
Abstract
Background
Patellofemoral arthritis is a common condition causing knee pain and functional limitations. The Mikhled Knee Exercise Program (MKEP) is an emerging approach for managing this condition, but its efficacy needs further evaluation.
Objective
To assess the comparative effectiveness of MKEP combined with ultrasound therapy and conventional physiotherapy combined with ultrasound therapy in managing patellofemoral arthritis.
Methods
Thirty participants diagnosed with patellofemoral arthritis were randomly assigned to two groups: MKEP group (n = 15) and conventional therapy group (n = 15). The MKEP group received the Mikhled knee exercise program along with ultrasound therapy, while the conventional group received traditional physiotherapy exercises and ultrasound therapy. Both groups underwent a 6-week intervention. Pain levels were assessed using the Numerical Pain Rating Scale (NPRS), and functional status was evaluated using the Anterior Knee Pain Scale (AKPS) at baseline and after the intervention.
Result
Both groups showed significant improvements in NPRS and AKPS scores after the intervention (p < 0.0001). However, the MKEP group exhibited substantially greater improvements in NPRS (mean post-test score: 3.93 vs. 4.87) and AKPS (mean post-test score: 76.14 vs. 65.93) compared to the conventional group (p < 0.0001).
Conclusion
The findings suggest that the Mikhled Knee Exercise Program combined with ultrasound therapy is more effective than conventional physiotherapy with ultrasound in reducing pain and improving functional status among patients with patellofemoral arthritis.
1. Introduction
Patellofemoral arthritis is a prevalent degenerative condition o of knee. Over the age of 55, 24% of females and 11% of males have patella femoral osteoarthritis, which is a rather prevalent condition [1–4]. Isolated patellofemoral osteoarthritis (PFOA) is a common subtype of knee osteoarthritis, with a high prevalence across different age groups and populations. The patellofemoral joint (PFJ) and quadriceps muscle work closely together during activities like walking. For individuals suffering from patellofemoral joint osteoarthritis (PFJ OA) or patellofemoral pain, they may unconsciously alter their gait pattern as a compensatory mechanism to reduce forces transmitted through the affected joint and alleviate discomfort. Specifically, these patients may rely more heavily on hip muscle forces and the lower portions of the quadriceps rather than engaging the full quadriceps contraction during the stance phase of gait. By shifting load away from the patellofemoral joint, this gait adaptation could provide some relief from pain experienced with forceful quadriceps contractions. However, research has not definitively determined if people with PFJ OA consistently demonstrate greater utilization of hip and distal quadriceps forces compared to healthy individuals during walking [5–7]. The stability of the patellofemoral joint relies significantly on the vastus medialis muscle (VMM), specifically the dynamic medial soft tissue stabilizer known as the vastus medialis obliquus (VMO). The VMO, situated in the distal part of the vastus medialis muscle with fibres inserting at a 50° angle into the longitudinal patellar alignment, plays a crucial role.
The Mikhled Knee Exercise Program (MKEP) is a novel therapeutic approach that incorporates isometric and dynamic exercises targeting the agonist and antagonist muscles surrounding the knee joint [9]. MKEP aims to improve joint range of motion, strength, and overall health status while reducing pain in individuals with knee osteoarthritis [10].
The MKEP is a therapeutic exercise approach that utilizes a series of deliberate, gentle movements and positions aimed at facilitating optimal muscle contraction and avoiding potentially detrimental postures. The exercises involve actively engaging and contracting specific muscle groups, while placing the body in aligned postures that counteract excessive internal or external rotation. Central to the MKEP is the concept of progressing through seven distinct therapeutic levels or positions. The first level consists of exercises performed in a supine (lying on back) position. The second level builds upon the first, performed while propped up on the elbows in a supine position. The third level transitions to a half-sitting posture, followed by the fourth level which is conducted in a prone (lying on stomach) position. The fifth level takes place in a long sitting stance on a bench. The sixth level is performed in a prone position on a bench, and the seventh level returns to a supine position but on a bench. Each progressive level challenges the neuromuscular system in a slightly different way, aiming to enhance muscle contraction capabilities while maintaining proper joint alignment and muscular balance. Importantly, the MKEP requires active participation from the patient, as they must consciously contract and control muscles through each position. The various positions and exercises within this therapeutic system are intended to improve strength, flexibility, and neuromuscular control without placing excessive strain on the joints or reinforcing detrimental movement patterns [11].
