
Abstract
BACKGROUND:
High pressure in diabetic foot plantar areas causes ulcer formation, leading to disability and amputations. Around 25% of diabetics experience foot ulcers, with prevalence rates varying among Africans, Asians, and Europeans. Egypt has the highest rates, ranging from 6.1% to 29.3%.
OBJECTIVE:
To investigate the impact of functional ankle taping correction on plantar foot ulcer healing in diabetic patients.
METHODS:
A double-blinded randomized controlled trial design. A total of 70 patients with plantar foot ulcers PFUs were randomly divided into two groups: group A, which received ankle taping in addition to usual medical therapy and debridement, and group B, which received ankle taping without routine medical treatment and debridement. Over two months, all patients underwent evaluation using a Walkway pressure monitoring system, goniometer, wound workstation, and saline injection. This evaluation aimed to determine maximal peak plantar pressure, active ankle dorsiflexion, wound area, and volume sequentially.
RESULTS:
Initially, there was no meaningful difference between the two groups. However, after eight weeks of treatment, there was a substantial impact, as indicated by a p-value of 0.001 and an f-value of 87.49 for treatment effect at 95% CI.Furthermore, a statistically significant interaction was found between treatment and time in the ankle-taping group between pre-and post-treatment. However, no difference was identified in the control group.
CONCLUSIONS:
The correction of ankle taping has a significant impact on various factors, including peak plantar pressure, ankle dorsiflexion, wound area, and wound volume. This correction leads to a reduction in peak plantar pressure, wound area, and volume while also enhancing active ankle dorsiflexion.
Keywords
Introduction
Diabetic foot ulcers (DFUs) are a significant and destructive consequence of diabetes, impacting approximately 26 million individuals globally each year. Individuals with diabetes have a lifetime risk of around 25% of acquiring a foot ulcer, which is significantly higher than those without diabetes [1]. The prevalence of foot ulcers in the diabetic community has been found to range from 4% to 10%. Around half of diabetic foot ulcers (DFUs) develop on the plantar surface of the foot. If not treated properly, these ulcers can become chronic and fail to heal [2]. Diabetic foot ulcers (DFUs) are a well-known condition that increases the likelihood of negative health outcomes, such as major limb amputation. Additionally, DFUs impose a costly burden on the healthcare system due to prolonged healing durations, diminished quality of life, and an elevated death rate [3].
Increased plantar pressure while walking is another indicator of diabetic foot ulceration. Nevertheless, research on the sensitivity and specificity of barefoot plantar pressure in predicting ulceration indicates that while barefoot pressure is significant, it is only a somewhat accurate predictor [4]. This is likely because patients walk barefoot in their daily lives and wear shoes, which create different biomechanical conditions. When walking without shoes, the pressure on the bottom of the foot is usually significantly greater than when wearing protective footwear that patients commonly receive after a plantar foot ulcer has healed [5]. Therefore, persistently wearing such footwear directly impacts the overall mechanical stress on the foot and can significantly influence the chance of ulcer recurrence [6]. Kinesio taping (KT) is a method that involves using conventional taping techniques to imitate the characteristics of human skin. The tape is very thin, similar to the epidermis, and may be stretched longitudinally by 30% to 40% of its original length [7]. Kinesio taping (KT) is an active method that does not immobilize but enhances proprioception to support the musculoskeletal system actively. This can be beneficial for improving posture and movement, even in individuals without symptoms, by optimizing muscle function and correcting misaligned joints [8].
This study aimed to examine the impact of correcting functional ankle taping on healing plantar foot ulcers (PFUs) in diabetic patients.
Methods
The study is a controlled, double-blinded, and randomized controlled trial that occurred between August 2023 and February 2024 at the outpatient clinic of the Modern University for Technology and Information Faculty of Physical Therapy. The Ethical Committee for Human Research endorsed the study in line with the principles of the 1975 Declaration of Helsinki at the Cairo University’s Faculty of Physical Therapy in Egypt (Reference number: P.T.REC/012/004688) and was registered with the Clinical Trials.gov (NCT06065488).
