
Abstract
Background:
Preliminary evidence showed additional effects of anodal transcranial direct current stimulation over the damaged cerebral hemisphere combined with cathodal transcutaneous spinal direct current stimulation during robot-assisted gait training in chronic stroke patients. This is consistent with the neural organization of locomotion involving cortical and spinal control. The cerebellum is crucial for locomotor control, in particular for avoidance of obstacles, and adaptation to novel conditions during walking. Despite its key role in gait control, to date the effects of transcranial direct current stimulation of the cerebellum have not been investigated on brain stroke patients treated with robot-assisted gait training.
Objective:
To evaluate the effects of cerebellar transcranial direct current stimulation combined with transcutaneous spinal direct current stimulation on robot-assisted gait training in patients with chronic brain stroke.
Methods:
After balanced randomization, 20 chronic stroke patients received ten, 20-minute robot-assisted gait training sessions (five days a week, for two consecutive weeks) combined with central nervous system stimulation. Group 1 underwent on-line cathodal transcranial direct current stimulation over the contralesional cerebellar hemisphere + cathodal transcutaneous spinal direct current stimulation. Group 2 received on-line anodal transcranial direct current stimulation over the damaged cerebral hemisphere + cathodal transcutaneous spinal direct current stimulation. The primary outcome was the 6-minute walk test performed before, after, and at follow-up at 2 and 4 weeks post-treatment.
Results:
The significant differences in the 6-minute walk test noted between groups at the first post-treatment evaluation (p = 0.041) were not maintained at either the 2-week (P = 0.650) or the 4-week (P = 0.545) follow-up evaluations.
Conclusion:
Our preliminary findings support the hypothesis that cathodal transcranial direct current stimulation over the contralesional cerebellar hemisphere in combination with cathodal transcutaneous spinal direct current stimulation might be useful to boost the effects of robot-assisted gait training in chronic brain stroke patients with walking impairment.
Introduction
Stroke is a leading cause of adult disability (Smania et al., 2009; Benjamin et al., 2017). Current best practice in stroke management aims to reduce the initial impact of brain damage, take precautions to avoid further burden of complications, and maximize functional recovery through extensive rehabilitation treatment (Di Pino et al., 2014; Picelli et al., 2014). Neuronal reorganization and plasticity begin in the very early stages after stroke and continue for several weeks also in brain regions distant to the affected site (Takeuchi & Izumi, 2012). Non- invasive brain stimulation (NIBS) is used to modulate the excitability of neuronal circuits and improve post- stroke functional recovery by altering synaptic efficacy in glutamatergic and γ-aminobutyric acid-mediated circuits (Di Lazzaro et al., 2012). Among NIBS techniques, transcranial direct current stimulation (tDCS) is used to deliver a weak polarizing current to a neuronal population and modulate its excitability by polarity-specific effect: cathodal stimulation is reported to reduce neuronal excitability by inducing hyperpolarization, while anodal stimulation increases neuronal excitability and leads to depolarization (Nitsche at al., 2000; Jayaram et al., 2009; Lefaucheur, 2009; Elsner et al., 2013).
Locomotion is a purposeful, goal-directed behavior initiated by signals that arise from volitional processing in the cerebral cortex or emotional processing in the limbic system. It is sustained by basic locomotor patterns generated by spinal interneuronal networks called central pattern generator (CPG) circuits (Dietz, 2002; Pisotta & Molinari, 2014). Robot-assisted gait training (RAGT) has been reported to effectively improve locomotion ability in stroke patients even during the chronic phase of illness (Mehrholz et al., 2007; Geroin et al., 2013; Mehrholz et al., 2013; Mehrholz et al., 2017; Morone et al., 2017). Recent preliminary evidence supports the hypothesis that cerebral stimulation (tDCS), when combined with transcutaneous spinal direct current stimulation (tsDCS), may actually enhance the effects of RAGT in chronic stroke patients (Picelli et al., 2015). This is consistent with the notion of a complex neural organization of locomotor control mechanisms involving some supraspinal structures in addition to the CPG circuits (Dietz, 2002; Geroin et al., 2011; Takakusaki, 2013). In this network of spinal, subcortical, and cortical controls, the cerebellum is an important contributor to feedforward control mechanisms crucial for avoiding obstacles and adapting to novel conditions (Pisotta & Molinari, 2014). In particular, the cerebellum has been reported to influence M1 activity through the cerebellar- thalamo-cortical pathway, whose activation state relates to mechanisms of locomotor adaptation (Bostan et al., 2013). Changes in cerebellar excitability were found to strongly correlate with the magnitude of behavioral adaptation during walking in healthy subjects and chronic stroke patients (Reisman et al. 2007; Reisman et al. 2009; Reisman et al. 2010; Jayaram et al. 2011).