While MKEP has shown promising results in preliminary studies, a comprehensive evaluation of its efficacy compared to conventional physiotherapy is warranted. This study aimed to assess the comparative effectiveness of MKEP combined with ultrasound therapy and conventional physiotherapy combined with ultrasound therapy in the management of patellofemoral arthritis.
2. Methods
This comparative study involved 30 participants diagnosed with patellofemoral arthritis through clinical evaluation and imaging studies (MRI). Participants who met the inclusion criteria were recruited through convenient sampling from Saveetha medical college and hospital and randomly allocated to two groups: the MKEP group (n = 15) and the conventional therapy group (n = 15).Inclusion criteria were (i) age >40 years, (ii) presence of anterior knee pain,(iii) stiffness (iv) crepitus, (v) swelling, (vi) functional impairment in activities such as squatting, climbing stairs, and walking, (vii) Q-angle >20 degrees, (viii) positive patellar grind test. Exclusion criteria included (i) the presence of other significant knee pathologies, (ii) history of knee surgery within the past six months, (iii) severe obesity, (iv) cognitive impairment, participation in another clinical trial, (v) history of substance abuse or psychiatric disorders, (vi) severe comorbidities that could affect the intervention or outcomes.The MKEP group received the Mikhled knee exercise program three times a week for six weeks, along with ultrasound therapy. The program consists of 7 level postures and has 5 exercises in each posture. This study focuses on three main levels. The program consisted of 15 different exercises targeting the knees and associated leg muscles. Participants performed the routine 3 times per week for 6 weeks. Each exercise involved a 10 second hold followed by a 30 second rest period before moving to the next exercise. The exercises were divided into three main positions - supine (lying on back), long sitting (seated with legs extended), and prone (lying on stomach). In the supine position, exercises included: Ankle dorsiflexion - Pulling toes up towards shins to stretch calf muscles, Knee straightening - Lifting one straight leg by tightening quadriceps, Straight leg raises - Lifting one straight leg up towards ceiling, Leg abduction - Lifting one straight leg out to the side, Heel slides - Bending knee to bring heel towards buttock
In long sitting, the same ankle, knee, leg raising, and abduction movements were performed while seated upright with legs out in front. For the prone position, participants did: Ankle dorsiflexion by pulling toes up, Knee straightening by tightening quads to raise leg, Straight leg raises by squeezing hamstrings and glutes, Leg abduction by lifting leg laterally from hips, Heel slides by bending knee to bring heel in. Emphasis was placed on proper form, controlled motions, breathing normally, and progressing at one’s own ability level. The varied positions and exercises aimed to improve knee strength, flexibility, and overall range of motion.
