
Abstract
PURPOSE:
Youth with physical disabilities are at an elevated risk for poor psychosocial health. Pediatric medical camps are one common intervention utilized to provide short-term psychosocial support. However, there is a growing criticism that the effects of such programs diminish as participants return to home and school settings post residential camp experience. A post camp support intervention, the first known in the literature, was tested for perceptions of mattering and self-esteem. Specifically, this study examined the psychosocial effect of a year-round mentoring and online support program as an adjunct to residential camp (intervention) as compared to peers that attended only the summer residential experience (comparison group).
METHODS:
A quasi-experimental design using an intervention and comparison group was implemented. Data were analyzed using a repeated measures analysis of variance to test for within group and between group effect.
RESULTS:
A small effect (partial
CONCLUSIONS:
The online and mentoring support program appeared to improve perceptions of mattering three months into implementation. Future implications center on the refinement of the support program and suggestions for further longitudinal research.
Introduction
Youth with physical disabilities encounter many documented social challenges. Shields et al.’s [1] systematic review of self-concept in adolescents with cerebral palsy concluded that self-concept was lower in a variety of domains including social acceptance, scholastic competence, and appearance. Fewer social activities, intimate relationships, and plans for college relative to a comparison sample have also been documented [2]. Furthermore, a review of the literature posits that youth with cerebral palsy have less robust social relationships in general, delayed dating behavior, and difficulty developing intimate relationships compared to peers without physical disabilities [3]. Altogether, this population is at-risk psychosocially. It is important for future research to develop, test, and refine evidence-based approaches that promote positive psychosocial health.
One common therapeutic approach aimed at supporting adolescents with diagnosed health conditions is enrollment in medical specialty camps with similar peers. Positive short-term psychosocial effects from participation in residential medical specialty camps are commonly seen in the literature. Studies have examined various constructs such as self-esteem, social acceptance, and quality of life [4, 5, 6]. Despite these documented short-term gains, there is a documented loss in psychosocial effect at follow-up several months after campers return to their more integrated home communities [7]. Likely, this is a contributing factor in Plante et al.’s [8] conclusion that despite medical camps being identified as one of five major pediatric program approaches, there is still a lack of enthusiastic support due to dissipating long term effects.
Seminal theoretical work on social inoculation theory, and subsequent application to health programming, may be an applicable lens to evaluate medical camps [9, 10, 11]. For example, youth typically attend a short term residential experience that is finely crafted for their specific needs, e.g., accessible facilities filled with peers experiencing the same health condition. However, after the conclusion of this short residential experience, then they are placed directly back into a more stressful integrated environment as they return to home communities. Dawson [12] has argued that a new medical camp program framework is needed to counter the extinguishing effects at medical camps by offering booster interventions in the months following residential summer camp.
Literature review
Mattering
Rosenberg and McCullough’s [13] work to discover the importance of mattering was seminal in understanding the relevance of this psychological filter in the lives of adolescents. Mattering is evident, according to Elliot et al. [14], when others invest, attend to, and have a reliance on the person of interest. In short, those who feel as though they matter also feel as though they are significant in the lives of others. The need to belong is paramount in Maslow’s Hierarchy of Needs [15] in that once physiological and safety-oriented needs are met, feelings of belonging become critical within the hierarchy. In turn, mattering may result in positive social health outcomes. Elliott et al. [16] found that adolescents who perceive that they matter are significantly less likely to have suicidal ideation. Raque-Bogdan et al. [17] found in a sample of college students that mattering mediated the relationship between attachment orientation and mental health. The authors went on to assert that mattering is a promising agent for future therapeutic interventions. Others have found that mattering is positively associated with well-being and negatively associated with worry in American college students [18]. Furthermore, Demir et al. [19] found that the mediating factor between friendship and happiness is that of mattering. Given the positive health outcomes related to having a positive perception of mattering, it was reasonable to utilize this construct to assess the mentoring and online support program.
