
Abstract
Objectives
to explore the patient experience of rehabilitation following a COVID-19 infection during the first wave of the pandemic.
Methods
All inpatients admitted for rehabilitation following COVID-19 infection or those who experienced COVID-19 infection while inpatients between March-August 2020 were screened for eligibility. Those meeting the eligibility criteria were invited to participate in a semi- structured interview, which were undertaken 3–6 months post discharge. Interviews were conducted by telephone, were audio recorded and transcribed verbatim. Interviews were analysed using Braun and Clarkes thematic analysis.
Results
A total of 23 participants participated in the study. Mean age of patients was 68.8(11.8) years, and 12 patients had a critical care admission prior to their admission for rehabilitation. Four key themes were identified from the qualitative data: (i) Acute period of symptoms after COVID-19 diagnosis, (ii) Post-acute inpatient rehabilitation experience, (iii) Transitioning home after hospitalisation with COVID-19 infection and (iv) Long Covid syndrome. Further subthemes were identified within these themes.
Conclusion
The lived experience of COVID-19 from the acute stages, through rehabilitation and transitioning home and into society varied hugely between individuals at all stages, which should be reflected in our management of this patients. Some participants expressed feeling lonely and stigmatised during their rehabilitation, which is avoidable and should be considered in future pandemics and healthcare delivery. The role of physiotherapists during rehabilitation grew from providing physical rehabilitation to being a central part of the patients social support network. This research provides important learnings for healthcare delivery and training of healthcare providers.
1. Introduction
The World Health Organisation declared COVID-19 a global pandemic in March 2020 and declared it ended in May 2023 [1]. While COVID-19 is no longer considered to be a pandemic it is still prevalent, with approximately 500 cases reported each week in Ireland [2].
The individual experience of COVID-19 varies significantly with some people experiencing no symptoms, mild illness (symptoms include sore throat, fever, headache, nausea, vomiting, diarrhoea, muscle pain, loss of taste and sense of smell), moderate illness (show evidence of lower respiratory disease on assessment), severe illness (symptoms of respiratory distress including increased respiratory rate, low oxygen saturations, reduced arterial oxygen) or critical illness (respiratory failure, septic shock, and/or multiple organ dysfunction) [3]. Risk of developing a more severe illness and requiring hospitalisation depends on a number of factors including underlying comorbidities, increasing age (>65), lower physical activity levels and who smoke cigarettes are an increased risk of more severe illness [3].
The direct effects of COVID-19 on the body systems result in a hyper inflammatory state which can cause multiple organ dysfunction [4]. This hyper inflammatory state combined with bed rest and immobility and reduced nutritional status (as per the symptoms of nausea, vomiting, diarrhoea and loss of taste and sense of smell) are risk factors for acute sarcopenia [5]. It therefore became apparent during the first wave of the pandemic that some patients recovering from COVID-19 would require rehabilitation and a designated COVID-19 rehabilitation centre was required. Clontarf Hospital is a 160-bed rehabilitation hospital in Ireland and serves a number of acute hospitals in the Dublin area. It was designated as a COVID-19 rehabilitation centre in April 2020. Guidelines for the rehabilitation of patients from COVID-19 were published [6, 7]: (i) reduced patient contact time (ii) staff to wear full personal protective equipment (PPE) (iii) no to access to the physiotherapy gym (iv) no group classes (v) social distancing in wards (vi) no visitor policy. This created a unique set of challenges for rehabilitation and the impact of these on individuals’ recovery and experience of rehabilitation is not clear. A designated COVID-19 rehabilitation centre was required.
The aim of this study was to explore the patient experience of rehabilitation following a COVID-19 infection during the first wave of the pandemic (March 2020-August 2020).
