We were able to partially confirm our hypothesis regarding the effects of VR on pain intensity and fully confirm our hypothesis regarding the effects on disability. In the short term, VR interventions were found to be superior than placebo VR, no intervention, exercise and exercise combined with PT in terms of pain intensity. However, the meta-analysis showed no significant difference in pain reduction between VR combined with exercise and exercise only. There were also no significant differences in disability outcomes between VR and non-VR interventions. Due to the high heterogeneity among studies and the small number of studies included in some meta-analyses, our evidence is of low quality, which calls for further research in the future.
Effects on pain intensity
Pain intensity was assessed in all studies included in the meta-analysis. In the short term, VR demonstrated significant advantages over placebo VR, no intervention, or exercise in terms of pain outcomes. In the short and long term, addition of VR to PT showed better results regarding pain intensity outcomes compared with PT combined with exercise. However, the results should be interpreted with caution. While in the studies that found superiority of VR, the effect size, represented by the standardized mean differences (SMD), appears substantial (SMD ≥0.61), the wide confidence intervals (CI) indicate potential unreliability in the estimation of the true effect or substantial heterogeneity between studies. On the contrary, VR combined with exercise therapy was not superior in reducing pain intensity than exercises alone. Six single-arm studies that were excluded from the meta-analysis showed a significant pain reduction after VR intervention [28, 49]. In a recent experimental study by Afzal et al. [50], a three-week intervention of VR combined with PT resulted in a significant improvement in pain levels as well. The mechanisms underlying pain reduction due to VR interventions primarily involve creating distraction from the painful area, engaging attention resources (i.e., focus shifting), and blocking external stimuli [51]. This increases pain tolerance and threshold, while also decreasing pain intensity and rumination [52, 53]. Long-term pain management can be achieved by skill-building through VR, which can empower patients to build capacities necessary to regulate their response to painful stimuli and take an active role in their own care [9]. Moreover, long-term VR use is expected to induce neuroplastic changes in sensory and motor brain regions [54]. While our results suggest that VR can be used to reduce pain intensity in CLBP patients, the question remains whether the use of VR is preferable to exercise therapy in reducing pain levels. Based on our study, VR and non-VR exercises have similar long-term effects on pain reduction in CLBP patients. Furthermore, our meta-analysis showed similar short-term effects on pain improvement between VR combined with exercise and exercise only interventions. In addition, the use of VR in training can have certain additional side effects that we need to keep in mind when prescribing such training, and these are: dizziness, headaches and motion sickness. VR can cause visually induced motion sickness, as the sensory information often contradicts the expected information from body movement, which is primarily due to visual information rather than the vestibular sense or proprioception [67]. Further research is needed to draw definite conclusions regarding the benefits of using VR interventions compared with exercise for pain management in CLBP patients.
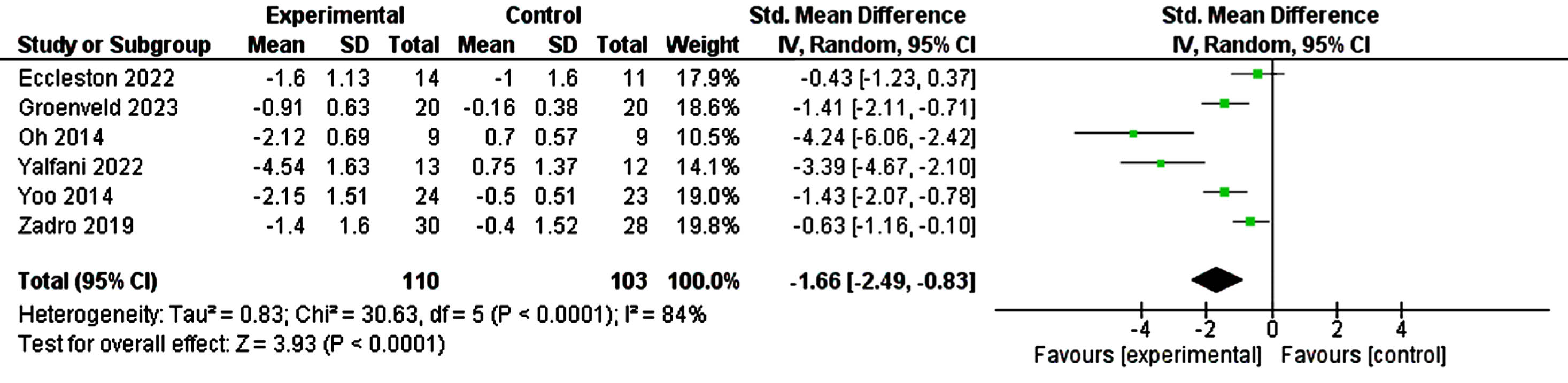
Comparison of virtual reality with no intervention for pain scores.

Comparison of virtual reality with exercise for pain scores.
