
Abstract
Background:
Dementia is a disease that is constantly evolving in older people. Its diverse symptoms appear with varying degrees of severity affecting the daily life of those who suffer from it. The rate in which dementia progresses depends on different aspects of the treatment, chosen to try to control and slow down the development of the illness.
Objective:
The aim of this study is to assess the effectiveness of cognitive training through a Brain Computer Interface (BCI) and the NeuronUp platform in two age groups whose MMSE is between 18–23 MCI (mild dementia).
Method:
32 subjects took part in the study. There were 22 subjects in Group 1 (61–69 years of age) and 10 subjects in Group 2 (70–81 years of age). The criterium for the selection of the groups was to identify the age range with greater improvements due to the training. In order to estimate neuropsychological performance, the subjects were evaluated with the Luria-DNA neuropsychological battery before and after training. This design enables us to evaluate five cognitive areas: visuospatial, spoken language, memory, intellectual processes and attention.
Results:
After training, Group 1 showed significant improvements in almost all the variables measured when compared with Group 2. This reveals a significant increase in cognitive ability, the degree of which depends on the age.
Conclusion:
People with mild dementia may delay cognitive impairment with a suitable cognitive training program.
Introduction
Dementia is a disease that is constantly evolving in older people. Its diverse symptoms appear with varying degrees of severity affecting the daily life of those who suffer from it. The rate in which dementia progresses depends on other aspects of the treatment chosen to try to control and slow down the development of the illness. This treatment may be pharmacological or rehabilitative, or a combination of both. Hence the importance in the first place of establishing a classification of dementia in patients depending on the stage of development which they find themselves in. This would take into account the different clinical signs, as it is not enough just to distinguish if the patients are at an early, medium or advanced stage.
The criteria of dementia according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM IV), requires that patients show cognitive impairment in two or more areas, such as calculations, language, orientation and judgement. It must be noted that an important deficit can lead to an inability to live their daily lives.
Folstein, Folstein & McHugh (1975) detected and followed the evolution of cognitive impairment with the aim of controlling and slowing down the development of the illness. For that purpose, it is firstly recommended to use a neuropsychological test and screening tools, such as Mini Mental State Examination (MMSE). Using MMSE, patients with cognitive impairment in two or more cognitive areas tend to score below 24, considering their age and level of education.
The interest is in studying patients with Mild Cognitive Impairment (MCI) in which deterioration is a transition between normal ageing and mild dementia (Plassman, Langa, Fisher, Heering, Weir, Ofstedal, Burke, Hurd, Potter, Rodgers, Steffens, Willis, & Wallaceg, 2007; American Psychiatric Association, 2013; Petersen, 2011; Nilton, Eder, David, Rosa, Julio & Liliana, 2012). Within this illness, we found different clinical manifestations, a) MCI of amnesia type with isolated impairment in memory. These patients tend to score in the MMSE between 24 and 28 points. However, they often obtain low scores in the section related to the memory, both in this test as well as in other cognitive tests; b) Single-domain MCI, which only affects language or executive function; c) Multiple-domain MCI which is characterized by affecting more than a single cognitive function.
Therefore, MCI is an illness in which many etiologic factors influence, such as degenerative diseases, vascular risk factors, psychiatric conditions, relationships between pathological states, clinical symptoms, with a clinical development can present a stable or even reversible cognitive deterioration (Bahar-Fuchs, Clare & Woods, 2013; Bahar-Fuchs, Clare & Woods, 2009; Andrade & Radhakrishnan, 2001).
Current studies highlight the limitations of the existing criteria, which does not allow definition of a homogenous population, both with regard to subtypes of MCI, or the way it develops. However, the diagnostic procedure proposed as the first step makes possible to identify patients with a high risk of development towards dementia. This is necessary to control or slow down the illness, establishing strategies for an actual functional treatment, as a cognitive training.