2. Methods
A qualitative study design was adopted for the study. Patients admitted to Clontarf Hospital received daily physiotherapy treatment which consisted of 1 : 1 sessions which were tailored based on assessment findings and patient goals for rehabilitation. Treatments focused on upper and lower limb strengthening, one-to-one pulmonary rehabilitation for patients with respiratory compromise, stairs practice, mobility practice, balance exercises and patients were also provided with individualised exercise programmes. Ethical approval was obtained from Clontarf Hospital Ethics Committee; Ethics Approval number EC01/20. Patients admitted to Clontarf hospital with a diagnosis of COVID-19 between March 2020-August 2020 or any patient who contracted COVID-19 as an inpatient in Clontarf Hospital during this time period were screened for inclusion by the physiotherapy team.
Patients were excluded from the study if they had a significant cognitive impairment as per their inpatient medical notes, if they did not complete their rehabilitation at Clontarf Hospital for example discharged to another care facility or if there was a full set of missing outcome measure data on either admission or discharge rendering an inability to determine impact of rehabilitation.
A study information pack was sent by post to each of the potential patients including a patient information leaflet about the study, two consent forms and a stamped, addressed envelope to return the consent form. Follow-up phone calls were made to each of the potential patients to give the opportunity to ask any questions about the study.
This study was not funded by any individual or organisation.
2.1. Data collection
Each patient was invited to participate in a short qualitative, semi-structured interview about their experience of COVID-19, their physiotherapy rehabilitation in post-acute rehabilitation hospital and whether or not they felt their needs were met. The interview script is available in Table 1.
Semi structured interview script questions.
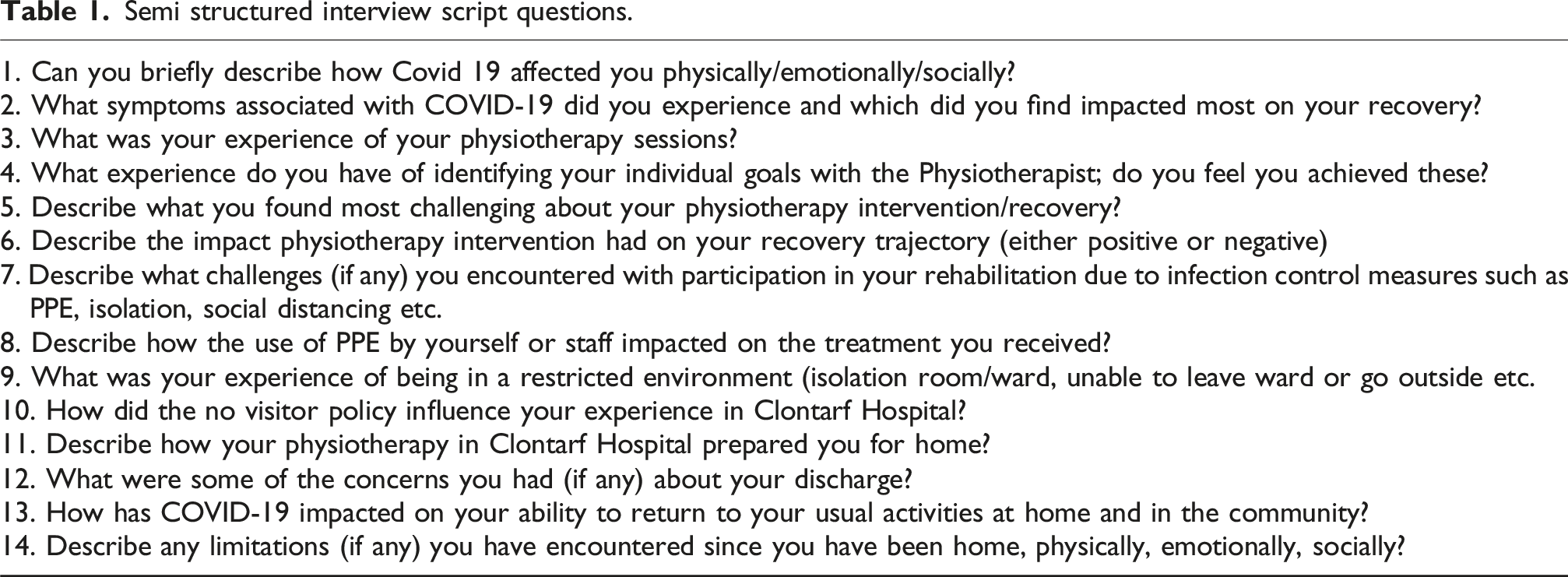
A qualitative interview script was developed and the interviews were conducted over the phone by a member of the research team (SG, RM, AC). All interviews were conducted between three and six months post discharge from Clontarf Hospital. The interviews were audio recorded and transcribed verbatim.