Participants
Patients (male and female) with PFUs who were referred for physical therapy by a vascular surgeon were recruited from Om El Masryeen General Hospital and El Rahma - a private clinic. Informed consent was obtained from the participants before the study. To participate in the study, participants had to be between 42 and 60 years old, have a single active unilateral PFU of at least 1 cm2 (greatest length x greatest width), not healed for > 3 months duration, and have the ability to walk independently. Several exclusion criteria were used, such as the absence of ankle pathology or surgery, the lack of protective sensation on the plantar foot as determined by a 10-gram monofilament based on the criteria established by the International Working Group on the Diabetic Foot in 2023, recent participation in another clinical trial, uncontrolled diabetes, insufficient blood circulation, skin allergies, foot deformities, and amputations.
Participant characteristics
All participants were measured by their body mass index (BMI), age, height, glycated hemoglobin A1c (HbA1c), monofilament sensation, and ankle-brachial pressure index at baseline and after eight weeks. All participants received standard care between follow-up visits outside of their involvement in the study. This typically involved assessing and treating their foot ulcer by a podiatrist at least once every week. Evaluation of infection, wound debridement, dressing of the ulcer, and diabetes management in consultation with an endocrinologist or general practitioner.
Sample size determination
The sample size was determined using data on plantar peak pressure obtained from a pilot study including 5 participants in each group. The calculation was conducted using the G*POWER statistical software (version 3.1.9.2; Franz Faul, Universitat Kiel, Germany) and determined that a sample size of N = 70 was necessary for this investigation. The calculation used an alpha value of 0.05, a beta value of 0.2, and an effect size of 0.42.
Allocation concealment and randomization
A computer-generated table of random numbers allocated patients to various therapy groups. Patients were assigned to one of two groups using a random allocation approach. Group A was administered functional ankle taping, medical care, and dressing based on their conditions. Group B received a placebo-taping approach that was regarded as useless. The taping did not involve the insertion to the origin of the muscles and was done using the same material without applying any strain.
Additionally, the participants in Group B also received medical care and dressing based on their circumstances. The allocation process was obscured through the use of sealed, opaque envelopes. Additionally, a qualified physical therapist, who had no involvement in the study protocols, was responsible for generating the randomization to guarantee an impartial assignment. This paraphrase rectifies the sentence structures and elucidates that the allocation of treatment groups was done randomly.
Outcome measure
Primary outcome measure
2.4.1.1. Plantar peak pressures by Walkway pressure system The Tekscan® pressure mat system, located in Boston, MA, was used to measure the maximum plantar peak pressures. These measurements were conducted utilizing the mat-based Stride Way System, which had dimensions of 150 cm in length and 60 cm in width. Patients were provided with an opportunity to acquaint themselves with the protocol. The mat was calibrated before testing. After the calibration, the patient was instructed to walk across the plantar pressure mat in the middle of the walkway. The procedure was verified, and each participant was required to do two steps before landing on the pressure pad. Trials were excluded and repeated if participants intentionally adjusted their walking style to ensure they made complete contact with the mat. To prevent this, a Tegaderm treatment (Wound Dressings designed to manage different level of exudate and protect surrounding skin from maceration) (did not interfere with measuring the pressure on the sole. Every trial was measured for its duration, and if it deviated by more than 5% from the duration of the first recorded trial, it was excluded. In such cases, the subject had to repeat the trial. Only the intermediate three steps of each trial were examined to mitigate the impact of acceleration and deceleration. Only plantar ulcerated feet [9] were included in the data collection.
Secondary outcome measure
2.4.2.1. Active ankle dorsiflexion range of motion The maximum dorsiflexion angle at the ankle joint was assessed using a handheld standard goniometer while standing, with the knee fully extended and the heel in touch with the ground. Participants were instructed to incline their bodies forward by moving their knees toward the wall. During the experiment, the subject kept their foot fully flexed. A goniometer, a measuring tool, was placed on the floor and aligned with the fibula bone. The position of the goniometer was determined by visually dividing the lateral malleolus and the fibular head. Each participant was allowed to complete three practice trials [10].
