
Abstract
Background:
Transcranial direct current stimulation (tDCS) is a non-invasive brain stimulation technique, which can modulate cortical excitability and combined with rehabilitation therapies may improve motor recovery after stroke.
Objective:
Our aim was to study the feasibility of a 4-week robotic gait training protocol combined with tDCS, and to study tDCS to the leg versus hand motor cortex or sham to improve walking ability in patients after a subacute stroke.
Methods:
Forty-nine subacute stroke patients underwent 20 daily sessions (5 days a week for 4 weeks) of robotic gait training combined with tDCS. Patients were assigned either to the tDCSleg group (n = 9), receiving 2 mA anodal tDCS over the motor cortex leg representation (vertex), or an active control group (n = 17) receiving anodal tDCS over the hand motor cortex area (tDCShand). In addition, we studied 23 matched patients in a control group receiving gait training without tDCS (notDCS). Study outcomes included gait speed (10-meter walking test), and quality of gait, using the Functional Ambulatory Category (FAC) before and after the 4-week training period.
Results:
Only one patient did not complete the treatment because he presented a minor side-effect. Patients in all three groups showed a significantly improvement in gait speed and FAC. The tDCSleg group did not perform better than the tDCShand or notDCS group.
Conclusion:
Combined tDCS and robotic training is a safe and feasible procedure in subacute stroke patients. However, adding tDCS to robot-assisted gait training shows no benefit over robotic gait training alone.
Introduction
Stroke is the primary cause of motor disability in adults. About one third of the patients who suffer from stroke do not reach complete motor recovery. Gait impairment is the most common complaint among survivors (Von Schroeber, Coutts, Lyden, Billings, & Nickel, 1995). Approximately 70% of patients with stroke regain at least some walking ability within a period of 12 weeks after physical therapy (Jørgensen, Nakayama, Raaschou, & Olsen, 1995), but as many as 30% do not regain walking ability (Krishnan, Ranganathan, Kantak, Dhaher, & Rymer, 2012; Krishnan, Kotsapoukis, Dhaher, & Rymer, 2013; Wade, Wood, Heller, Maggs, & Langton Hewer, 1987).
Extensive research has been conducted in order to elucidate the best approach to develop an effective rehabilitation program to restore gait following stroke. Modern concepts favour a task-specific, repetitive locomotion training (Mehrholz, Elsner, Werner, Kugler, & Pohl, 2013). Specifically, electromechanical devices like Gait-trainer (Hesse et al., 2001) or Lokomat (Wallard, Dietrich, Kerlirzin, & Bredin, 2015) are being used for gait restoration, showing improvement in gait parameters in patients with subacute (Schwartz et al., 2009) and chronic stroke (Li et al., 2015). Despite these advances, not all patients reach satisfactory recovery. Therefore, there remains a need to examine interventions that might enhance the benefits of robot-assisted gait rehabilitation.
In the last decade several non-invasive brain stimulation techniques have aimed to promote adaptive plastic changes and inhibit maladaptive changes to enhance motor recovery after stroke (Fregni et al., 2005; Claflin, Krishnan, & Khot, 2015). tDCS is a non-invasive and painless procedure to modulate cortical excitability of motor areas and induce changes in the descending corticospinal output (Nitsche & Paulus 2000). tDCS involves application of a low-intensity electrical current between 2 electrodes placed over the scalp (Nitsche et al., 2008). tDCS can either increase (e.g., anodal) or decrease (e.g., cathodal) cortical excitability (Nitsche α Paulus, 2000) and thereby modulate cortical activity levels. tDCS can enhance motor learning and facilitate motor training (Zimerman et al., 2013). The combination of rehabilitation therapies with tDCS may enhance the beneficial effects of the former (Tanaka et al., 2011; Sohn, Jee, & Kim, 2013; Dimyan, & Cohen, 2010). When targeting hand function, beneficial effects of tDCS in stroke patients have been extensively studied and demonstrated (Lüdemann-Podubecká, Bösl, Rothhardt, Verheyden, & Nowak, 2014). Specifically, tDCS increases the therapeutic benefits of upper extremity robotic training (Edwards et al., 2009).
In the present study, we examined the feasibility of combining tDCS with robot-assisted gait training, and whether tDCS to the leg motor area enhances its benefits. Jeffrey et al. (Jeffery, Norton, Roy, & Gorassini, 2007) showed that tDCS on deeper cortical structures that innervate muscles of lower leg can modulate corticospinal projections to leg muscles. We hypothesized that robot-assisted gait training would be more effective when coupled with anodal tDCS over the vertex (leg motor cortex; tDCSleg) than when tDCS was applied over the hand motor cortical representation (tDCShand) or no tDCS was applied (notDCS).
