
Abstract
Background:
Specific investigation of dual task-interference (DTI) may help researchers to develop the optimal training exercise for enhancing the performance of daily activities.
Objectives:
To reveal the DTI by comparing the performances between personalized single tasks (cognitive or motor task) and dual task with serial decomposition in normal healthy adults.
Methods:
After a preliminary period, healthy participants randomly (n = 46) performed three computerized experiments of cognitive (CT), motor (MT) and dual tasks (DT). In CT, participants were required to release button 1 (BT1) as rapidly as possible when the font color of a word and its meaning were congruent (Go), and in MT, they had to release BT1 and then tap button 2 (BT2) 10 times as rapidly as possible if the symbol “○” was presented (Go). The DT consisted of a combination of CT and MT elements. The reaction time (RT) of correct releases (RTCR) of BT1 in all tasks was measured, as well as the button shifting time between releasing BT1 and pressing BT2, and the finger tapping rate in MT and DT. To obtain the DTI values, we calculated the RTCR ratio in CT and MT and divided the outcome by the RTCR of DT.
Results:
The ratio of RTCR in CT (% CT/DT, 78.6±13.0%) and MT (% MT/DT, 74.2±10.1%) were significantly lower than the ratio of RTCR in DT (% DT/DT, 100%). The button shifting time of MT was at 92.0±23.7% of baseline, and the finger tapping rate of MT was 106.1±19.1%, which was significantly higher than baseline.
Conclusions:
The % DT/DT is significantly higher than both % CT/DT and % MT/DT, which suggests that the cognitive load depends on the type of cognitive task that is being performed. Additionally, the significant increase of % DT/DT compared to % CT/DT indicated that there is a cognitive load prior to a motor task. The increased button shifting time and decreased tapping rate in DT may indicate that a residual cognitive load and a concurrent motor load were present.
Introduction
Typical daily activities, such as walking and driving simultaneously require cognitive and motor functions and are thus called dual tasks (DT) (Sethi & Raja, 2012). When evaluating an individual’s performance of daily activities, the motor and cognitive functions are usually assessed separately. However, performing daily DT does not only lead to motor dysfunction in the long-run, but also to dysfunctional cognitive processes such as memory, attention, and executive processes (Klotzbier & Schott, 2017). Therefore, it is crucial to understand the roles of both motor and cognitive processes in DT in order to enhance an individual’s performance of a daily activity.
Previous studies of DT interference (DTI), which refers to an impaired performance when performing two tasks simultaneously, has been observed in healthy subjects (Lu, Liu, Yang, Wu, & Wang, 2015), as well as patients with stroke (Yang, Lam, Huang, He, & Pang, 2017), mild cognitive impairment (Klotzbier & Schott, 2017), multiple sclerosis (Malcay, Grinberg, Berkowitz, Hershkovitz, & Kalron, 2017), Huntington’s disease (Kloos et al., 2017), and Parkinson’s and Alzheimer’s disease (Christofoletti, Andrade, Beinotti, & Borges, 2014). Screening for DTI in healthy individuals may enable the early detection of functional deterioration caused by the aging process or neurodegenerative diseases.
So far, to study the motor component of DTI the function of the lower extremities were assessed by observing behaviors, such as the gait (Kloos et al., 2017; Klotzbier & Schott, 2017; Yang, Lam, Huang, He, & Pang, 2017) or balance of an individual (Ghai, Ghai, & Effenberg, 2017). However, the motor functions of upper limbs have not been extensively studied, though they play an important role in daily activities. Assessing the DTI in hand motor function may be important in discovering the functional processes involved in daily activities. Moreover, the traditional method for evaluating DTI was to calculate the ratio of the difference between dual task RT and single task RT and divide the outcome by the single task RT (Plummer & Eskes, 2015). However, this method did not assess the role of cognitive and motor tasks separately and therefore did not identify how these specifically play a role in DTI. A better understanding of the effect of both cognitive and motor tasks on DTI will help researchers develop optimal training exercises for individuals that will help to enhance their performance of daily activities. Therefore, because DTI of hand function may hinder the performance of daily activities, the purpose of this study was to discover the interference pattern in upper limb motor function during DT in healthy subjects.
Methods
Participants
Healthy farmers from the Gangwon province of South Korea were recruited from November 2017 to January 2018. Initially, 61 participants were screened; 8 participants were excluded because they were diagnosed with stroke (n = 4), dementia (n = 2), or they were left-handed (n = 2). Further, 7 were excluded due to having performed poorly in the tasks. Then, those with diagnosed and/or medicated cancer, stroke, dementia, and depression were excluded, and those who performed poorly during challenging tasks were also excluded (Fig. 1). Finally, a total of 46 participants (age 60.7±4.7 years, 32 female farmers) were included in the analysis (Feb.).