Self-esteem
The construct of self-esteem has been widely researched in the literature, yet a firm definition is still evolving. The global body of evidence on self-esteem defines this construct as one’s positive or negative attitude towards oneself [20]. Also, it focuses more on a person’s attitude about themselves while the aforementioned mattering is focused on how significant that person feels they are to others [20, 14]. Zimmerman et al. [21] examined the self-esteem of youth in the sixth grade through tenth grade to determine longitudinal changes throughout development. Adolescent females were more likely to have their self-esteem decline as they aged as compared to male peers. The largest drop in self-esteem took place from the sixth to the eighth grade. Generally, youth with higher self-esteem appeared to use alcohol less, were not as influenced by peer pressure, and had better grades.
Having a health condition can result in lower levels of self-esteem compared to peers without disabilities [22]. Schieman and Campbell [23] found that age was negatively associated with self-esteem among people with disabilities such that self-esteem decreases as people with disabilities age. More specific to gender effects on self-esteem, Magill and Hurlbut [24] found that females with cerebral palsy have a lower self-esteem than males with the same health condition. Furthermore, males with cerebral palsy had similar self-esteem scores to males without cerebral palsy. Due to a high desire to be in a relationship with a significant other, female adolescents with cerebral palsy that have low sexual and body esteem are also at-risk for intimate partner abuse as they grow into adulthood [25]. Taken together, females with physical disabilities appear to be an at-risk group when it comes to self-esteem.
Assessing support interventions based on changes in self-esteem is common. Devine and Dawson [4] documented increased self-esteem during medical residential camp participation for youth with craniofacial differences. However, self-esteem dissipated 6–8 weeks after returning to their home communities. Shaw and Gant [26] found that perceptions of social support from an online chat platform improved the self-esteem scores of participants. Readdick and Schaller [27] examined the effects of a residential camp on economically disadvantaged youth and found improvements in self-esteem from the start to end of camp for campers six to twelve years of age. The literature posits that residential camp and online support may have the potential to impact self-esteem.
Theoretical foundation
Leary’s Sociometer Theory of self-esteem [28, 29] provides the theoretical foundation for this study. Sociometer Theory posits that self-esteem is a sociometer reflecting the quality of relationships one has with other people. To the extent that one feels socially included and valued, self-esteem may rise. Conversely, self-esteem decreases when one perceives there is deterioration in social inclusion and feeling socially valued. Rosenberg and McCulough [13] found that mattering and self-esteem were positively associated, which supports the basic concept of the sociometer theory of self-esteem. Dixon and Kurpius [30] note a connection between mattering, self-esteem, stress, and depression in college students. Sociometer Theory is a strong theoretical foundation for the evaluation of self-esteem and mattering within the mentoring and online support program.
Research procedures
This study sought to examine the effect of a year-round support program designed to support psychosocial effects of a medical specialty camp in the months following a residential summer camp. The year-round support program included an assignment of an adult mentor with a physical disability to an adolescent camper with the same or similar physical disability. Prior to the beginning of the program, mentors had background checks and were interviewed by the camp director, and subsequently completed an online training program facilitated by a research team member. The online training consisted of an overview of the research that informed the program’s safety and liability rules and regulations, along with expectations from the mentors. Expectations included a one-year commitment to the program, meeting at least twice monthly 1:1 with the mentee, attending an in-person event once, and being present during monthly collective group meetings where all mentors and mentees were present. Initially, they had an opportunity to meet during the summer camp experience and then began a year-long mentoring relationship following the residential camp.
A structured online support program was created in addition to the one-to-one mentoring relationship to provide structured one-hour online meetings once per month between the collective group of mentees, mentors, and at least one trained camp staff member. Each online meeting was led by a nationally certified recreational therapist who served in an administrative role during summer camp. The online curriculum focused on the following topics germane to the mentees and mentors: 1) adapted sport and recreation opportunities, 2) medical diagnoses, 3) healthy living, 4) career path, 5) college or alternative option, 6) “You’re an inspiration” and other forms of stigma, 7) independent living, 8) driving with a physical disability, 9) social connections, and 10) identity. Attendance as a group of mentees and mentors provided opportunities for them to interact with one another while also providing support between adolescents attending. Individual mentee and mentor pairs were then encouraged to correspond 1:1 at least twice per month via email, texting, social media, or by phone.