2.2. Data analysis
The interviews were analysed using Braun and Clarke [8] framework for thematic analysis. The steps involved in the framework are listed in Table 2.
Braun and Clarke Steps for thematic analysis.
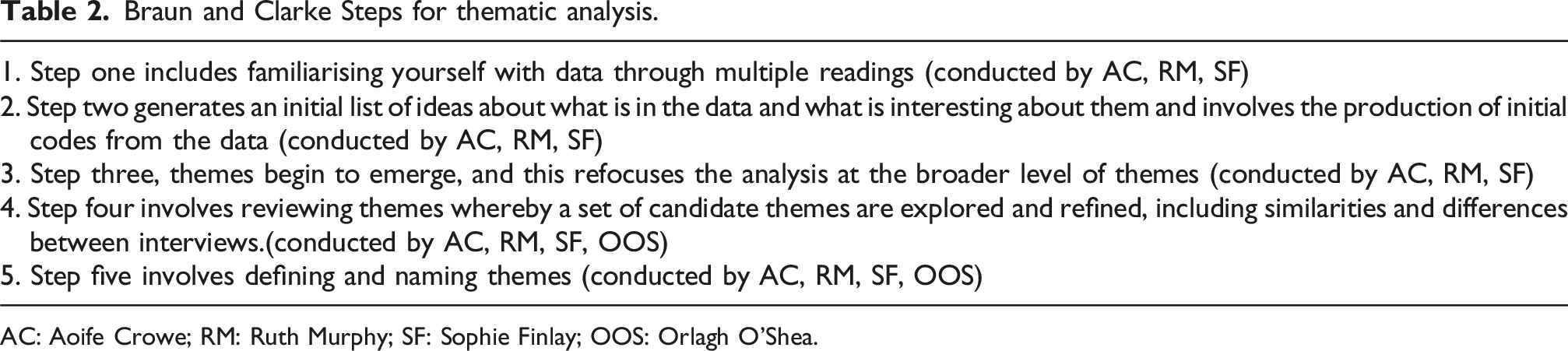
AC: Aoife Crowe; RM: Ruth Murphy; SF: Sophie Finlay; OOS: Orlagh O’Shea.
3. Results
3.1. Sample demographics
One hundred and fourteen patients were screened for inclusion, 56 were eligible for participation and 23 consented to participate. Details of screening and reasons for non-participation are available in Fig. 1. The mean age of patients was 68.8 (11.8) years, there were 11 females and 12 patients had a critical care admission prior to their admission to Clontarf for rehabilitation.