On this basis, and according to the concepts about locomotor control described so far, there is a rationale for the modulation of cerebellar and spinal activity in combination with RAGT to improve gait ability after stroke. To the best of our knowledge, despite its key role in gait control, the effect of transcranial direct current stimulation of the cerebellum (tcDCS) on brain stroke patients treated with RAGT has not been previously investigated (Priori et al., 2014). Thus, the main aim of this pilot study was to compare the effects of cathodal cerebellar stimulation (tcDCS) + cathodal spinal stimulation (tsDCS) versus anodal cerebral stimulation (tDCS) + cathodal spinal stimulation (tsDCS) on RAGT in patients with chronic brain stroke as measured by changes in walking distance on the 6-Minute Walk Test (6MWT). The secondary aim was to compare the effects of the above- mentioned stimulation protocols on RAGT as measured by improvements in locomotion ability, spatiotemporal gait parameters, affected lower limb motricity, and spasticity in these patients.
Methods
For this single center, single blind, randomized controlled trial, the inclusion criteria were: age greater than 18 years; first-ever unilateral ischemic brain stroke (as documented by computerized tomography scan or magnetic resonance imaging); at least 6 months since stroke onset; no botulinum toxin injection into the affected leg muscles or rehabilitation treatment in the 6 months before recruitment; Mini Mental State Examination score >24 (Folstein et al., 1975). Exclusion criteria were: participation in other trials; history of epileptic fits; electroencephalography (EEG) suggesting increased cortical excitability; metallic brain or spinal implants; previous cranial or spine surgery; medications altering central nervous system (CNS) excitability (e.g., antiepileptics, neuroleptics, benzodiazepines or antidepressants) or with a presumed effect on CNS plasticity (i.e., dopamine, fluoxetine or D-amphetamine); deficits of somatic sensation involving the lower limbs (assessed by physical and neurological examination); posterior circulation stroke; vestibular disorders or paroxysmal vertigo; other neurological or orthopedic conditions involving the lower limbs (musculoskeletal diseases, severe osteoarthritis, peripheral neuropathy, joint replacement); cardiovascular co-morbidity (recent myocardial infarction, heart failure, uncontrolled hypertension, orthostatic hypotension).
All participants were outpatients and gave their informed, written consent to participate in the study, which was carried out according to the tenets of the Declaration of Helsinki and approved by the local Ethics Committee. Prior to testing, eligible participants were randomly assigned in a one-to-one ratio to two arms: Group 1 received cathodal cerebellar stimulation (tcDCS) + cathodal spinal stimulation (tsDCS); Group 2 underwent anodal cerebral stimulation (tDCS) + cathodal spinal stimulation (tsDCS). The patients were allocated to one of the two treatment arms according to a balanced (restricted) software-generated randomization scheme. When the decision was made, the investigator (E.C.), who determined whether a subject was eligible for inclusion in the trial, was unaware of which group the subject would be allocated to (allocation was by sealed opaque envelopes). Another investigator (M.F.) checked for correct patient allocation according to the randomization list. After unmasking at the end of the study, we made sure that no errors in allocation had been made. During the study, participants did not undergo any form of physical therapy other than that scheduled under the study protocol.
Treatment procedures
Robot-assisted gait training
The RAGT program consisted of ten, 20-minute sessions, five days a week (from Monday to Friday) for two consecutive weeks, carried out on a G-EO System Evolution (Reha Technology, Olten, Switzerland). The system is composed of an end-effector device with body weight support and footplates attached to a double crank and a rocker gear system with three degrees of freedom each that allows control of step length and height (Hesse et al., 2012, Picelli et al., 2015). The step length of each patient was evaluated with the GAITRite system (CIR Systems, Havertown, PA, USA) and individually defined (Kuys et al., 2011). Each training session consisted of two parts. First, patients were trained at 10% of body weight supported and 1.5 km/h for 10 minutes and then at 0% of body weight supported at 2.0 km/h for 10 minutes. Before each RAGT session, 4 electrodes were placed on the patient (2 on the scalp and 2 on the back) and connected to a multichannel current stimulator (Starstim®, Neuroelectrics, Barcelona, Spain).