The year-round support program was focused on adolescents instead of children based on previous social network findings indicating a strong desire by 13–18 year old campers to connect with non-relatives compared to younger campers 8–12 years of age [31, 32]. Offering programming outside of the residential summer camp experience also followed previous findings indicating adolescents with physical disabilities desired opportunities for social connection and programming in the months following summer camp participation [33]. The mentoring program provided the opportunity for the mentee to meet with an assigned mentor at least twice per month one-to-one in addition to seeing their adolescent peers once per month in collective group online meetings. The current study was designed to examine the effect of the mentoring and online support intervention on the campers’ perceptions of mattering and self-esteem.
Setting
This study took place in the Midwest at a residential medical specialty camp for 80 youth 8–18 years of age with physical disabilities such as cerebral palsy, muscular dystrophy, and spina bifida. Medical care was provided by a regional medical center that staffed the camp with nurses and physicians. In addition, 80 college students studying in various allied health fields were employed as full-time summer staff. The staff were trained for 1–2 weeks before the camp program started. Campers were housed in gender specific accessible cabins with approximately 10 campers in each cabin for the two-week duration of the residential summer camp experience. Programs and activities included climbing towers, equine assisted therapy, zip line, lake, boating, adapted water skiing, adapted scuba diving, archery, crafts, campfires and other traditional camp activities. The staff-to-camper ratio was set at 1 staff to 3 campers along with up to 5 nurses, a physician, and a pharmacist staffing the health center. The camp used a recreational therapy approach utilizing a systematic process consisting of an assessment for each camper, plan of care including therapeutic goals while at camp, the residential camp experience as a social intervention, and daily and end of session evaluations completed by recreational therapy interns and cabin staff to track progression of individual social goals.
Research subjects
Youth 12–18 years of age with physical disabilities were the research subjects. Common diagnoses included cerebral palsy, spina bifida, neuromuscular diseases, mitochondrial myopathy, Pierre Robin Syndrome, double leg amputation, hemiplegia, and other physical disabilities. Campers had a history of attending this camp between 1–11 years. Consent and assent forms were created for the study and approved through the Institutional Review Board at Indiana University. An overview of the research project as well as the consent and assent forms were sent in an email to participating families prior to the start of camp. On the first day of camp, a research team member met with each family to further describe the study and to record consent from parents and assent from adolescents willing to participate. A total of
Intervention and comparison groups
A quasi-experimental design was implemented in that the intervention group had attended summer camp, was assigned a mentor, and invited to monthly online support programming following the summer experience. The comparison group attended the same residential camp experience without an assigned mentor in the months following camp.
The following procedures were used to select the comparison and intervention groups. The camp utilized two villages, Village A and Village B, which were located approximately 200 yards apart. During the two-week camp experience, the participants resided in their cabins. The comparison group was chosen from the campers from Village A that were scheduled to move to Village B the following summer (campers move from Village A to Village B in approximately their 8
Research instruments
The General Mattering Scale [34] was used in this study due to ease of use, widespread application, and positive psychometric properties. The General Mattering Scale is the most cited mattering scale in the literature and uses a five-question approach. Each question is associated with five major components of mattering: 1) interest, 2) being missed, 3) importance, 4) attention, and 5) dependence [18, 19]. Although there continue to be debates as to the best way to measure mattering, this instrument is currently viewed as one of the most widely used scales for mattering. It also met the needs of a short and effective instrument that could be used with youth that have disabilities in the camp setting. The internal reliability of the General Mattering Scale has been noted as consistent with a study on homeless men resulting in a 0.85 internal reliability rate [35]. The Rosenberg Self Esteem Scale has been widely utilized for over fifty years for the measurement and reporting of self-esteem. It is a 10 item instrument and has strong reliability and validity across various population groups including adolescents [36, 37].