Wound surface area by + Wound Desk mobile application
Mobile application-based system that can be synchronized with a web-based administration that depending on the selected subscription model. Signing into the account was mandatory. A patient’s profile was filled out, specifying the site and mechanism of the trauma. The application was switched to a new photo mode, activating the camera feature on the mobile application. A wound depth indicator should be positioned adjacent to the examined wound. The region of the wound was captured in an image, and the software subsequently identified markers indicating the wound. However, the manual detection of the boundaries of the wound was necessary using a thumb knob thumb. Subsequently, an automated computation of the extent of the wound surface was executed, yielding a value of [11].
Wound volume assessment by saline solution
They utilized sterilized syringes and saline solutions, injecting a 5 cm3 sterile syringe with saline solution. Next, inject the appropriate amount of saline solution into the wound. The approach for wound volume estimation [12] was straightforward and precise.
Treatment procedures
The procedure of the treatment was divided into two main categories.
Therapeutic procedures (preparatory treatment application)
Patient history was taken about the study, and the patient was informed of the treatment and its purpose and placed in a comfortable position; contraindications (mentioned in the exclusion criteria) were excluded.
The procedure of functional ankle tape
The tape applied was elastic. Kinesio tapes, a Sportstex kinesiology therapeutic tape that was not stretched for 5 cm from the initial site, were then stretched to 30% for the remaining parts. The tape used was flexible. The Kinesio tapes, a type of Sportstex kinesiology therapeutic tape, were initially applied without stretching for a distance of 5 cm from the starting point. After that, the tapes were stretched to 30% of their original length for the rest of the application.
A taping was initially put along the entire length of the gastrocnemius muscle, starting from its insertion point and extending to its origin. This was done to reduce muscle activity while the person was lying face down with their knee fully extended. Due to variations in the patient’s ankle placements, the dorsiflexion was manually adjusted, and the tape was applied without causing any pain or discomfort. The second taping was done throughout the whole length of the tibialis anterior muscle, starting from its origin and ending at its insertion, to enhance muscular activity when lying on the back. The third and fourth tapings were used to correct a functional subtalar eversion while the patient was lying down. The tape was perpendicular to the midline of the second and third toes and the midline between the medial and lateral malleoli. The tape was applied from the medial malleolus to the sole, extending approximately 10 cm above the lateral malleolus. During the fourth taping session, the tape was put from the inner ankle bone (medial malleolus) to the outer side of the ankle. The adhesive tape was affixed for five days and detached for one day to facilitate the process of skin sweating. This method was iterated for a total of eight consecutive weeks. The patient was advised to refrain from engaging in strenuous activities for 30 minutes since this is necessary for the adhesive to reach its maximum level of activation.
Statistical analysis
An unpaired t-test was used to compare the subject characteristics between the groups. A Mann– Whitney test was performed to compare the ulcer grades between the groups. The chi-squared test was employed to compare sex distribution between the groups. The normality of the data was assessed using the Shapiro-Wilk test. A Levene’s test was performed to assess the homogeneity of variances between groups. A mixed-design MANOVA was conducted to assess the impact of both within-group and between-group factors on peak plantar pressure, ankle dorsiflexion, ulcer volume, and ulcer area. Post-hoc tests were conducted using the Bonferroni correction to compare several groups. The statistical tests were conducted with a predetermined significance level of p < 0.05. The statistical analysis was performed using the SPSS software package, specifically version 25 for Windows, developed by IBM SPSS in Chicago, IL, USA.