Methods
Participants and study design
This was a single-blind, active-control, prospective study. The participants were sequentially assigned to one of two tDCS groups: 1) tDCS over the vertex (leg motor cortex area) (tDCSleg) or 2) tDCS over the hand motor cortex representation in the affected hemisphere (tDCShand). In addition, the data of 23 stroke patients who underwent the same gait rehabilitation program without tDCS (Conesa et al., 2012) was used as a further control group (notDCS). All patients were naive to tDCS and blinded to the intervention.
The inclusion criteria were: 1) age 18 to 65 years; 2) no prior stroke history; 3) able to stand on a flat surface; 4) presence of hemiparesis; 5) time since onset >2 weeks and ≤6 months; 6) ability to follow simple orders and give written informed consent for the study, which had been approved by the Institutional Review Board of Institut Guttmann in accordance with the Declaration of Helsinki. Patients were excluded if they presented with any of the following characteristics: 1) medically unstable; 2) severe spasticity with Ashworth ≥3; 3) joint contracture and severe limitation of range of motion; 4) pressure-ulcers in pelvic region or lower limb; 5) contraindications for brain stimulation (sensitive scalp or skin lesions, history of seizures, family history of epilepsy, presence of metal head implants).
Physical therapy and Gait training protocol
All patients received standard care for Stroke rehabilitation at our institution. The program comprised 5 hours of therapy, 5 days per week, including training in activities of daily living, occupational therapy for the upper extremities, fitness training, introductory activities to adapted sports, hydrotherapy, and robotic gait training as described below, complemented with conventional gait training therapies on parallel bars.
Patients received daily robot assisted gait training using one of two electromechanical systems, Gait Trainer (Hesse et al., 2001) or Lokomat, (Wallard et al., 2015) (5 days/week) across four weeks. Both of these assistive devices have been previously shown to be equivalent in clinical improvement in neurological patients (Benito-Peñalva et al., 2012).
Each gait training session lasted between 30 to 45 minutes depending on signs of fatigue and clinical judgement by the supervising physical therapist, who in all instances was unaware of the study group assignment.
tDCS protocol
tDCS was administered using a Magstim Edith DC stimulator (NeuroConn, Germany). The electric current was applied by two surface sponge electrodes (35 cm2 surface area) soaked in saline solution connected to a battery-driven constant current stimulator, following the latest safety recommendations (Krishnan, Santos, Peterson, & Eginger, 2015). According to the protocols used in previous studies that have studied tDCS on the leg motor area and its effects on gait rehabilitation (Jeffery et al., 2007; Jayaram & Stinear 2009; Madhavan, Weber, & Stinear, 2011), patients received 2 mA tDCS during the first 20 minutes of the gait training period. After this period, the stimulator was switched off, and the electrodes remained in place so that the training was continuous. 1) The tDCSleg group received tDCS stimulation with the anode placed over the vertex (Cz) and the cathode over the right supraorbital area. 2) In the tDCShand group, the anode was placed over the primary motor cortex of the affected hemisphere (at C3 or C4, depending on the stroke location), thus targeting the hand motor cortical representation. The cathode was placed over the contralateral supraorbital area.
Clinical and functional evaluation
Functional evaluations were done at the beginning and the end of the 4-week training period, and included: 1) Ten Meter Walk Test (10MWT) to calculate gait speed. This scale is considered to be more sensitive to changes in mobility after stroke (Rossier, & Wade, 2001); 2) Functional Ambulatory Category (FAC) (Holden, Gill, Magliozzi, Nathan, & Piehl-Baker, 1984): to categorize each subject into five different groups ranging from “0” (non-functional ambulatory patient) to “5” (ambulatory), depending on how much assistance the subject required when walking.
Data analysis
Data are presented as mean±standard deviation (SD). Change scores were calculated for each individual patient by subtracting baseline data from the evaluation at the end of the last tDCS session (4 weeks). Average change scores were calculated for each group. Since distribution of the data was not normal according to the Kolmogorov-Smirnov-test, Wilcoxon-t was used. The Kruskal-Wallis test was used for multiple comparison (for change score between 3 groups) and MannWhitney-U test for post-hoc non-paired comparisons when necessary. Statistical analyses were performed using SPSS 16.0. Significance level was set as p < 0.05 with Bonferroni correction for multiple comparisons.