In this regard, there are several studies that aim to evaluate the effectiveness of cognitive training in adults with subjective memory loss. The assessment procedure focuses on performing standard neuropsychological tests, which measure the general cognitive capacity, verbal memory and executive functions, among other abilities, before and after the training process (Yi-jung, Yang, Lan & Chen, 2008; Reijnders, Van Heugten & Van Boxtel, 2013; Claire & Woods, 2004, Gomez-Pilar et al., 2016). The assessment of the effects of training varies from six months to five years with some reinforcement sessions (Willis, Tennstedt, Marsiske, Ball & Elias, 2006; Ball, Berch, Helmers, Jobe, Leveck, Marsiske et al., 2002; Rebok & Balcerak, 1989). In the studies reviewed, we have not found cognitive training which involves cognitive processes related to the activities of daily life. This is a crucial factor since it could be a marker for functional autonomy and independence in older people (Gutiérrez, Solera & Larroy, 2012, Carballo-García, Arroyo-Arroyo, Portero-Diaz & Ruiz-Sánchez de León, 2013). Thus, the NeuronUp platform (Fernández de Pierola & Sastre, 2015) improves the quality of life because it contains exercises for rehabilitating, stimulating or learning cognitive functions (orientation, attention, agnosias, praxias, etc.) and practicing common daily activities (basic activities, instrumental activities, education, etc.), like real-life simulators and social abilities. The final purpose of this platform is to improve the quality of life of people (Christensen, 2000; Adams & Victor, 1993; Parkin, 1996; Prigatano, 1999; Sohlberg & Mateer 1989).
In turn, a review of 175 clinical studies published between 1980 and 2011 in the area of cognitive and memory training in adults at risk from dementia (Gates, Sachdev, Fiatore & Valenzuela, 2011), concludes that in this type of population, it is more effective to work on cognitive training than on memory (Gates, Sachdev, Fiatore & Valenzuela, 2011). This suggests that cognitive training enhances brain plasticity.
We must be aware that the ageing of society leads to the prevalence of cognitive impairment (Snyder, Jackson, Petersen, Khachaturian, Kaye, Albert, Weintraub, 2011; Solé-Padullés, Bartres-Faz, Junque, Vendrell, Rami, et al., 2007). Therefore, it is necessary to devise procedures for assessing the cognitive impairment and therapies for preventing its appearance and/or slowing down its effects considering the different age groups.
This study presents a program through cognitive training by means of BCI, which evaluates the progress of the MCI participants’ cognitive capacity in order to avoid cognitive impairment by age groups (under and over 70 years old). In this study, 32 MCI people participated (14 men and 18 women, average age = 68.18, STD = 4.28, age range = 63–81). All of them were selected by the State Reference Centre for Disability and Dependency (CRE in its Spanish initials), San Andrés del Rabanedo (León, Spain).
The Luria-DNA neuropsychological battery (DNA: neuropsychological diagnosis for adults) has been used to prove the efficacy of the training (Christensen, 1979) of each group. The neuropsychological profile evaluation was carried out in five areas: visuospatial, spoken language, memory, intellectual processes and attention. The objective was to evaluate the efficacy of cognitive training, analyzing whether the improvement in the neurological profile of the MCI subjects depends on the age.
Methods
Participants
As previously mentioned, 32 MCI people participated in this study (14 men and 18 women, average age = 68.18, STD = 4.28, age range = 63–81). Using the MMSE, participants reached scores in the range between 18 and 23, which imply the level of dementia related to MCI. The participants had reached between 18–23 MCI level dementia (Folstein et al., 1975). For all the participant, the inclusion criteria were: (i) an age over 60 years, (ii) healthy, without severe neuropsychological pathologies and (iii) first-time users of BCI (no previous BCI experience) and NeuronUp platform. All the patients received the same cognitive training. The participants were divided into two groups. Group 1 consist of 22 subjects (12 men and 10 women, age between 61 and 69 years, average age = 65.95, STD = 2.21) whereas 10 participants formed the Group 2 (2 men and 8 women, age between 70 and 81 years, average age = 73.1, STD = 3.57). We are aware that the populations of both groups are not completely balanced. Other possible criteria of division are possible, such as a median split, obtaining the same number of subjects in both groups. However, in this study, we consider more important that the age ranges are equal, so that it is direct to determine the importance of age in the cognitive training. No significant differences were found in the initial cognitive level for both groups in any of the factors (t-student for independent samples with p values between 0.145 and 0.854).
The local ethics committee approved the study. All the subjects gave their informed consent to participate in the study. The study was carried out at the State Reference Centre for Disability and Dependency (CRE in its Spanish initials), San Andrés del Rabanedo, León (Spain).