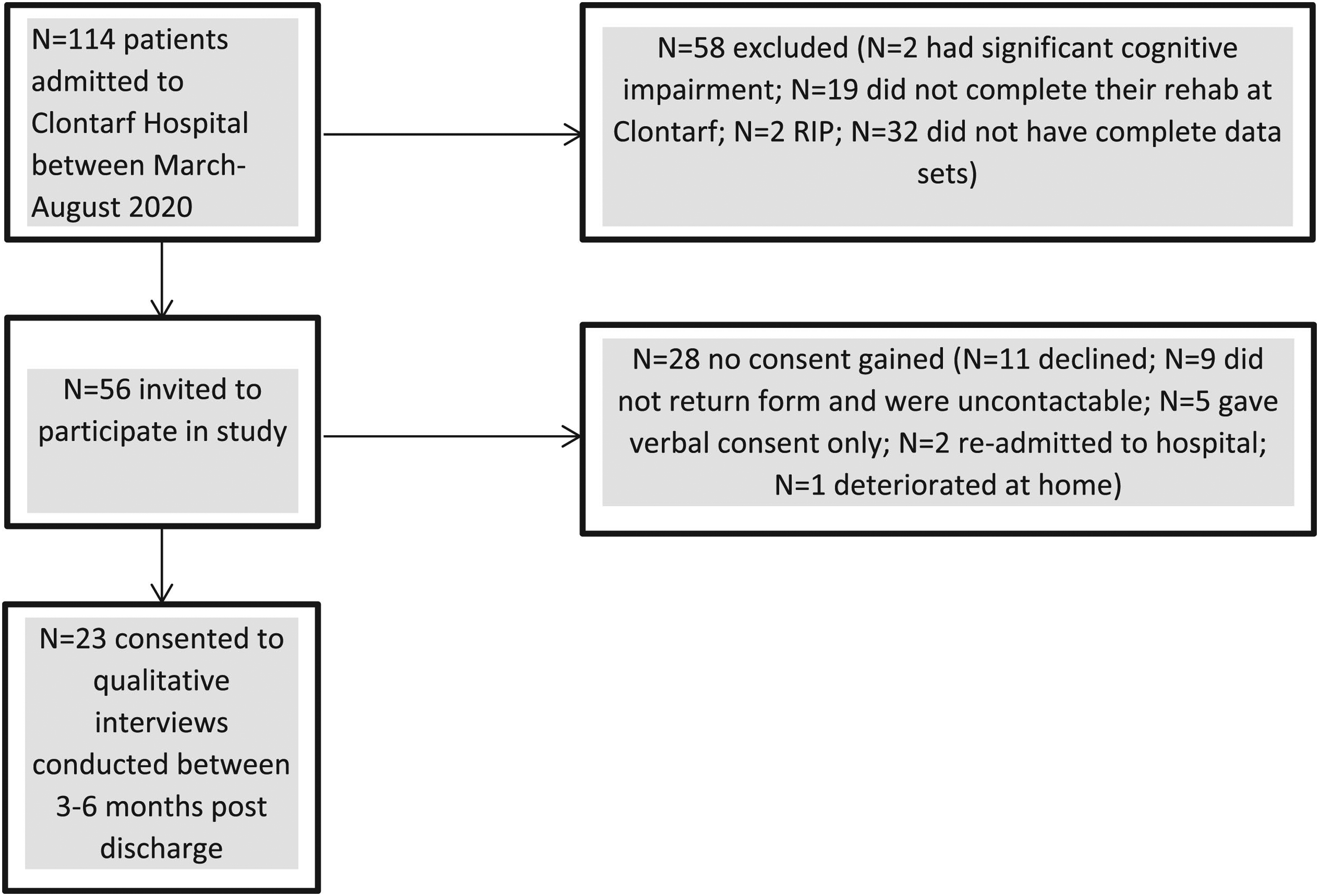
Participant flow diagram.
Four key themes were identified from the analysis of the semi-structured interviews: (1) Acute Period of Symptoms after COVID-19 diagnosis, (2) Sub acute rehabilitation experience, (3) Life after hospitalisation and (4) Long Covid symptoms. There were a number of subthemes within each of these themes.
3.2. Theme 1 – Experience during the Acute Period after COVID-19 diagnosis
Theme 1 explored the experience of participants during the acute period after a diagnosis. Two subthemes were identified under this theme including: (i) Symptoms experienced during the acute period of a COVID-19 infection and (ii) Post ICU syndrome
3.2.1. Symptoms experienced during the acute period of a COVID-19 infection
The symptoms experienced by the participants in the current study differed between those who had become critically ill and those who did not require invasive support. Those who became critically ill experienced a myriad of symptoms as compared to those who did not require invasive support, these participants reported having “no side effects from it whatsoever”, (F63; Non Critical-Care) and some “didn’t know,” (F80; Non Critical-Care) they had it. To demonstrate the diversity in symptoms experienced by these two groups, the symptoms reported by patients in interviews were quantitatively synthesised (Table 5).