Cathodal tcDCS applied over the contralesional cerebellar hemisphere
Two identical circular, saline-soaked electrodes (diameter 4 cm; 12.56 cm2) were placed and secured on the scalp. The cathode was positioned over the contralesional cerebellar hemisphere following the 10–20 international EEG system (O1 or O2 position) and the anode was placed over the buccinator muscle on the same side (Ferrucci et al., 2015). The intensity of stimulation was set at 2 mA and applied for 20 minutes during RAGT (on-line stimulation). As to the rationale of this stimulation paradigm, we have to remember that one of the main outputs of the cerebellum is the dentate-thalamo-cortical pathway. In particular, Purkinje cells (the output neurons of the cerebellar cortex) have inhibitory connections with the dentate cerebellar nucleus, which in turn has a disynaptic excitatory connection through the ventral thalamus to contralateral M1 (Middleton & Strick, 2000; Kelly & Strick, 2003). Thus, Purkinje cell activity exerts an inhibitory tone over the contralateral M1 (cerebello-brain inhibition). In this study the cathode (stimulating electrode) was placed over the contralesional cerebellar hemisphere in order to decrease the inhibitory tone exerted by the cerebellum over the lesioned M1, according to the polarity specific-effect of tcDCS previously reported in literature (Galea et al., 2009). On the same line, the return electrode (anode) was placed over the ipsilateral buccinator muscle in order to avoid current spreading (i.e. to the brachial plexus) (Galea et al., 2009; Ferrucci et al., 2015). The rationale for on-line tcDCS was based on previous literature about this type of application as an intervention to speed up motor skill improvement, which reported that cerebellar stimulation could facilitate motor skill acquisition by increasing on-line rather than off-line learning (Cantarero et al, 2015).
Anodal tDCS applied over the damaged cerebral hemisphere
Two identical circular, saline-soaked electrodes (diameter 4 cm; 12.56 cm2) were placed and secured on the scalp. The anode was positioned over the lesioned primary motor cortex (M1), on the leg representation area (Pfurtscheller et al., 2000), following the 10–20 international EEG system (Cz position), and the cathode was placed above the orbit on the other side (Roche et al., 2012; Cha et al., 2014). The intensity of stimulation was set at 2 mA and applied for 20 minutes during RAGT (on-line stimulation).
Cathodal tsDCS
A pair of circular, saline-soaked self-adhesive electrodes (diameter 5.5 cm; 23.75 cm2) was positioned on the patient’s back. The cathode was placed over the spinous process of the tenth thoracic vertebra (from ninth to eleventh) and the anode was placed above the shoulder of the unaffected hemibody (Bocci et al., 2014; Picelli et al., 2015). The intensity of stimulation was set at 2.5 mA and applied for 20 minutes during RAGT (on-line stimulation).
Evaluation procedures
Patients were evaluated before treatment (T0), immediately after treatment (primary endpoint) (T1), at 2 weeks (T2) and 4 weeks (T3) of follow-up. The same rater (P.C.), who was blinded to group allocation, evaluated all patients. Asking the assessor to make an educated guess tested the success of blinding.
Primary outcome
The primary outcome was the 6MWT, which was selected as a measure of walking capacity. The patients were asked to cover as much ground as possible within 6 minutes (walking continuously at their fastest speed) along a marked distance (1 lap, 40 m). The distance covered was then recorded (Enright, 2003).