Results
One hundred and forty-seven subacute stroke patients were identified as potential participants for this study. Fifty of those patients met the inclusion criteria, gave informed consent and participated in the study (see Fig. 1, consort diagram). There were 35 males and 15 females; mean age: 48,7 years±11.2 years; mean time from onset 1.9 months±1.1 months. Twenty-nine patients had an ischemic stroke, and 21 a haemorrhagic stroke. A total of 23 patients were assigned to the notDCS group, and 27 patients were assigned to the combined gait and brain stimulation training group. One subject from the tDCSleg group drop out due to side-effects, so we end up with 9 subjects in this group and 17 in the tDCShand group. The characteristics of all patients for each group are described in Table 1. There were no significant differences between the groups for age, gender, type of stroke, time since onset, affected hemisphere and etiology. and initial FAC score. Neither differences were found in the baseline values of velocity and FAC (Table 2).

Flow chart of the study protocol.
Demographic and clinical characteristics of participants
10 MWT: Ten Meter Walk Test; FAC: Functional Ambulatory Category.
Comparisons between baseline values
Patients in all three groups showed significant improvement in FAC and in gait velocity after the 4-week intervention (Table 3) groups (Fig. 2).
Gait parameters results. Group data of the 10MWT and the FAC for the 3 intervention group before and after 4-week training period
10 MWT: Ten Meter Walk Test; FAC: Functional Ambulatory Category.
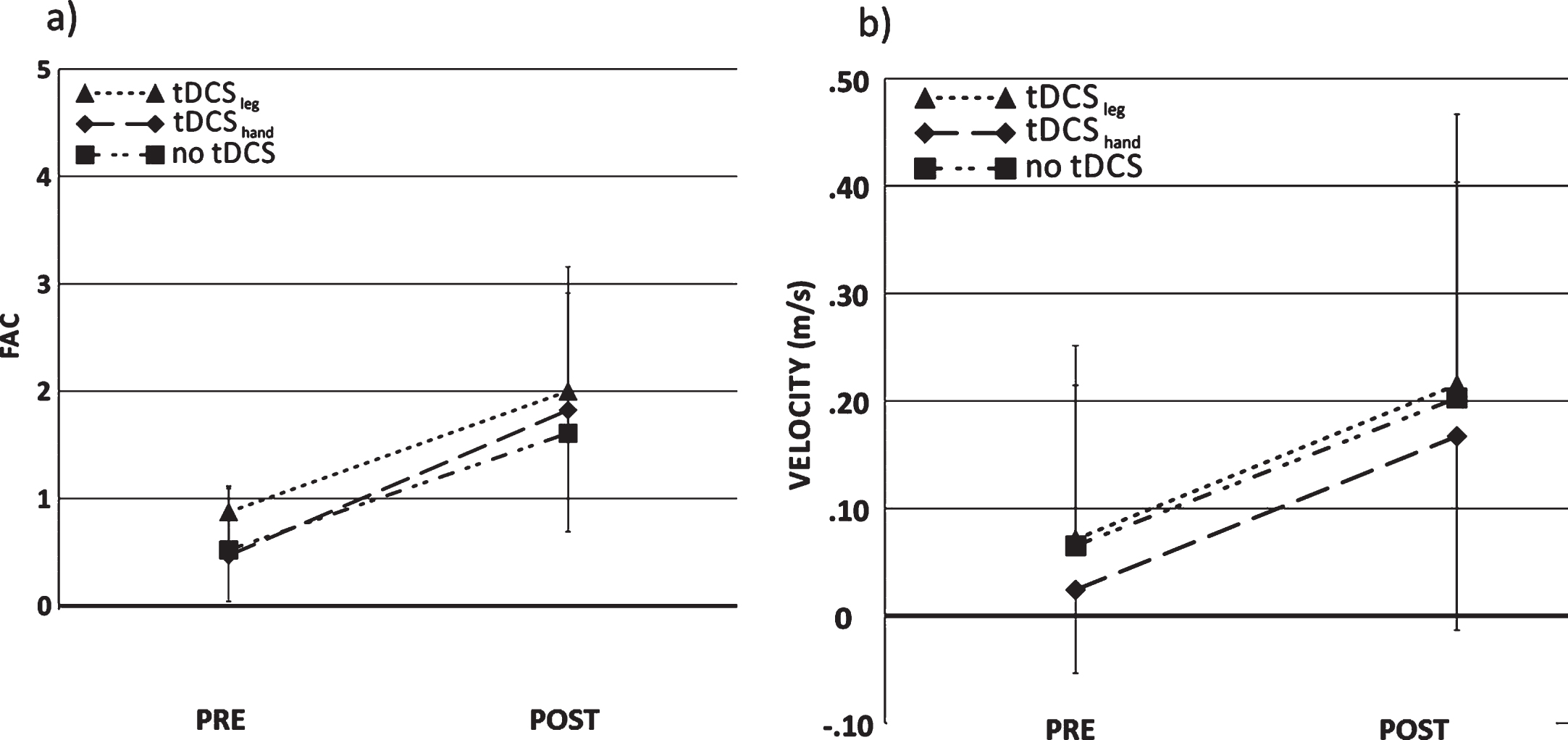
Functional Ambulatory Category a) and Gait velocity b) of each group before and after the four-week intervention.