Results
The study investigated the effectiveness of functional ankle taping correction on plantar foot ulcer healing in diabetic patients in a randomized clinical trial. The trial involved 74 participants who were assessed for eligibility, with two excluded for various reasons (One individual does not fit the criterion for participation), while the other individual has chosen not to participate., leaving 72 randomized into two groups, each receiving a different intervention over eight weeks. Group A received functional ankle taping, medical treatment, and dressing according to their cases. Group B received a placebo taping method that was considered ineffective (not from insertion to the origin of muscles) with the same material without tension; they also received medical treatment and dressing according to their cases. After the 8-week intervention period, the participants were assessed for outcome measures, including the walkway pressure system for plantar pressure assessment, a handheld standard goniometer for active ankle dorsiflexion, wound surface area by the+Wound Desk mobile application, and saline solution for wound volume. The randomized procedure was managed by a licensed physical therapist who was not involved in the study’s protocols. Two participants discontinued Group A during the trial due to skin irritation and were referred to a dermatologist for intervention. The analysis of the trial included a total of 35 participants per group who completed the full intervention (Fig. 1).
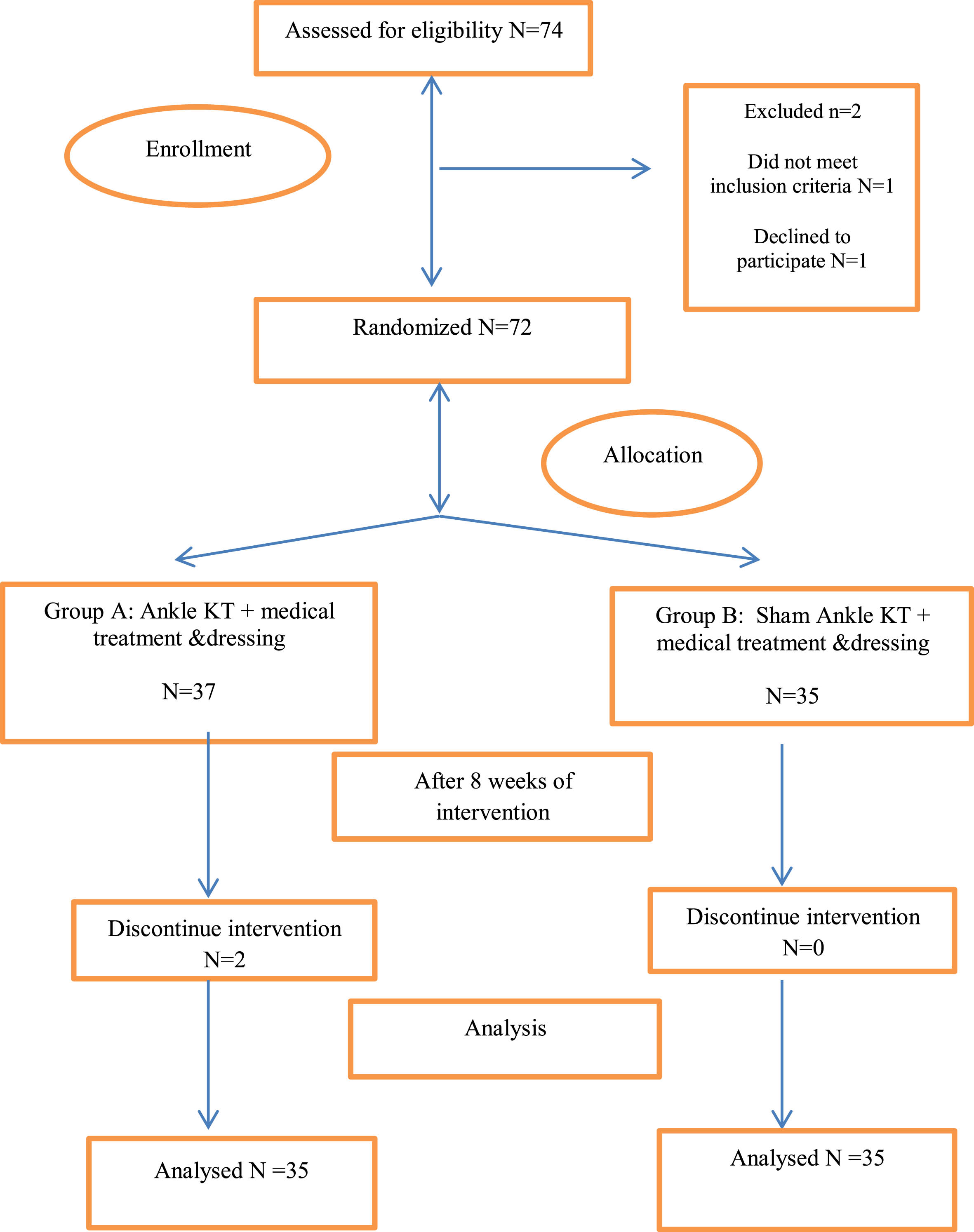
Flow chart diagram.