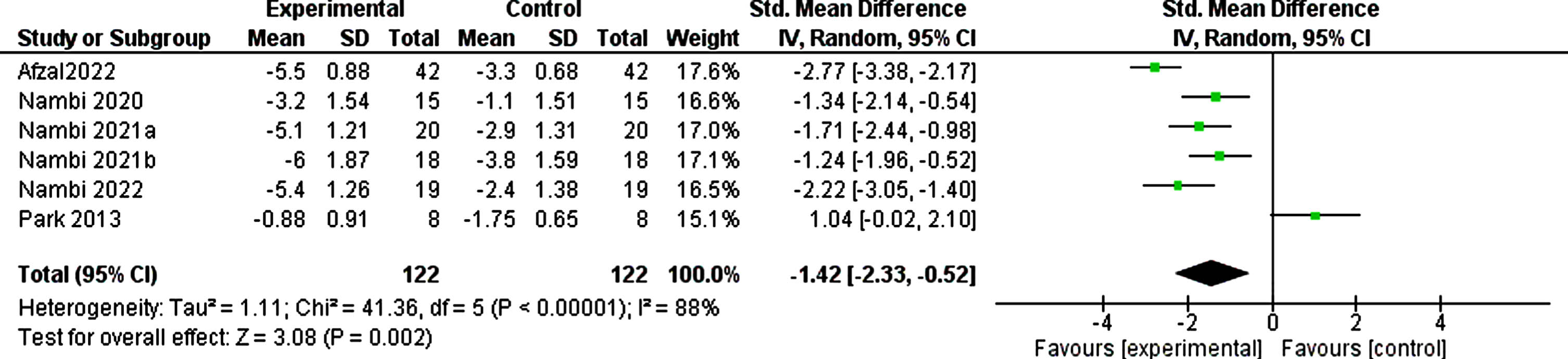
Comparison of virtual reality combined with physical therapy with exercise combined with physical therapy for pain scores.
Six studies included in the meta-analysis assessed disability outcomes in patients with CLBP. Consistent with a previous systematic review Brea-Gómez et al. [6], VR interventions were no better than no VR interventions in improving disability in the short term. VR showed similar effects on disability compared with placebo VR, exercise, or no intervention. However, it should be noted that the pooled effect favoured VR in all meta-analyses related to disability outcome. It is possible that significant effects would be obtained if more studies were included in the meta-analysis. Two single armed studies [48, 49] that were not included in our meta-analyses found a significant improvement in disability after VR intervention, whereas one study [33] reported a non-significant disability improvement overtime. Studies that examined the effects of VR interventions lasting less than four weeks on CLBP patients also found conflicting results. Some report a significant impact on disability after the intervention [50], while others do not [55]. Although our results do not confirm significant differences regarding the short-term improvements in disability between VR intervention and non-VR interventions, the use of VR in patients with CLBP may still be useful in the long term, as it may contribute to a better patient compliance [56, 57].
Effects on kinesiophobia
Due to the lack of studies that observed changes in kinesiophobia that had comparable study design, meta-analyses could not be performed for kinesiophobia outcomes. However, we included nine studies that reported changes in kinesiophobia in the narrative review. As a stand-alone intervention, VR has been shown to result in greater improvements in kinesiophobia outcomes compared with placebo VR or standard treatment [42]. Similarly, studies report greater improvements in kinesiophobia levels following combined VR interventions with PT or patient education when compared with non-VR interventions (exercise therapy combined with PT or patient education) [22, 58]. Kinesiophobia reduction through VR interventions can be achieved by patients paying less attention to fear and shifting attention from harmful stimuli to more pleasant experiences [59]. However, when VR was compared to no intervention, [38] found no significant between-group differences in kinesiophobia. No significant improvements in kinesiophobia post VR intervention were seen in the majority of single-armed studies [39, 44]. Given the inconsistent results between studies and comparisons of VR interventions with different control groups, it is difficult to recommend a VR intervention over other non-VR interventions to improve kinesiophobia levels in patients with CLBP.
Strengths and limitations
This review represents an update of our understanding of the effects of VR treatment in CLBP by including a meta-analysis of recently published studies not included in previous meta-analyses. Furthermore, in our meta-analyses, we examined the effects of VR on additional outcomes such as disability and kinesiophobia, which were not analysed in the most recent meta-analysis by Choi et al. [60]. According to the PEDro scale, most studies included in our meta-analysis (12 of 22) were of good methodological quality. However, most meta-analyses (five of eight) were small and included only two to three studies. One of the main limitations was the high heterogeneity of the included studies. Studies differed primarily in the type of VR used, sample size, duration of intervention and gender and age of the participants. Almost a third of the included studies (10 of 33 studies) had a sample size of less than 30. In addition, the average age of participants in 9 of the 33 included studies was below 30 years, which does not represent the population with the highest incidence of CLBP, which is between 50 and 60 years old [66]. It is possible that different conclusions would have been drawn if the studies had been more homogeneous or more research was available for inclusion in the meta-analysis. In addition, if more research had been available in this area, we could have included more studies in our meta-analysis, which could also have led to different results.
Conclusion
The aim of this systematic review and meta-analysis was to examine the effects of VR on pain, disability, and kinesiophobia compared with other therapeutic interventions in CLBP patients. We found short-term superiority of VR interventions over non-VR interventions in terms of pain intensity. However, no significant differences were found in disability outcomes between VR and non-VR interventions. Furthermore, the inconsistent results across studies prevent us from recommending VR interventions over other non-VR interventions for changes in kinesiophobia in patients with CLBP. Due to the high heterogeneity between studies and the small number of studies included in some meta-analyses, our evidence is of low quality, which calls for further research in the future. Future research should focus primarily on the population that best represents patients with CLBP, i.e. patients older than 50 years. At the same time, more research would be needed on the use of VR in CLBP, investigating the effects on kinesiophobia.
Footnotes
Acknowledgments
The authors were supported by the Slovenian Research and Innovation Agency through the research program KINSPO - Kinesiology for the effectiveness and prevention of musculoskeletal injuries in sports (P5-0443). The funder played no role in conceptualization of the article and decision to publish.
Data availability
Raw data may be obtained by request to the corresponding author.
Conflict of interest
The authors have no conflict of interest to report.