The 9 patients in the tDCSleg group finished the training protocol with significant improvements in both FAC and gait speed (10MWT). FAC pre: 0.88±0.835; FAC post: 2±1.309 (p = 0.001); gait speed pre; 0.07 m/s±0.143 m/s; gait speed post: 0.21 m/s±0.189 m/s (p = 0.02).
In the active control (tDCShand) group, all 17 patients finished the training with significant improvements in FAC and gait speed (10MWT): FAC pre: 0.47±0.624; FAC post: 1.82±1.33 (p = 0.002); gait speed pre: 0.024 m/s±0.078 m/s; gait speed post: 0.16±0.18 m/s(p = 0.008).
Finally, the 23 patients in the notDCS control group also had significant improvements in the two outcome measures: FAC pre: 0.52±0.593; FAC post: 1.61±1.305 (p = 0.03); gait speed pre: 0.065 m/s±0.186 m/s; gait speed post: 0.2±0.264 m/s (p = 0.002).
The change score of improvement between groups was not statistically significant for gait speed (Kruskal-Wallis test; p = 0.8), nor FAC (p = 0.9).
None of the patients undergoing the combined gait-training and tDCS intervention experience any problems or significant side-effects. Overall, all patients in both tDCS groups (leg and hand) showed good tolerance to brain stimulation. Two patients felt a slight itching sensation, which was transitory and thus, did not affect the intervention. Only one patient, in the tDCSleg group was excluded due to a mild headache episode during and after stimulation.
Discussion
In the present study we demonstrated the feasibility of combining tDCS with robot-assisted gait training delivered as a four week daily regimen in an inpatient setting. However, the benefits of the robot-assisted gait training were not enhanced by the tDCS whether applied to the leg motor area, or the hand motor area (active control).
Following Jeffrey et al. (Jeffery et al., 2007), other authors have studied the usefulness of tDCS to modulate the corticospinal projection to the leg in stroke patients (Jayaram & Stinear 2009; Madhavan, Weber, & Stinear, 2011). Jayaram et al., 2009, applied one session of 10-min tDCS at 2 mA with an anodal surface of 8.1 cm2 over the cortical leg area on nine chronic stroke patients while walking on a treadmill. They showed an increase in the amplitude of the motor evoked potentials [MEPs] induced by transcranial magnetic stimulation (TMS) in the tibialis anterior and medial hamstrings muscles. Madhavan et al., 2011 also reported an increase in TMS-evoked MEP amplitude in nine chronic stroke patients after tDCS with the anode over the leg motor area (one 15-min session at 2 mA, with anodal surface electrode of 8 cm2). Combining tDCS with conventional physical therapy, Min Cheol Chang et al. (Chang, Kim, & Park, 2015) reported MEPs of shorter latency and higher amplitude after tDCS with the anode over the leg motor cortex (ten 10-min sessions at 2 mA, anodal surface of 8 cm2) in comparison to sham tDCS in 24 patients with early-stage stroke. The increased cortical excitability was sustained for approximately 24 hours. Therefore, a tDCS intensity of 2 mA seems adequate to modulate the activity of the leg motor cortex both in subacute and chronic patients. However, these studies did not evaluate a functional effect on gait.
Madhavan et al., 2011, found a beneficial effect of tDCS to the leg motor cortex on voluntary control of the paretic ankle in stroke patients. Sohn et al. (Sohn, Jee, & Kim, 2013) reported enhanced isometric strength of the affected quadriceps and improved postural stability after tDCS with the anode over the vertex (2 mA, surface electrodes of 8 cm2, during 10 min) in 11 stroke individuals. Tahtis et al. (Tahtis, Kaski, & Seemungal, 2014) reported improved performance in Time Up and Go, despite no changes to biomechanics of the hemiparetic limb in 14 subacute stroke patients following tDCS with the anode over the vertex (2 mA, surface electrodes of 8 cm2, during 15 min).