The conventional therapy group underwent traditional physiotherapy exercises three times a week for six weeks, along with ultrasound therapy. The exercise program consisted of 9 different exercises targeting the lower body muscles. Participants performed the routine 3 times per week for a set duration (exact duration not specified). Each exercise involved a 15 second hold followed by a 15 second rest period before moving to the next exercise in the sequence. The exercises were as follows:
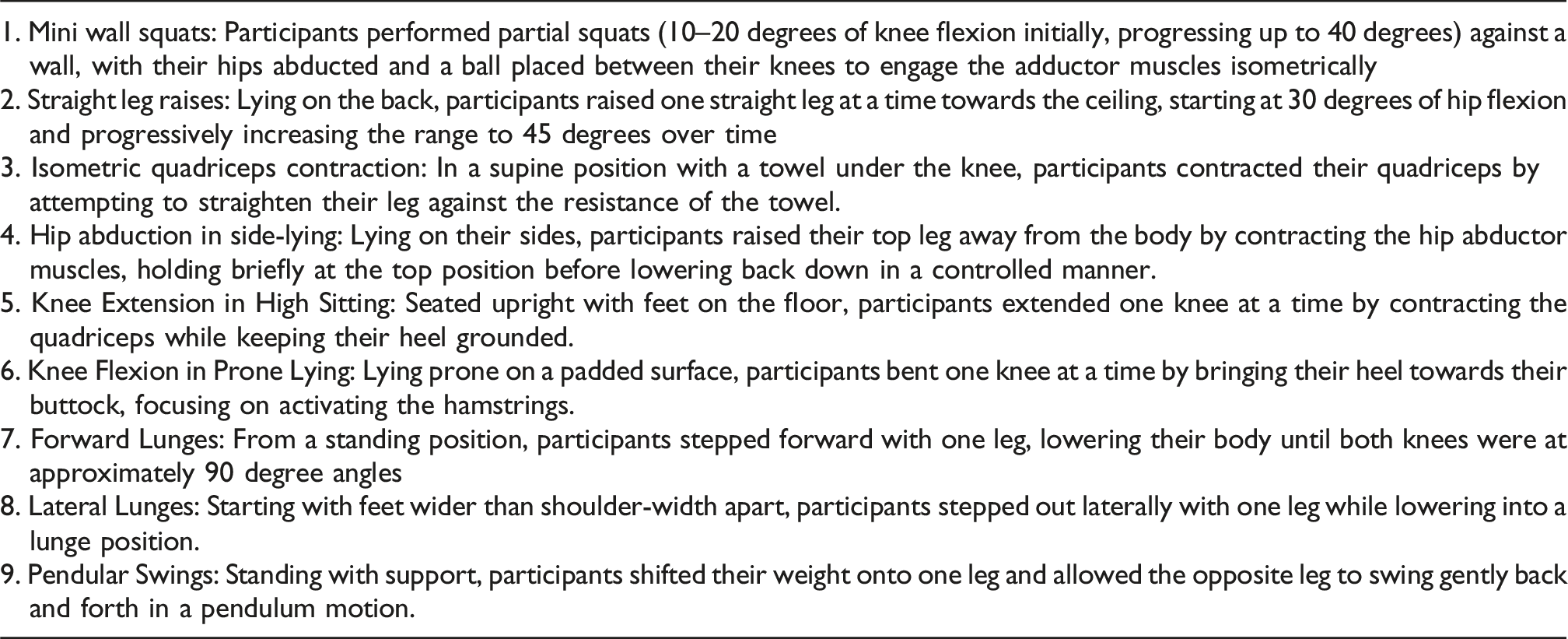
Emphasis was placed on maintaining proper form, using controlled movements, avoiding excessive strain or compensation, and progressively increasing range of motion and intensity as appropriate for each individual. This well-rounded program aimed to improve lower extremity strength, flexibility, balance and overall function.
Both groups received ultrasound therapy for 6 minutes at 1.2 watts/cm2 at a frequency of 1 MHz on all present trigger points in quadriceps(VMO), twice a week for four weeks. Pain levels were assessed using the Numerical Pain Rating Scale (NPRS), and functional status was evaluated using the Anterior Knee Pain Scale (AKPS) at baseline and after the 6-week intervention. Paired t-tests and unpaired t-tests were used for statistical analysis. A p-value <0.05 was considered statistically significant.
3. Results
Both groups showed significant improvements in NPRS and AKPS scores after the intervention (p < 0.0001).