Secondary outcomes
The Functional Ambulation Category (FAC) was used to classify locomotion ability. Scores range from 0 (patient cannot walk or needs help from two or more persons) to 5 (patient can walk independently anywhere) (Holden et al., 1986). The Motricity Index leg sub-score (MI) was used to assess the strength of the affected lower limb. The leg subtest score ranges from 1 (complete paralysis) to 100 (normal strength) (Demeurisse et al., 1980). The Ashworth scale (AS) was used to test the muscle tone of the affected lower limb (ankle plantar flexors) (Ashworth, 1964). This validated scale grades the resistance of a relaxed limb to rapid passive stretching in 5 stages (range 0–4; 0 indicates no increase in muscle tone; 4 indicates joint rigidity). Spatiotemporal gait parameters were evaluated with the GAITRite system (CIR Systems Inc) (Kuys et al., 2011). To avoid acceleration and deceleration, the patients were asked to ambulate along the 7.66-m GAITRite walkway on a 12- m course. The data from three trials were collected and their average calculated. Cadence and ratio between single and double support duration were evaluated.
Statistical analysis
We assessed all patients who were randomized (intention-to-treat principle). The Mann-Whitney U-test was used to assess the homogeneity of the two groups at baseline and to analyze changes in performance at the evaluation sessions and the effect of treatment between groups. For this purpose, we computed the differences in performance between T1 and T0 (T1-T0), between T2 and T0 (T2-T0), and between T3 and T0 (T3-T0) for all outcome measures. Within-group comparisons (T1 vs. T0; T2 vs. T0; T3 vs. T0) were performed with the Wilcoxon signed-rank test for all outcomes. Descriptive analysis was used to evaluate the effect size measures (Cohen’s d calculation) and the 95% confidence intervals (Cohen, 1988). The alpha level for significance was set at P < 0.05. Bonferroni correction was used when investigating multiple within-group comparisons, resulting in P < 0.016 as the significance threshold (Benjamini et al., 1995). Statistical analysis was carried out using the Statistical Package for Social Science for Macintosh, version 20.0 (IBM SPSS Inc, Armonk, NY, USA).
Results
Twenty subjects (13 men and 7 women; mean age 62.7 years) presenting with chronic brain stroke (mean time since onset 4.9 years) were recruited from among 36 outpatients attending our research center. The enrolment period was from October 2015 to May 2016. Ten patients were allocated to each treatment group. No dropouts or adverse events were recorded during the trial in either group. The study flow is shown in Fig. 1.
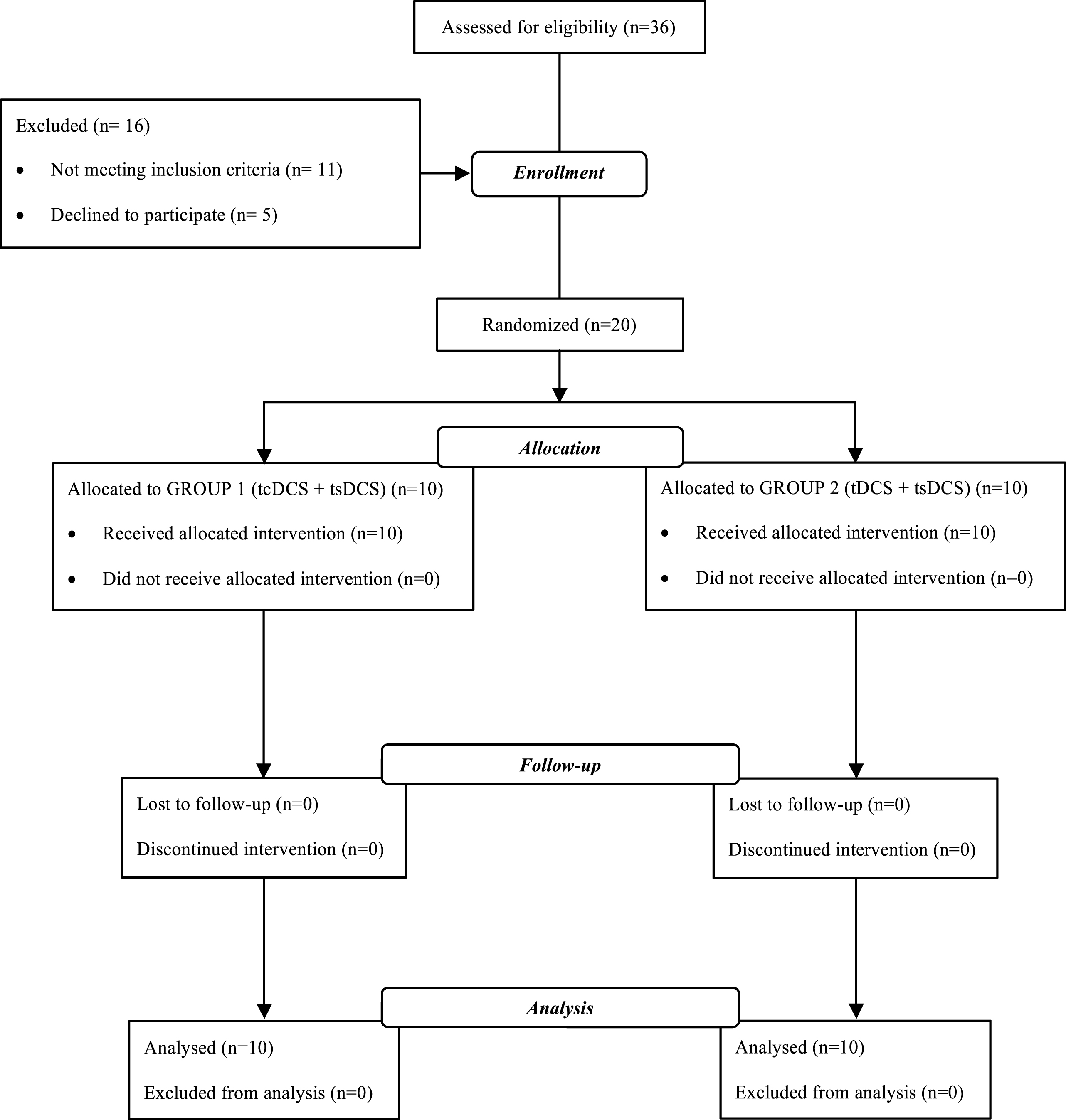
Study flow.