3.2.2. Post ICU syndrome
Post ICU syndrome is a term that describes the cognitive, psychological, physical and other consequences that persist beyond discharge from the acute setting [17, 18]. Physical impairments as reported by the following patient were typical: “I couldn’t move in the bed, I couldn’t move my limbs, I couldn’t stand, I couldn’t walk...I had to obviously have a hoist” (M75; Critical-Care). One participant attributed the psychiatric consequences such as “PTSD,” to “someone dying beside me“(M53; Critical-Care). Fear surrounding survival seemed particularly emotive for some participants who became critically unwell as stated by the one participant: “the emotional thing was that I didn’t know whether I was going to make it or not”, (M70; Critical-Care).
3.3. Theme 2 - Post acute rehabilitation experience
Theme 2 explored the participants’ experience of the sub-acute rehabilitation services. The subthemes identified under this theme included: (i) The overall rehabilitation experience and (ii) The role of the physiotherapist.
3.3.1. Overall rehabilitation experience
Transfer to off-side rehabilitation from the acute hospital setting was perceived as very positive by most participants as they could “see the light,” and that they were “improving and getting better.” (M75; Critical-Care). However, some participants voiced a degree of frustration during their rehabilitation: “I didn’t realise that I need so much time to recover” (M62; Critical-Care). One participant even stated: “the hardest part in there was that I felt good enough that I should have been out of there” (M70; Critical-Care). Rehabilitation during the COVID-19 pandemic was additionally challenging for participants, as there was a range of restrictive measures in place including, patients not being allowed have visitors which resulted in participants reporting feeling “lonely”, or “a bit down” (M38; Critical-Care). Even those who did not experience a critical illness felt “depressed at times” (F90; Non Critical-Care). Some, patients reported the situation as “very distressing” (M70; Critical-Care). More concerning was that one individual reported feelings of stigmatisation as he observed “people cleaning up immediately” after he sat somewhere or “people trying to avoid” him (M53; Critical-Care). Despite these additional challenges to their rehabilitation experience participants in the current study developed coping mechanisms to over these for example using technology, for example “Facetime,” (F69; Non Critical-Care) to connect with family or friends was a common strategy. Some others reported that they were “dealing with it spiritually” (M38; Critical-Care).
3.3.2. The role of the physiotherapist
Physiotherapists play a primary role in physical rehabilitation [19] and participants in the current study received almost daily physiotherapy input. Participants reported the physiotherapists, “were great for encouraging you,” (F69; Non Critical-Care) and were described as “amazing people,” (M; 70; Critical-Care). However due to the visiting restrictions the physiotherapists treating participants in the current study were also an important social support, one participant reported “people don’t realize how, when you interact with your physio, how that has such a good effect on you mentally because they make you kind of believe in yourself” (F59; Critical-Care). The rehabilitation experience was also challenged by the use of PPE however interestingly participants reported that “it didn’t affect the treatment“(M61; Critical-Care) and there was a general “accepting” (M38; Critical-Care) that PPE had to be used “to protect everybody” (M38; Critical-Care). Despite the unique environment the participants in the current study experienced most participants reported they were “enjoying doing” (M; 64; Critical-Care) their rehabilitation some however “didn’t find the treatment really a challenge” (M64; Critical-Care). Given the novel nature of COVID-19 and the reports of persistent fatigue following the infection [20, 21], treating physiotherapists were mindful not to over exert patients during the rehabilitation.