Experimental setup
The participants of both groups underwent an initial neuropsychological evaluation test, followed by the cognitive training with BCI and the NeuronUp platform and a final evaluation. The evaluations were carried out using the Luria-DNA neuropsychological battery comprised of nine neuropsychological tests distributed between five different areas. In the area of spoken language, the expression test via expressive and receptive language (through recognition of words, cards, objects and sentence comprehension) was used. The expressive language test evaluated the formulation of discourse, narrative discourse and sentences. In order to evaluate the area of memory, immediate memory (10 words) was used, retaining and evoking in verbal/non-verbal tasks. Logical memorizing was evaluated via the relationships the subjects made. For the evaluation of intellectual processes, a test comprising themed pictures and texts was used in order to analyze comprehension of messages provided via pictures and texts. Discursive and conceptual activity was evaluated via formation of abstract ideas and problem-solving capacity. Finally, for the evaluation of attention-concentration, verbal and non-verbal tasks were used. The neuropsychological profile of each participant was thus established. Each participant used a BCI cap, which translates the subject’s intentions, collected via electrodes in contact with the scalp, into control commands for a device. A portable, 16-channel biomedical signal amplifier with g.tec USB connection (Austria) was used to record the EEG signal. The EEG is needed to provide feedback to the users in real time. Thus, BCI detect the intentions of the users enabling a direct communication between the user and the computer. The reduced dimensions and weight of this device facilitated its portability. The recording equipment was completed with a cap-like device (g.GAMMAcap2SET) on which the electrodes (g.LADYbird) are were placed over specific areas of the cortex. g.GAMMAbox was also used as preamplifier as well as a g.GAMMAconnector. The BCI system detected the correct cerebral pattern in the participant’s cerebral activity using the recorded EEG. If the subject did not achieve the objective, the visual feedback allowed them the possibility to maintain or change their strategy. Additionally, the users also performed activities of the NeuronUp platform.
Each group took part in 10 training sessions: 5 neurofeedback training sessions (NFT) which were alternated with 5 work memory training sessions (WMT). Each NFT session lasted approximately 60 minutes, while each WMT session lasted around 20 minutes. The total duration of the training was 5 weeks, one NFT session and one WMT per week. The NFT session was comprised of 60 trials at different levels of difficulty and the WMT session was comprised of 20 trials. The NFT training tasks had 5 progressive difficulty levels. Additional information of the tasks as well as the trial distribution can be found in the previous study of Gomez-Pilar et al. (2016).
The WMT sessions consisted of memory exercises related to different shapes, colours and expressions.
Statistical analysis
The data was analysed with the IBM SPSS 22 software. In the first instance, it has been analysed whether the factors meet the level of normality using the Shapiro-Wilk test, with all being parametric factors. The homogeneity of Group 1 and Group 2 were proven, and a Chi-square value has been obtained of 4.50 and p-value of 0.034. In order to verify that both groups have a similar level of cognition before the training, statistical differences between groups in the LURIA scores were assessed by means of t-test for independent samples. Non-significant differences were found in the comparison since the t values ranged from –1.149 to 1.407 and the p values between 0.145 and 0.854. A descriptive analysis was carried out and subsequent pre-post intra-group comparison for each of the factors of the battery using the equation t-Student for related samples.
In the Intra-Group analysis of Group 1 (from 60 to 69 years of age), significant differences were observed in the following variables: Visual perception, Spatial orientation, Receptive speech, Expressive speech, Logical memory, Immediate memory, Picture recognition and Concepts (Table 1). Taking into account that in Logical memory, the group does not show a significant improvement in performance after the five training sessions. Among these variables, it is worth noting that in Picture recognition, the average increased 28.18 points and in Visual perception, the improvement was of 16.36 points. In Immediate memory, the improvement was of nearly 8 points (7.95), in spatial orientation of 6.13, in Receptive speech of 5.22 and finally in both Expressive speech and Concepts, the improvement was of 2.95 points. In Logical memory, as was indicated, the group performance declined significantly. The only variable which did not show significant difference was Attention, a factor in which they started with a level of 40.22 and finished with a score of 45.45, noting that the standard deviation both in the pre-test and the post-test was high.
Scores (mean±standard deviation) of the LURIA-AND test for both groups. Within-group statistical differences in each cognitive domain were assessed by means of t-Student test or related samples
Scores (mean±standard deviation) of the LURIA-AND test for both groups. Within-group statistical differences in each cognitive domain were assessed by means of t-Student test or related samples
In the Intra-Group analysis of Group 2 (between 70 and 81 years of age), significant differences were only observed in two of the nine Factors (Table 1). These were specifically significant improvements in Picture recognition and Concepts. In Picture recognition, the improvement was of 29 points and in Concepts, it was seven points. In the variables of Visual perception, Spatial orientation, Receptive speech, Expressive speech, Immediate memory, Logical memory and Attention, there were no significant differences. All these findings are summarized in the Fig. 1. The figure shows a marked increase in several cognitive domains for the Group 1, whereas the Group 2 only show a significant increase in two of the nine Factors.