No significant difference between the two groups was observed for age and length of illness (Table 1) or for any of the following outcomes at baseline evaluation: 6MWT (P = 0.650); FAC (P = 0.490); MI (P = 0.761); MAS (P = 0.119); cadence (P = 0.131); ratio between single and double support duration (P = 0.596). Table 1 presents the patients’ demographic and clinical features.
Demographic and clinical features of patients
Demographic and clinical features of patients
Abbreviations: tcDCS, transcranial cerebellar Direct Current Stimulation; tsDCS, transcutaneous spinal Direct Current Stimulation; tDCS, transcranial Direct Current Stimulation; SD, Standard Deviation; n, number of patients.
Significant differences in 6MWT between the two groups were found at T1–T0 (P = 0.041; Z = –2.043; effect size 0.43). No significant difference between groups was found at T2–T0 (P = 0.650; Z = –0.454; effect size 0.10) and T3–T0 (P = 0.545; Z = –0.606; effect size 0.36). Group data and within-group comparisons are reported in Table 2.
Within-group comparisons of treatment effects on all outcome measures
Within-group comparisons of treatment effects on all outcome measures
Abbreviations: 6MWT, 6-minute walk test; FAC, Functional Ambulation Category; MI, Motricity Index; AS, Ashworth scale; S/D, Single/Double; m, meters; cyc/min, cycles/minute; IQR, Inter Quartile Range; SD, Standard Deviation; CI, Confidence Interval. *=statistically significant after Bonferroni correction (P < 0.016).
No significant difference in FAC between the groups was found at T1–T0 (P = 1.000; Z = 0.000; effect size not calculable), T2–T0 (P = 1.000; Z = 0.000; effect size not calculable), and T3–T0 (P = 0.317; Z = –1.000; effect size 0.22). Significant differences in MI between the groups were found at T1–T0 (P = 0.017; Z = –2.396; effect size 0.51), T2–T0 (P = 0.045; Z = –2.000; effect size 0.44) and T3–T0 (P = 0.008; Z = –2.669; effect size 0.62). No significant difference in MAS between the groups was found at T1–T0 (P = 0.210; Z = –1.255; effect size –0.30), T2–T0 (P = 0.251; Z = –1.147; effect size –0.21), and T3–T0 (P = 0.644; Z = –0.463; effect size –0.06). Significant differences in cadence between the groups were found at T1–T0 (P = 0.019; Z = –2.348; effect size 0.46). No significant difference between the groups was found at T2–T0 (P = 0.650; Z = –0.454; effect size –0.23) and T3–T0 (P = 0.545; Z = –0.606; effect size –0.10). No significant difference in the ratio between single and double support duration between the groups was found at T1–T0 (P = 0.472; Z = –0.720; effect size –0.22), T2–T0 (P = 0.212; Z = –1.248; effect size –0.21), and T3–T0 (P = 0.075; Z = –1.783; effect size –0.41). Group data and within-group comparisons are reported in Table 2.