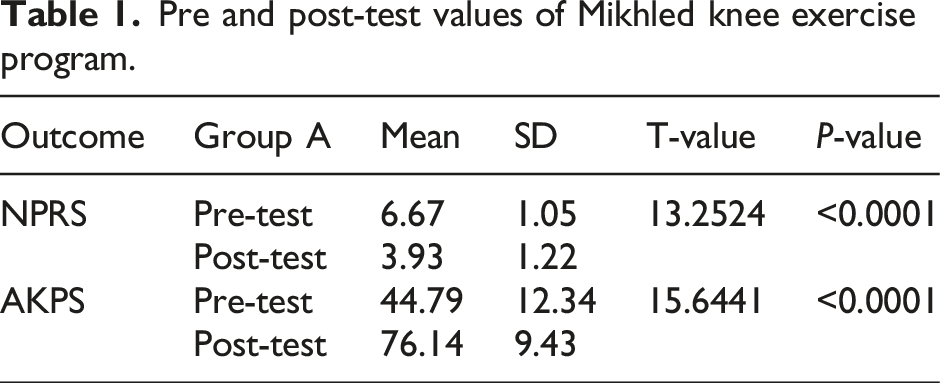
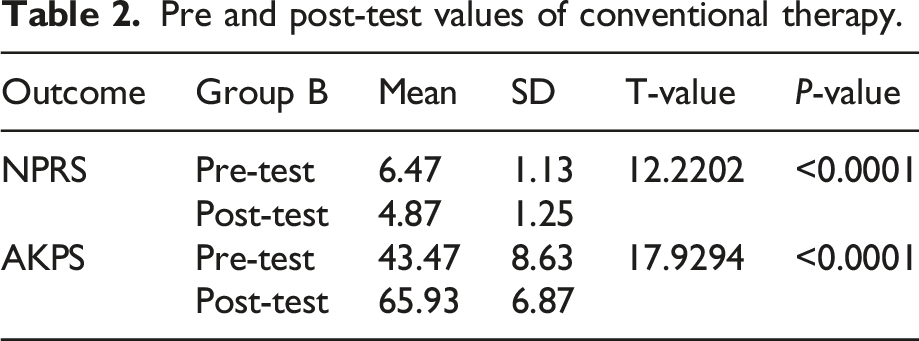
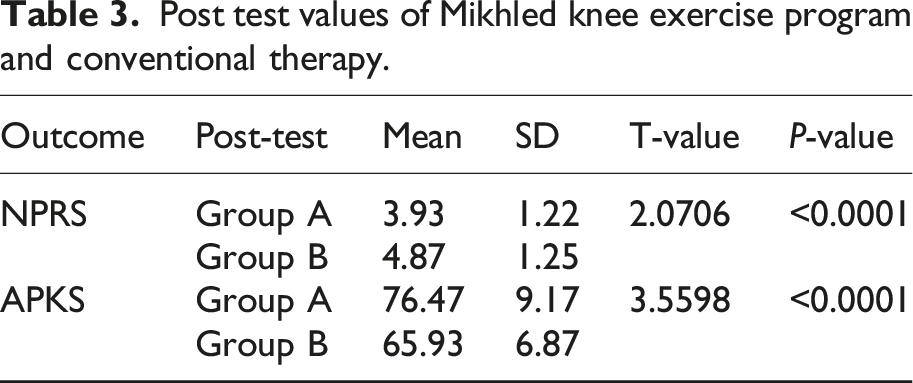
In the MKEP group, the mean NPRS score improved from 6.67 (pre-test) to 3.93 (post-test), and the mean AKPS score improved from 44.79 (pre-test) to 76.14 (post-test)’as shown in Table 1’. In the conventional therapy group, the mean NPRS score improved from 6.47 (pre-test) to 4.87 (post-test)’as shown in Table 2’, and the mean AKPS score improved from 43.47 (pre-test) to 65.93 (post-test)’as shown in Table 3’. When comparing the post-test values, the MKEP group showed significantly better improvements in NPRS (mean post-test score: 3.93 vs. 4.87, p < 0.0001) and AKPS (mean post-test score: 76.14 vs. 65.93, p < 0.0001) compared to the conventional therapy group. Confidence interval of 95% for all values.
Pre and post-test values of Mikhled knee exercise program.
Pre and post-test values of conventional therapy.
Post test values of Mikhled knee exercise program and conventional therapy.
4. Discussion
The findings of this study demonstrate the effectiveness of both the Mikhled Knee Exercise Program (MKEP) and conventional physiotherapy in improving pain and functional status among patients with patellofemoral arthritis [12–14]. However, the MKEP group exhibited substantially greater improvements compared to the conventional therapy group, suggesting the potential superiority of MKEP combined with ultrasound therapy in managing this condition [15].