The Rosenberg Self-esteem Scale is a ten-question instrument with up to a potential of 30 points. The internal reliability (Cronbach’s alpha) for this study with adolescents that have physical disabilities was 0.801. Questions three (0.349) and four (0.361) had the lowest internal reliability for the instrument. However, eliminating these questions would not have improved reliability overall. The General Mattering Scale is a five-question instrument with a possibility of 20 points. The internal reliability of the General Mattering Scale was 0.623 in this study. Question three (0.175) had the lowest internal reliability score. Eliminating this question would have improved reliability just slightly overall.
The General Mattering Scale [34] and Rosenberg Self-esteem Scale [36] were administered during the thirteen-day residential camp in the middle of the program on the sixth day of attendance (pre-test) and again three months after camp (post-test) with the intervention and comparison groups respectively. The pre-test measures were collected within the cabins during the summer experience. Participants were asked to complete both instruments independently unless support was verbally requested. At three-months post camp, the instruments were sent to the homes of each participant with the same instructions. An envelope with pre-paid postage was included to encourage a strong response rate. In both cases, the adolescents were instructed to fill out the instruments independently and were given help only when needed. In both circumstances, paper copies were utilized to maintain consistency. Once collected, the pre-test and post-test data were paired to maintain connection along with demographic variables. To maintain anonymity, the names of the campers were removed.
Gender, age, and mentor demographics by group
Gender, age, and mentor demographics by group
Baseline scores on self-esteem and mattering in each group
Total post scores for comparison and intervention groups
Total post scores by gender
A series of hypotheses were established for this study. Both self-esteem and mattering hypotheses were written separately to tease out any differences seen in the data between the two psychosocial constructs. Both within group and between group differences were captured.
Null Hypothesis 1: There will be no difference in self-esteem scores of the treatment group (enrolled in program) and the comparison group after 3 months (i.e., Comparison mean change = Treatment mean change)
Alternative Hypothesis 1: The scores of self-esteem in the treatment group (enrolled in program) will be greater than the comparison group after 3 months (i.e., Comparison mean change < Treatment mean change)
Null Hypothesis 2: There will be no difference between pre-test and post-test self-esteem scores of the treatment group (treatment mean pretest
Alternative Hypothesis 2: The post-test self-esteem scores of the treatment group will be greater than the pre-test scores of the treatment group (treatment mean pretest < treatment mean posttest)
Null Hypothesis 3: There will be no difference in mattering scores of the treatment group (enrolled in program) and the comparison group after 3 months (i.e., Comparison mean change
Alternative Hypothesis 3: The mattering scores of the treatment group (enrolled in program) will be greater than the comparison group (i.e., Control mean pre-test
Null Hypothesis 4: There will be no difference between pre-test and post-test mattering scores of the treatment group.
Alternative Hypothesis 4: The post-test mattering scores of the treatment group will be greater than the pre-test mattering scores of the treatment group (i.e., Treatment mean post-test
Analysis
The Levene’s test [38] was used to check equality of variances. A parametric test was determined to be suitable for this analysis over a non-parametric approach. A repeated measures analysis of variance (ANOVA) was utilized comparing within groups and between groups using the Statistical Package for the Social Sciences (SPSS). An ANOVA was utilized to test within group and between group differences. Within group differences included a pre-test and post-test for both the intervention group and comparison group. Between group differences were also compared for the comparison and treatment groups.