Discussion
The aim of this pilot study was to compare the effects of cathodal cerebellar stimulation (tcDCS) + cathodal spinal stimulation (tsDCS) versus anodal cerebral stimulation (tDCS) + cathodal spinal stimulation (tsDCS) on RAGT in patients with chronic brain stroke. Our findings showed a significantly greater improvement as to walking capacity (measured by the 6MWT) in Group 1 (cathodal cerebellar stimulation + cathodal spinal stimulation) patients than the Group 2 (anodal cerebral stimulation + cathodal spinal stimulation) patients at the first post-treatment evaluation (T1–T0); however, these improvements were not maintained at the subsequent follow-up evaluations (T2–T0 and T3–T0). Accordingly, we observed a significantly greater improvement in gait cadence at the post-treatment evaluation (not maintained at the subsequent follow-up evaluations) in the patients who received cathodal cerebellar stimulation + cathodal spinal stimulation (Group 1 patients). Furthermore, with regards to secondary outcomes, we found a significantly greater improvement as to the affected lower limb motricity (measured by the MI) at each time point in Group 1 patients (cathodal cerebellar stimulation + cathodal spinal stimulation).
Since all patients underwent the same protocols of spinal stimulation and RAGT, the significant differences found between groups after treatment are to be ascribed to the effects of cerebral and cerebellar stimulation. Some issues about NIBS need to be considered in order to correctly interpret our results. First, several models of brain functional reorganization have been described in the literature (Di Pino et al., 2014). For instance, according to the vicariation model, post-stroke functional recovery has been reported to occur through the activity of residual networks that substitutes (presumably via the intact unaffected hemisphere) those functions lost in damaged areas (Aminoff et al., 2009). Alternatively, the interhemispheric competition model assumes the presence of a mutual, balanced, transcallosal inhibition between hemispheres in healthy people. This model suggests that damage to one hemisphere in stroke disrupts this balance, leading to reduced inhibition of the unaffected hemisphere by the affected one, which results in increased inhibition of the affected hemisphere by the unaffected one, further contributing to motor impairment and suppression of recovery of the ipsilesional motor cortex after stroke (Traversa et al., 1998; Duque et al., 2007; Jayaram et al., 2009). More recently, the bimodal balance recovery-model has been advanced to combine the vicariation and the interhemispheric competition models by introducing the concept of structural reserve, which describes the extent to which neural pathways and relays spared by the lesion contribute to recovery. This model of post-stroke functional recovery suggests that the amount of structural reserve determines whether interhemispheric imbalance dominates over vicariation and that the interhemispheric competition model underlies motor recovery in stroke patients with high functional reserve (Di Pino et al., 2014).
Second, we have to take into account the role of the cerebellum, which is known to be essential for adaptive learning mechanisms that contribute to a broad range of behaviors, including walking (Reisman et al. 2005; Jayaram et al., 2012; Picelli et al., 2017). The activity of Purkinje cells leads to cerebello-brain inhibition by exerting an inhibitory tone over the contralateral M1 through the dentate-thalamo-cortical pathway, which is one of the main outputs of the cerebellum (Middleton & Strick, 2000; Kelly & Strick, 2003; Galea et al., 2009). According to the characteristics of our sample of chronic brain stroke patients, we argue that the interhemispheric competition model had greater relevance to the present pilot study (Di Pino et al., 2014; Picelli et al., 2015). Thus, we compared two different strategies for restoring, as far as possible, a balanced activity between hemispheres by stimulating the affected M1 directly (anodal tDCS applied over the damaged cerebral hemisphere) or indirectly through the dentate-thalamo-cortical pathway (cathodal tcDCS applied over the contralesional cerebellar hemisphere). Our findings support the hypothesis that modulating activation of the cerebellar (dentate nucleus) thalamo-cortical pathway by means of cathodal stimulation over the contralesional cerebellar hemisphere might be the more effective strategy to boost the effect on RAGT in combination with cathodal spinal stimulation in patients with chronic ischemic stroke. Methodologically, this was probably reasonable because stimulating an unaffected structure, such as the cerebellum, might better induce cortical currents than an affected one, such as a damaged M1. On the same line, previous literature found that changes in electrical properties at stroke boundaries might have an impact on stimulation outcome according to an altered distribution of currents in magnitude, location, and orientation (O’Brien et al., 2016). In particular, cerebral stimulation protocols appeared to be less efficient in head models of chronic stroke patients, according to the influence of stroke lesion on the electric fields generated by tDCS in cortical grey matter, which showed a decreased strength in comparison to healthy controls (Manoli et al., 2017; Minjoli et al., 2017).