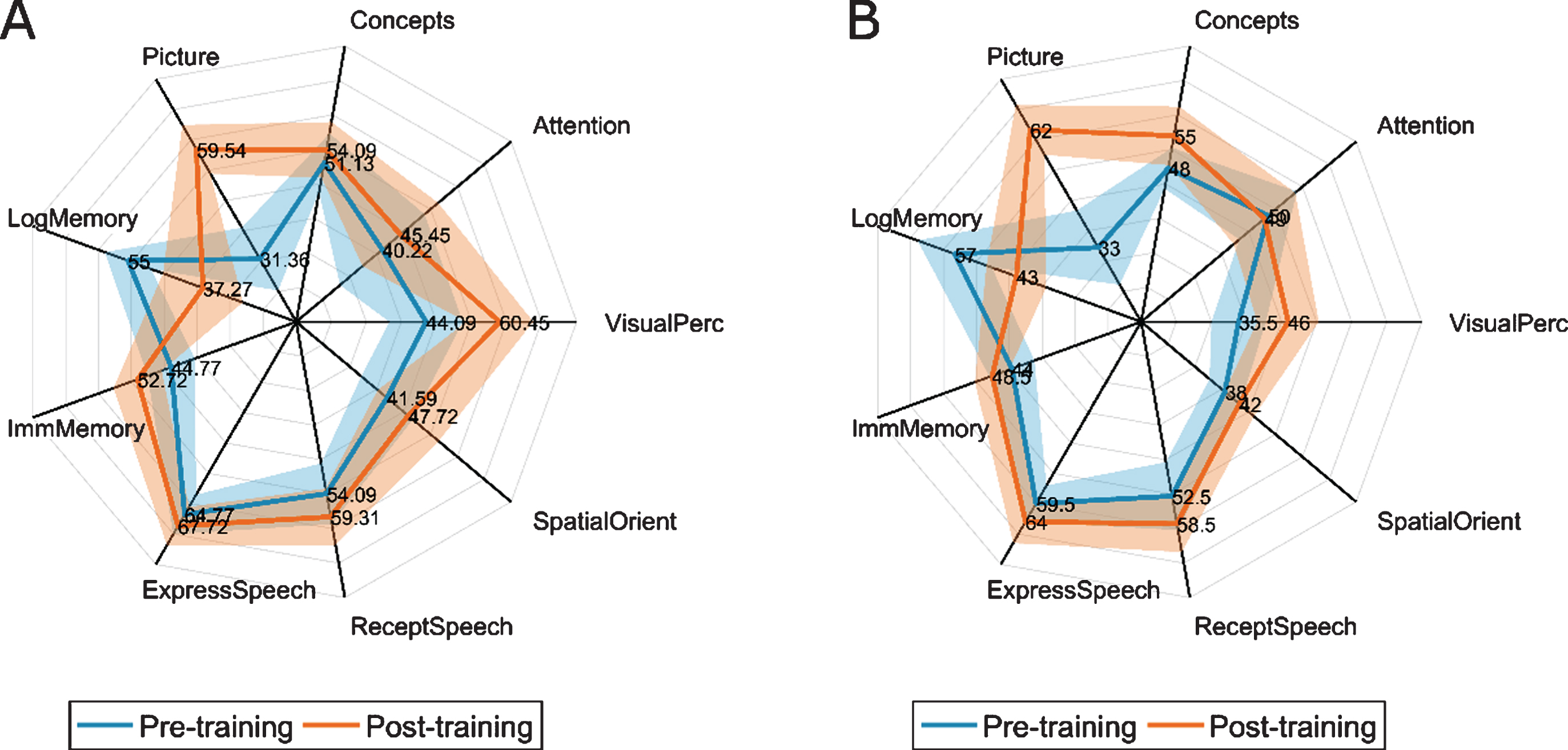
Radial maps of the LURIA-AND scores for Group 1 (A) and Group 2 (B). Standard deviation for each Group and cognitive domain are represented with transparency.