Table 1 shows the subject characteristics of groups A and B. There was no significant difference between groups in age, weight, height, BMI, duration of diabetes, HbA1c, MNDS, ulcer grade, and sex distribution (p > 0.05).
Basic characteristics of participants
Basic characteristics of participants
SD, standard deviation; MD, mean difference; U: Mann Whitney test; IQR, interquartile range; χ2, Chi squared value; p-value, level of significance.
There was a significant interaction of treatment and time (F = 84.19, p = 0.001, η2 = 0.83). There was a significant main effect of time (F = 690.03, p = 0.001, η2 = 0.97). There was a significant main effect of treatment (F = 87.46, p = 0.001, η2 = 0.84).
Within the group’s comparison
There was a significant decrease in ulcer area, volume, and peak plantar pressure and a significant increase in active dorsi flexion of both groups post-treatment compared with pre-treatment (p < 0.001). (Table 2).
Mean values of ulcer area, volume, ankle dorsi flexion and peak plantar pressure pre and post treatment of group A and B
Mean values of ulcer area, volume, ankle dorsi flexion and peak plantar pressure pre and post treatment of group A and B
SD, Standard deviation; MD, Mean difference; CI, Confidence interval; p-value, Level of significance.
There was no significant difference between groups pre-treatment (p > 0.05). There was a significant decrease in ulcer area, volume, and peak plantar pressure and a significant increase in group A’s active dorsiflexion compared with group B’s (p < 0.001). (Table 2).
Discussion
This study aimed to investigate the effectiveness of functional ankle taping correction on plantar foot ulcer healing in diabetic patients. Although there is not a lot of literature on the use of ankle taping for plantar foot ulcer healing, some studies have indicated that this method could be beneficial when used around the wound.
To accomplish this, we used functional ankle KT for plantar ulcers and measured peak plantar pressures, active ankle dorsiflexion, and ulcer healing after eight weeks.
The most important result observed in this study was the change in peak plantar pressure scores. Plantar pressure is not routinely assessed in clinical practice, which reduced the experimental group towards that due to a reduction in the active range of dorsiflexion, which improves plantar ulcer healing. The KT group showed a statistically greater reduction than the sham control group.
Ankle taping is commonly employed to prevent and cure foot and ankle diseases. Research indicates that traditional taping can effectively manage foot movements, particularly excessive pronation, and plantar flexion while walking. Kinesiotaping (KT) is becoming increasingly common [13]. A recent study has investigated the impact of KT on clinical outcomes related to plantar flexion. The findings indicate that the KT group experienced more significant clinical advancements than standard clinical care. However, it is important to note that the lack of a control group constrained the study for comparison purposes [14].
Additionally, Sawkins et al conducted a study that showed a placebo effect of functional taping in individuals with unstable ankles. Participants reported feeling more comfortable and confident, but their biomechanics had no observable change. Also, Luque-Suarez et al. demonstrated the immediate effectiveness of neuromuscular taping and functional taping. They observed significant and clinically meaningful improvements in correcting pronated and supinated hind foot postures when applying placebo neuromuscular tape with no actual stress (sham-tension) [15]. Furthermore, Seo HD et al conducted a study to explore the impact of kinesio tape on ankle mobility function in individuals with and without foot ulcers. The researchers determined that kinesio tape can rapidly reduce foot pressure and enhance human performance. Additionally, it may shift the pressure on the sole, which aids in healing ulcers. Nevertheless, there is an improvement in the patient’s postural stability with PFUs [16].