In keeping with the thoughts just expressed, previous literature about robotic training combined with NIBS delivered on the affected hemisphere of chronic stroke patients showed no significant difference between real and sham-stimulation as to post-treatment clinical gains, probably because in patients with severe brain damage, it might be less useful to manipulate the excitability of the affected hemisphere in terms of promoting relearning from rehabilitation (Di Lazzaro et al., 2016). Conversely, in these patients, might be more helpful to target stimulation on unaffected structures in order to obtain a more relevant recovery (Di Pino et al., 2014; Di Lazzaro et al., 2016). Thus, stimulation of the cerebellum not only as a target to indirectly modulate the affected M1 activity but also as a key component of locomotor control needs to be considered. Indeed, decreased activation of the cerebellar (dentate nucleus) thalamo-cortical pathway has been reported to be related to the processes of locomotor adaptation and storing of new locomotion patterns (Ugawa et al., 1995; Middleton & Strick, 1999; Pinto & Chen 2001; Daskalakis et al. 2004; Reis et al. 2008; Jayaram et al., 2011). We believe this might have led to the long-lasting effects on the affected lower limb motricity observed in Group 1 (cerebellar + spinal stimulation) at all assessments, also opening several interesting future perspectives for daily clinical practice. Indeed, lower limb motricity is a main contributor to gait ability, which has been shown to be greater in community ambulation stroke patients than in limited community ambulation ones (Lee et al., 2015). On this basis, we hypothesize that increasing the intensity of RAGT or combining it with a protocol of overground exercises might translate to a long-term increase in walking ability, given the greater long-lasting improvement of the affected lower limb motricity we found in Group 1 (cerebellar + spinal stimulation) patients. Future studies are needed to investigate and substantiate this hypothesis.
Finally, no adverse events or dropouts were recorded during the study. Moreover, as to the primary outcome and spatiotemporal gait parameters, we found no non-responders (both patient groups showed within-group improvements after stimulation) (see also Table 2). This is in line with previous observations and further confirms the safety of direct current stimulation procedures (Bikson et al., 2016).
This pilot study has several limitations. First, the sample size was small. We estimated that a total of 50 subjects (25 patients per group) would provide 90% power to detect a difference of 50 meters on the 6MWT between the groups (Perera et al., 2006). This may have hindered some long-term combined effects of cerebellar stimulation (tcDCS) and spinal stimulation (tsDCS) on RAGT in our patients. Second, no neurophysiological assessment (e.g. motor-evoked potentials or H-reflex) was done. Third, long-term (more than 1 month) follow-up was not conducted. Fourth, no comparison was done with other non-invasive stimulation techniques, such as transcranial magnetic stimulation. Fifth, because we included only patients with chronic ischemic stroke, we cannot draw conclusions about the effects of the current protocols of NIBS on RAGT in patients with acute or sub-acute stroke or in those with hemorrhagic brain stroke or cerebellar stroke. Nonetheless, our preliminary findings support the hypothesis that cathodal stimulation of the contralesional cerebellar hemisphere (tcDCS) in combination with cathodal spinal stimulation (tsDCS) might be a useful tool to improve the effects of RAGT in patients with chronic ischemic brain stroke. Future properly-sized randomized controlled are needed to further validate our findings.
Footnotes
Acknowledgments
None.