Findings
Descriptive statistics
Demographic data for the intervention (camp attendance and mentor assigned) and comparison group (only camp attendance) are presented in Table 1. The ratio of males to females was similar in each group with 11 males and 15 females in the intervention group and 16 males and 19 females in the comparison group. The intervention group was significantly older (
Table 2 reports the sample size, baseline mean scores, standard deviation, and standard error for the comparison and treatment groups. The comparison group included 35 participants while the intervention group had 26. Generally, the comparison group started with a higher self-esteem overall at 22.26 compared to the treatment group at 20.50. This trend continued for the mattering construct with the comparison group beginning with a 16.57 average mattering score compared to the treatment group average of a 15.68 (see Table 2).
Table 3 provides an overview of the differences in post-scores for self-esteem and mattering based on group identification, i.e., intervention versus comparison groups respectively. The total overall scores for self-esteem and mattering are reported. A paired
Table 4 provides further delineation based on any differences in gender for self-esteem and mattering post-test scores. Male campers appeared to have higher post self-esteem scores while mattering scores were similar.
Figures 1 and 2 display the estimated marginal means for both self-esteem and mattering at pre-test (during residential camp) compared to post-test (three months post-camp) respectively. The mattering scores increase for the intervention group by nearly two points while the comparison group remains flat from pre-test to post-test. The self-esteem scores appear to lessen from pre-test to post-test for both comparison and treatment groups. The lessening in self-esteem follows a similar trend in the extinguishing psychosocial effects of medical camp participation seen in other studies [7, 12], i.e., psychosocial scores are higher during medical specialty camps and then tend to extinguish upon return to home and school settings.
Estimated Marginal Means for Mattering (Pre vs. Post).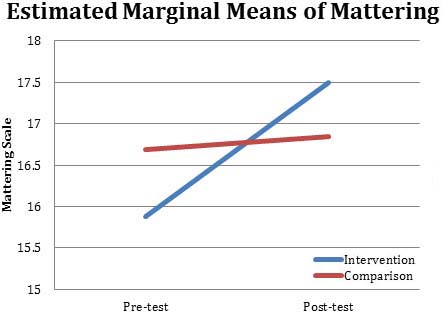
Estimated Marginal Means for Self-esteem (Pre vs. Post).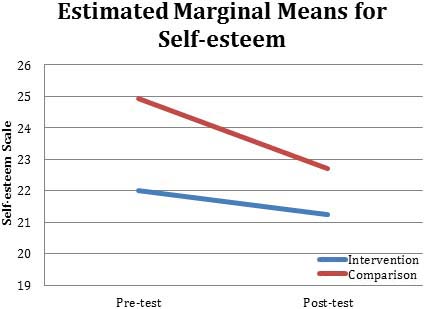
Partial eta squared was utilized to determine effect size of the intervention on both self-esteem and mattering. This is a commonly recommended approach for social science research when using an ANOVA [39, 40]. Effect size for partial eta squared is based on a standardized scale in which 0.02 is a small effect, 0.13 indicates a medium effect, and 0.26 a large effect. This standardized measurement standard can be seen in Table 5 below.
Partial eta squared effect size calculations
Partial eta squared effect size calculations
Table 6 below presents the data from the analysis of variance calculations. The data indicate that there was no effect on self-esteem within or between groups for this test. A medium effect was detected in the mattering scores from pre-test to post-post (within group) for the intervention group in addition to a small program effect in comparing between means of the comparison and intervention groups. Perceptions of mattering appear to be a potential outcome of the mentoring and online support intervention.