In addition, Lin CC et al found that the use of an ankle KT enhances the flexibility of the ankle and knee joints, reduces the speed at which force is applied to the joints, and lowers the likelihood of damage during walking. This treatment promotes efficient healing and decreases the likelihood of recurring wounds [17]. Correspondingly, Tobruk MS et al demonstrated that the application of the KT method could effectively improve ankle motion and assess the pressure on the foot’s sole. This method provides valuable insights into foot injuries and significantly impacts walking using Kinesio tape. The positioning of the foot plays a crucial role in redistributing pressure and absorbing shock during walking, particularly for diabetic patients [18].
Besides, Griebert et al. discovered that KT has a substantial effect on reducing plantar pressures. The researchers examined individuals with medial tibial stress syndrome, a common overuse injury among individuals who engage in regular physical activity— the elastic therapeutic tape benefits muscular function by improving muscle efficiency and effectiveness [19]. In a study conducted by Guner S et al it was determined that applying kinesiology tape (KT) to the arch of the foot in healthy individuals does not result in any immediate changes in walking plantar pressures [20]. Further, Cornwall et al. utilized tape with a 100% elongation, but their evaluation of static kinematics did not reveal any enhancement in posture 24 hours following the administration of Kinesio Tape, in comparison to the application of sham Kinesio Tape without stress [21]. Also, Kiseljak et al. Hence, according to his perspective, the KT Functional Correction Technique was deemed superior to the KT Muscle Facilitation Technique [22] regarding diminishing walking plantar pressures.
Alternatively, these changes in the plantar pressures shown in this study are not similar to other walking pressure studies of functional taping in a similar group of participants with plantar foot ulcers which explained by Sullivan et al. demonstrated substantial elevations in plantar pressure in the lateral midfoot region and reductions in the medial forefoot and hindfoot areas. There were no alterations observed in the middle part of the foot or the outside part of the front foot. The pressure investigations conducted on low-dye taping do not indicate that taping leads to a consistent alteration in foot pressures. However, it remains to be seen whether these findings are due to unreliable measurements of plantar pressures or variations in polarography systems [23].
Additionally, García-Madrid et al. demonstrated that the plantar pressure in the big toe and the first, second, third, and fourth metatarsal regions remained unchanged before and after the application of kinesio tape, indicating no significant difference. However, a significant difference was seen in the fifth metatarsus. The results indicate that the heel area experienced the maximum pressure both before and after applying kinesio tape, while the fourth metatarsus experienced the lowest pressure. This reduced the overall time required for ulcer healing compared to utilizing standard treatment alone. Nevertheless, the decrease in pressure is consistently lower [24].
The existing data on the efficacy of functional ankle taping in correcting plantar ulcers and promoting healing has certain limitations. There needs to be more sample numbers, and the lack of follow-up data is among the limitations. In future studies, the scientific community should consider employing bigger sample sizes and collecting follow-up data to evaluate the long-term sustainability of treatment outcomes. Furthermore, further research is required to provide a more comprehensive understanding of the processes via which these treatments operate. Gaining comprehension of their functioning could streamline treatment methods and enhance therapy outcomes.
Conclusion
The study found that correcting ankle taping has an impact on various factors including peak plantar pressure, ankle dorsiflexion, wound area, and wound volume. This correction leads to a reduction in peak plantar pressure, wound area, and wound volume, while also boosting active ankle dorsiflexion.
The study indicated that functional ankle taping correction affects peak plantar pressure, ankle dorsiflexion, wound area, and wound volume by reducing peak plantar pressure, wound area, and wound volume and increasing active ankle dorsiflexion.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Author contributions
Conflict of interest
The authors have no conflict of interest to report.
Funding
None.
Data availability
The data that support the findings of this study are available on request from the corresponding author.