Two previous studies have evaluated the combination of tDCS with robot-assisted gait training in chronic stroke patients (Geroin et al., 2011; Danzl, Chelette, Lee, Lykins, & Sawaki, 2013). Geroin et al studied 30 chronic stroke patients, combining tDCS with the anode over the vertex with robot-assisted gait training (1,5 mA, surface electrode of 35 cm2, 7 min) during 10 sessions. Training session lasted for 50 min and stimulation was applied during the first 7 min of each session. They compared three different conditions: tDCS combined with robot assisted gait training, robot assisted gait training alone and conventional walking rehabilitation. Consistent with our findings, they did not find any differences between robot-assisted gait training with and without tDCS, but their study lacked an active tDCS control. Danzl et al., reported studied 10 chronic stroke patients (mean FAC: 2, 25±0, 48), combining tDCS with the anode over the vertex with robot-assisted gait training (2 mA, surface electrode of 25 cm2, 20 min) during 12 sessions. They found significant improvement in gait function measured by FAC and the Time Up and Go in the tDCS active condition as compared with sham. Our study failed to replicate these findings in a larger number of patients, but our patients were more acute. Chronic phases of the recovery may be more suitable to see effective results than subacute phases, where spontaneous recovery is still happening and can mask the effect of our intervention.
There is only one prior study on the effects of tDCS combined with physical therapy in early-stage stroke patients. Chang et al. (Chang, Kim, & Park, 2015) studied 24 patients (Mean FAC: 3, 58±0, 51), combining tDCS with the anode over the vertex (2 mA, 10 min) and conventional physical therapy. In addition to the effects on cortical excitability they also evaluated motor function, finding statistically significant differences favoring the active group in lower limb motor strength measured with the lower limb subscale of the Fugl-Meyer Assessment and lower limb Motricity Index. However, consistent with our findings, these effects did not lead to any significant differences in the degree of functional recovery.
Compared with prior studies, our patients received similar stimulation intensity (2 mA) and for longer duration. Hence this is unlikely to have played a role in our negative results. However, in our study we used relatively small surface electrode of 36 cm2, following stimulation procedures successfully used by our group to modulate cortical excitability in motor and non-motor areas, with neurophysiological, neurobiological or therapeutic effects (Murray et al., 2015). Smaller electrode may result in more focal and more superficial stimulation. It is thus possible that our tDCS intervention may have failed to sufficiently modulate activity in the leg motor cortex deep in the interhemispheric fissure. Future studies may evaluate the effect of larger electrodes.
Another factor that is becoming important due to its influence on the results is whether to do the stimulation prior or during the robotic training (Edwards et al., 2009; Giacobbe et al., 2013). Danzl et al. in their study with chronic stroke patients found significant improvement in FAC doing the tDCS stimulation prior to robotic training.
In addition, it is worth noting that compared with previous studies our patients were overall more functionally impaired with a baseline average FAC of 0.5. It is thus possible that less affected patients may show greater benefit from the combination of tDCS with other interventions. Finally, our sample size is relatively small. Nonetheless, our findings reveal a lack of a large effect size of the combination of tDCS with robot-assisted training and thus raise doubt of a meaningful clinical benefit of the combined intervention.
Disclosure
The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University and its affiliated academic health care centers, the National Institutes of Health, or the Sidney R. Baer Jr. Foundation.
Conflict of interest
APL serves on the scientific advisory boards for Nexstim, Neuronix, Starlab Neuroscience, Neuroelectrics, Axilum Robotics, Magstim Inc., and Neosync; and is listed as an inventor on several issued and pending patents on the real-time integration of transcranial magnetic stimulation with electroencephalography and magnetic resonance imaging.
The other authors declare no conflicts of interest.
Footnotes
Acknowledgments
We thank the participants for their contribution to the study. This work was supported in part by grant from NIH R01HD069776 for MC and DE. APL was partly supported by the Sidney R. Baer Jr. Foundation, the NIH (R01MH100186, R01HD069776, R01NS073601, R21 NS082870, R21 MH099196, R21 NS085491, R21 HD07616), the Football Players Health Study at Harvard University, and Harvard Catalyst | The Harvard Clinical and Translational Science Center (NCRR and the NCATS NIH, UL1 RR025758).
We thank Raquel López and Eloy Opisso for assistance with data collection and analysis. JMT was partly supported by Barcelona Brain Health Initiative at Institut Guttmann, NEUROCHILD EYETRACKING (RTC-2014-2228-1) and INNOBRAIN (COMRDI15-1-0017).