3.4. Theme 3 – Transitioning home after hospitalisation with COVID-19 infection
Theme 3 explored whether patients reported if they felt prepared for discharge home. Two subthemes were identified under this theme: (i) Preparation for transitioning home and (ii) Life at home
3.4.1. Preparation for transitioning home
Most participants were highly engaged in their rehabilitation as they were keen to return home: “I did my exercises because I wanted to get out and get home.” (M75; Critical-Care). Nearly, all participants reported feeling “confident” (M72; Critical-Care) in being able to return home independently. However, one patient reported feeling “unsure” about returning home and expressed concern over “becoming institutionalised” (F85; non Critical-Care).
3.4.2. Life at home
A measure of successful rehabilitation is reintegration back into previous societal roles [22, 23]. Successful discharge from a social perspective was more difficult to ascertain as at the time of data collection as there were national restrictions in place, people were “limited socially” (M64; Critical-Care) and were unable to engage in normal social activities “like meeting the lads over in the pub for a few drinks or whatever.” (M64; Critical-Care). Others chose to restrict and or alter their social interactions and activities regardless of governmental restrictions: “I get the shopping delivered now I don’t go out and do my own shopping anymore.” (M56; Critical-Care). A small number of patients were still working in the time preceding their COVID-19 infection. One self-employed individual reported that they were “back working 15 weeks now” (M70; Critical-Care), having returned to work shortly after discharge. Seven other patients reporting that they had “not yet.” (M38; Critical-Care) been able to return to work.
3.5. Theme 4. Long Covid syndrome
Long Covid is a term being used to describe the persistence of one or more of the symptoms associated with a COVID-19 infection [24, 25]. Three subthemes were identified under this theme: (i) the psychological and emotional consequences, (ii) the physical consequences and (iii) follow up and self-management.
3.5.1. Emotional and psychological consequences
The majority of individuals who reported emotional consequences described negative sequelae to having had COVID-19 infection. Some described emotional and psychological responses to their experience in hospital, such as “flashbacks” (F59; Critical-Care), low mood: “recounting the experience ... brings me down” (M53; Critical-Care) and loss of enthusiasm: “I don’t think I’ll ever feel the same zest for life that I had.” (F59; Critical-Care). Participants reported feelings of sadness and nostalgia about “the life” they before their COVID-19 infection (F63; Non Critical-Care).
3.5.2. Physical consequences
Although the quantitative results of this study indicated an improvement in all of the outcome measures from admission to discharge, there have been broad descriptions of physical consequences with ”post COVID fatigue” (F59; Critical-Care) being the most frequently reported. While all patients were discharged home, many reported that they hadn’t “quite recovered” (M72; Critical-Care) and were “nowhere near” (M75; Critical-Care) where they were before being hospitalised with COVID-19. Two individuals who were younger than the average age of participants and had experienced a critical illness relating to COVID-19 described the unpredictability of their physical functioning: “Strength wise, some days I feel so strong, no shortness of breath and some days is like, I just feel deflated.” (M53; Critical-Care), “If I walk today for a few kilometres then the next day I feel tired” (M38; Critical-Care).
3.5.3. Follow up and self-management
Given the novel nature of COVID-19 at the time of data collection there was no defined pathway of care for those recovering from a COVID-19 infection. Some patients reported that they were “back in the COVID clinic” (F59; Critical-Care) or that they had “been attending the hospital,” to be “monitored” (M56; Critical-Care). Many individuals reported being followed up with “physio .... in the primary care centre” (F59; Critical-Care) or with a public health “nurse” (M62, Critical-Care) after discharging home. This was not the uniform experience with one patient reporting “no physio whatsoever” (F63, Non Critical-Care) since discharge from post-acute rehabilitation. As part of their self-management of the condition number of participants reported continuing to do their “exercises” (M56; Critical-Care), “every day of the week” (M64; Critical-Care), and now consider it “part of life.” (M64; Critical-Care).
4. Discussion
This study met its aim to explore the patient experience of rehabilitation following a COVID-19 infection during the first wave of the pandemic. The results of this study shed light on the loneliness and stigmatisation that patients felt during this time, it also highlights the importance of the patient-physiotherapist relationship as physiotherapists became the patients’ social support.