Currently there are different methods for preventing cognitive impairment in individual or group format, with pen and paper or computerized, in which the problem is in the generalization of the benefits (Gutiérrez et al., 2012; Carballo-García et al., 2013; Fernández-Calvo, Rodríguez-Pérez, Contador, Rubio-Santorum & Ramos, 2011). It must be taking into account that computerized tests are not always effective, in line with (Willis et al., 2006; Fernández-Calvo et al., 2011; Dunning & Holmes 2014), since the usual procedure for evaluation consists in standard neuropsychological tests, which measure general cognitive capacity, verbal memory and executive functions, among other faculties, before and after the training process. In addition, the period chosen for evaluating the effects of the training varies.
We confirm that there are studies, which prove the advantages of using programs for neurocognitive training in the prevention of cognitive impairment, like NeuroUp platform (Fernández de Pierola & Sastre, 2015), to improve functional performance of a person and compensate for the resulting cognitive deficits in brain damage in order to reduce functional limitations, increasing the ability of people to perform their daily activities (Carballo-García et al., 2013; Fernández de Pierola & Sastre, 2015; Adams & Victor, 1993; Parkin, 1996; Prigatano, 1999; Sohlberg & Mateer 1989). In this study the final purpose was to improve the quality of life of people. However, it has also proved the usefulness of cognitive training via BCI and NeuroUp platform in a significantly shorter time than the reviewed studies. We also want to highlight that improvements in different neuropsychological aspects in elderly subjects with cognitive impairment have been achieved in a reduced timeframe (5 weeks). In the pre-post of each factor, Group 1 obtained highly significant improvements in Picture recognition, Visual perception, immediate memory, Spatial orientation, Receptive speech, Expressive speech and Concepts in comparison with Group 2, which only obtained significant improvements in Picture recognition and Concepts. Group 1 does not obtain an improvement in Logical memory. The reason could be linked to the low scores in the cognitive areas related to memory that MCI patients usually obtain. Memory, in turn, is connected to the Attention factor, in which no differences were found in this study, perhaps due to the characteristics of the subjects (Nilton et al., 2012; Bahar-Fuchs et al., 2013; Bahar-Fuchs et al., 2009; Andrade & Radhakrishnan, 2001; Donoso, Venegas, Villarroel, Vásquez, 2001).
The training with NeuroUp platform for MCI between 18 and 23 in the MMSE is beneficial for people between 60 and 80 years of age. It was suggested that cognitive training in tasks related to daily life generates more significant changes than those focused only on memory. It is especially useful to increase neuronal plasticity of the patients, improve their autonomy and gain independence in their daily life (Gutiérrez et al., 2012; Carballo-García et al., 2013; Gates et al., 2011). Comparing the benefits of cognitive training among the two age groups (under 70 against over 70), we have discovered that cognitive training is much more beneficial for people between 60 and 70 years of age than for people between 70 and 80 (remembering that both groups started from the same base level in each of the factors). Given that the cognitive ageing of the society is evident (Snyder et al., 2011; Solé-Padullés et al., 2007), these findings suggest that the age between 60 and 70 years is a key time for working on cognitive training focusing on preventing, stabilizing or slowing down cognitive impairment. Thus, dementia could obtain cognitive improvements in a range of ages between 60–70 in a significantly short time.
Some issues of this research merit further consideration. Firstly, the sample size is small and the groups are not completely balanced. For this reason, larger populations, especially for the Group 2, should be analyzed in the future. Additionally, we followed a quasi-experimental approach in this study. However, the inclusion in the future of a control group could be helpful to reinforce the conclusions of the current study.
Conclusion
1. The proposed program of cognitive training, serves as a method for preventing, stabilizing or slowing down cognitive impairment in a short time in people between 60 and 70 years old.
2. Performing a program which includes activities of Visual perception, Spatial orientation, Expressive and receptive speech, Immediate and logical memory, Picture recognition and Concepts, applied to daily life, leads to an improvement in neuronal plasticity and provides greater autonomy and independence for the subject in their life.
3. The NeuroUp platform, together with the BCI, opens a new line of work and research with the aim of preventing cognitive impairment in people with MCI, improving their quality of life.
Footnotes
Acknowledgments
This research project was supported in part by “Ministerio de Economía y Competitividad” and FEDER under project TEC2014-53196-R, by ‘European Commission’ (POCTEP 0378_AD_EEGWA_2_P), and by ‘Consejería de Educación de la Junta de Castilla y León’ (VA037U16). J. Gomez-Pilar was in receipt of a grant from University of Valladolid.
We thank the managers for their support in carrying out this study, and the people for accepting to participate in this research.