Repeated measures analysis of variance (computed using alpha
The first two hypotheses focused on the effects of the year-round support program on the self-esteem of campers in the program versus those not yet in the program. Based on the results of the repeated measures analysis of variance, this study fails to reject hypothesis one and two. The last two hypotheses centered on the effects of the mentoring intervention on mattering. This study fails to reject the null hypotheses three and four. However, using partial eta squared, a moderate effect size for mattering is seen in the data at 0.133 for pre to post-test within group means and a small to medium effect at pre to post between treatment and comparison groups at 0.096. Furthermore, a paired T test for those participants completing both the pre-test and post-test was completed. Although it lacked statistical power due to the difficulty in capturing follow up data from participants, this resulted in a medium effect size for Cohen’s
Changes in mattering approaches statistical significance from pre- to post-test. After conducting a power analysis using G Power, it was determined that to obtain 80% power it would require a sample size of 32 subjects and to obtain 90% power it would require a sample size of 42 subjects. Although the pre-test sample was strong, the follow-up data fall below this threshold. Upon analysis of effect size, a moderate effect was seen in the within group means for mattering and a small effect between the comparison and intervention group while a paired T-test resulted in a moderate effect for pre-test to post test for mattering using Cohen’s
In the present study, self-esteem did not appear to be positively impacted by the program despite seeing an effect in perceptions of mattering. However, there was a negative effect in that the self-esteem of clients appeared to decrease from the time they attended camp compared to three months post camp. Given the theoretical foundation of the sociometer theory [29] and further evidence of the correlation between self-esteem and mattering [13, 14], this is a somewhat surprising finding. Mattering may be a more sensitive psychosocial construct as compared to self-esteem which could take longer to change. It does appear that self-esteem for both the comparison and intervention groups follows the same trend line that other medical camp studies have indicated in that there are extinguishing effects upon return to integrated home communities. For example, Devine and Dawson [4] found a significant increase in self-esteem while attending residential camp for youth with craniofacial disabilities with a return to baseline in follow up self-esteem scores three months after summer camp. Arnoldo et al. [41] also reported difficulty in finding any improvements in the self-esteem of campers with burns from pre (start of camp) to post-test (shortly after returning home) during a medical specialty camp. The results of the current study appear to follow this same pattern with self-esteem.
Future implications
The year-round support program appears to have promise related to the mattering construct. Many lessons were learned in implementing this pilot intervention. Future work should attempt to accomplish six objectives. First, future studies need to be adequately powered which can be a challenge with this population. Many of the research subjects were lost at the follow up data collection point. This was a limitation of the data and should be considered in the future. With guidance from the power analysis, it is suggested that future studies target a minimum sample size of 40–50 at both pre and post-test. Second, the program should be pilot tested for adolescents with other health conditions. It is suggested that future studies examine populations impacted by craniofacial differences, cancer, burns, and other health conditions in which medical residential camps are commonly held without follow-on support interventions. Third, given the lack of evidence for self-esteem in this study and others, future studies should consider other psychosocial constructs such as loneliness or social acceptance that may be more responsive to this type of intervention. Fourth, in this study, only three months had passed from the pre to post test. Data were collected at the 3 month time frame in an effort to provide data that aligns with camp studies that have collected follow-on data 3 months post camp in an effort to add to the medical specialty camp literature [4]. Future studies should capture follow-on data points 12 months after subjects are enrolled in the treatment group. Fifth, the quality of the mentoring to mentee relationship should be monitored in the future as a mediating variable, e.g., number of contacts and closeness of relationship. Lastly, through implementation of this program, it is feasible that 1–2 mentors could be hired to mentor the entire group of campers. This would provide consistency within the mentorship role in addition to providing a person with a disability a rewarding and quality full or part time job.
Limitations
A limitation of this study was that random assignment was not feasible. Thus, intervention and comparison groups differed in terms of age. This may have resulted in natural developmental differences. Also, over half of the groups were lost at follow-up, thus reducing follow-up sample sizes. Lastly, the low sample size resulted in difficulty reaching statistical significance at the 0.05 alpha level despite documented small and medium effects for mattering. Results should be interpreted with caution until further testing can be completed.
Conclusions
The findings from this study indicate that implementing an online mentoring program in addition to traditional residential summer camp experiences, may have a small to medium positive effect on the perceptions of mattering for adolescent participants with physical disabilities three months post camp. Online mentoring did not positively impact self-esteem. This appears to be a promising support intervention which should be developed and tested further with youth that have various health conditions. This should be for greater lengths of time, with different psychosocial instruments, and with adequately powered studies.
Footnotes
Conflict of interest
The authors report no conflicts of interest.