Participants in the current study described a sense of loneliness and stigmatisation during their inpatient stay. Since the conduct of this study there has been a programme of research exploring loneliness and social isolation during the COVID-19 pandemic. Sayin Kasar and Karam (2021) conducted a scoping review to evaluate the social isolation, loneliness and quality of life of elderly individuals during the COVID-19 pandemic and to map suggestions to reveal and improve the current situation [9]. Seven studies were included in this review and the authors provide recommendations for overcoming loneliness which include the use of technology and providing support by means of the individual’s religious practice. Participants in the current study reported using these practices for example the use of facetime to contact family members while others dealt with the loneliness spiritually. However the use of video calls to reduce loneliness is currently unsupported in the literature [10], future research should explore the use of video calls with additional strategies tailored to individual needs to overcome loneliness. COVID-19 stigmatisation became widespread particularly during the first wave of the pandemic due to the spreading of misinformation and fear [11]. A study found that more than 50% of the respondents were afraid from COVID-19 and 64% had stigma towards infected people and their contact during the COVID-19 pandemic [12]. Stigmatisation can have a profound negative effect on an individual, including increased risk of anxiety and depression [13]. While it was likely not the intention for any individual to feel stigmatised in a healthcare setting, future research should focus on developing policy and procedure to ensure that no patient should feel stigmatised while receiving treatment.
Given the visiting restrictions that were imposed in healthcare settings during the COVID-19 pandemic, participants in the current study described how their physiotherapist became part of their social support network. While there seems to be limited research specifically on the evolution of the patient-physiotherapist relationship during COVID-19. Elsewhere patients have reported the positive impact of physiotherapy intervention during the COVID-19 pandemic in combatting social isolation [14]. However, the psychological burden of this added emotional support to patients on staff delivering care during the COVID-19 pandemic has been widely reported in the literature [15, 16]. Jacome et al. 2021 reported that more than 40% of physiotherapists experienced personal and work-related burnout and 25% patient-related burnout, with resilience, depression and stress having a relevant role in the three burnout dimensions [17]. Future research should explore the long term of impact of working during the COVID-19 pandemic on physiotherapists, how their roles evolved during this time and how learnings from this can help inform the response to future pandemics.
Long COVID (sometimes referred to as ‘post-acute sequelae of COVID-19’) is a multisystemic condition comprising often severe symptoms that follow a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection [18]. The incidence of long-COVID in those who have been hospitalised is estimated to be 50–70% [18]. In Ireland there is estimated to be 336, 451 individuals experiencing or have experienced medical issues associated with long-COVID [19]. It is therefore unsurprising that participants in the current study reported feelings of fatigue, breathlessness and reduced physical function, which are documented in the literature as symptoms of long-COVID. This data was collected between three to six months post infection of COVID-19. Given the relatively novel nature of long-COVID the trajectory of recovery is not fully understood, the prevalence of some symptoms have increased over time, while other have subsided within a year and others are still present at two years following an infection. More longitudinal studies exploring the experience of people living with long-COVID are required to fully understand and treat this condition.
4.1. Strengths and limitations
This study adds to the research of the lived experience of individuals who had a COVID-19 infection. It highlights some important areas for future research specifically relating to interventions to combat loneliness and stigmatisation and how the role of physiotherapists evolved to provide additional social support to inpatients during the COVID-19 pandemic. The data was collected three to six months following discharge from the rehabilitation facility, therefore participants recall may have been affected. Additionally this three month time frame may have resulted in a varied experience for participants.
5. Conclusion
The lived experience of COVID-19 from the acute stages, through rehabilitation and transitioning home and into society varied hugely between individuals at all stages, which should be reflected in our management of this patients. Some participants expressed feeling lonely and stigmatised during their rehabilitation, which is avoidable and should be considered in future pandemics and healthcare delivery. The role of physiotherapists during rehabilitation grew from providing physical rehabilitation to being a central part of the patients social support network. This research provides important learnings for healthcare delivery and training of healthcare providers.