MKEP is a unique exercise program that incorporates both dynamic and isometric exercises, targeting the agonist and antagonist muscles surrounding the knee joint [16]. This approach is designed to address the biomechanical deficiencies associated with patellofemoral arthritis, such as quadriceps weakness, vastus medialis obliquus (VMO) dysfunction, and imbalances in hip muscle strength [17–19].
The isometric component of MKEP allows for targeted strengthening at specific joint angles, which is particularly beneficial for patellofemoral arthritis [20]. Isometric exercises have been shown to effectively increase muscle strength at the targeted joint angles and, to a lesser extent, at other joint angles [21]. This targeted approach can enhance joint stability and improve function in individuals with patellofemoral arthritis [22].
Additionally, MKEP incorporates dynamic exercises that promote strength development throughout the entire range of motion [23]. This combination of isometric and dynamic exercises provides a comprehensive approach to rehabilitation, addressing both localized and global muscle strengthening needs [24].
The convenience of MKEP is also noteworthy, as it does not require specialized equipment, making it accessible for patients to continue their exercises at home, potentially improving adherence and long-term outcomes [25].
While conventional physiotherapy exercises also showed improvements in pain and function, the superiority of MKEP combined with ultrasound therapy suggests a synergistic effect between targeted exercises and the therapeutic benefits of ultrasound, Ebenbichler et al concluded that 24 daily applications of ultrasound therapy at 2.5 W/cm2 (5 times per week for 3 weeks and then 3 times per week for 3 weeks) reduced the painful symptoms in patients with calcific tendinitis of the supraspinatus tendon [26]. Ultrasound therapy has been shown to alleviate pain, reduce inflammation, and promote tissue healing, which may have contributed to the enhanced outcomes in the MKEP group. Crossley et al, stated that there is no significant effect on quadriceps group by physical therapy on a time period of 6 weeks, when isometric exercises are performed at the extremes of joint range of motion, flexibility may increase. In certain dynamic activities, muscle fibres that are frequently overlooked are recruited by these isometric contractions. It may be more convenient for them to continue performing the exercises at home alone because MKEP does not require any equipment [27–29]. It is important to note that this study evaluated the effects of MKEP and conventional physiotherapy in combination with ultrasound therapy. Future research could explore the individual contributions of each component and investigate the optimal dosage and frequency of MKEP exercises for maximum therapeutic benefit. According to Brosseau et al., ultrasound therapy did not have a clinically significant impact on PFPS patients’ pain alleviation. The low methodological quality of the included trial and the inadequate reporting of the therapeutic use of ultrasonography limit the validity of these conclusions. Regarding the application or nonapplication of ultrasound therapy for the treatment of PFPS, no conclusions can be made. There must be more carefully planned research. Conversely, the current study showed that both PFPS groups’ pain and impairment had significantly improved [30].
5. Conclusion
The findings of this study suggest that the Mikhled Knee Exercise Program (MKEP) combined with ultrasound therapy is more effective than conventional physiotherapy with ultrasound in reducing pain and improving functional status among patients with patellofemoral arthritis. MKEP’s unique approach, incorporating both isometric and dynamic exercises, targets the specific biomechanical deficiencies associated with this condition, leading to superior outcomes compared to traditional exercise programs.
Further research is warranted to explore the long-term effects of MKEP, optimize exercise prescriptions, and investigate the potential synergistic effects of MKEP with other therapeutic modalities. Nonetheless, this study provides valuable insights into the efficacy of MKEP as a promising therapeutic option for the management of patellofemoral arthritis.
5.1. Limitations
Lack of continued follow-up of participants. The sample size was relatively small, and the study duration was limited to three weeks. The research employed convenience sampling, potentially introducing selection bias and restricting the generalizability of the sample. The study had a relatively short intervention duration of three weeks, which may not be sufficient to fully evaluate the effects of the interventions. The study did not collect proper follow-up data, which may limit the ability to assess the long-term effects of the interventions.
Footnotes
Acknowledgments
The authors have no acknowledgement.
Conflict of interest
The authors declare no conflicts of interest.
Ethics approval
This study was approved by the Institutional Scientific Review Board (03/015/2023/ISRB/SR/SCPT), and all participants provided written informed consent.