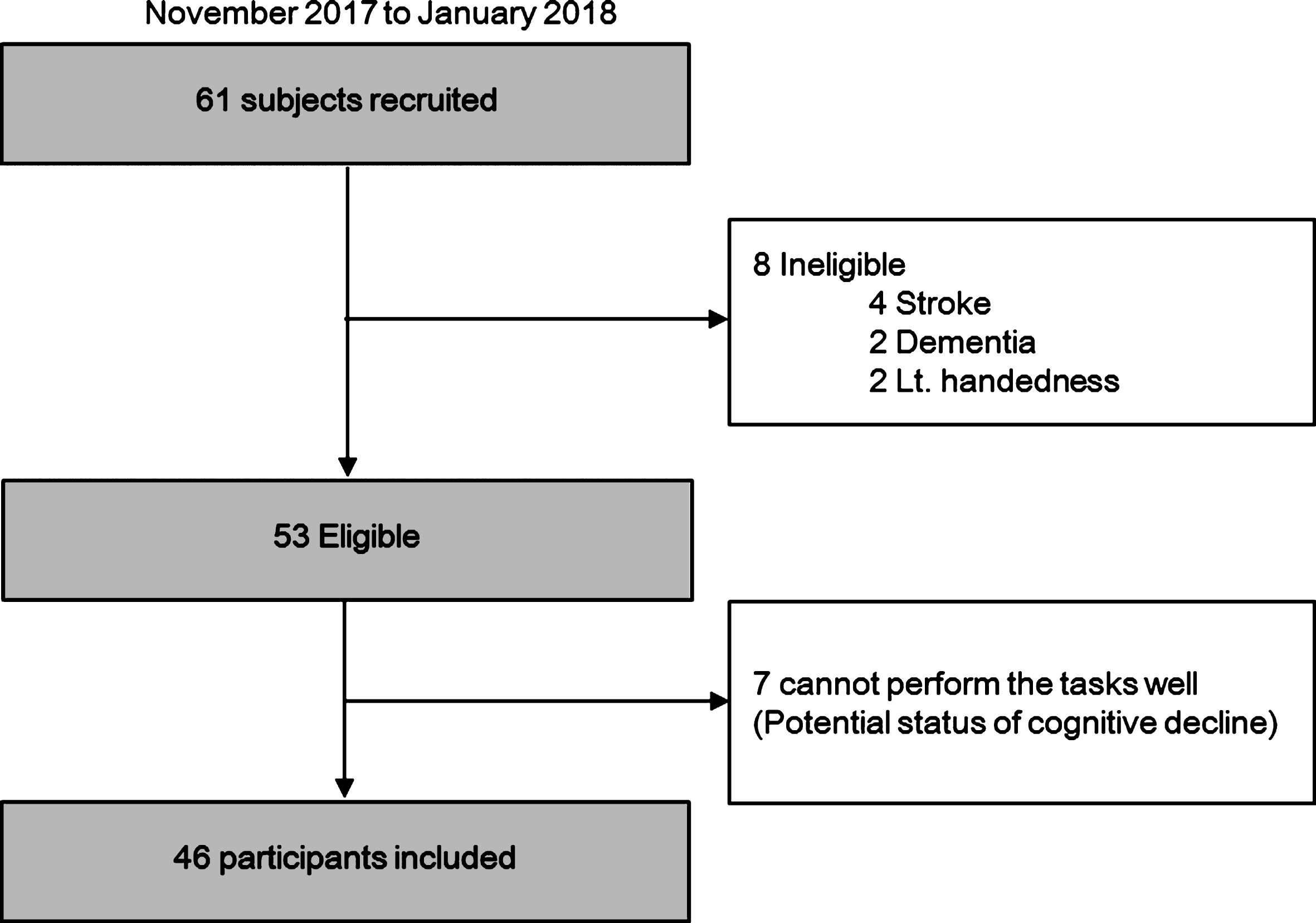
A flow chart summarizing the recruitment process.
Subsequently, we assessed the subjects’ sex, age (years), body mass index (BMI, kg/m2), grip strength using a Lavisen electronic hand grip dynamometer KS 301 (Lavisen Co. Ltd., Namyangju, Korea), physical function using the Short Physical Performance Battery (SPPB) test (Gawel et al., 2012), and the following two scores: 1) Korean version of the Mini-Mental State Examination (MMSE-KC) from the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) score (Lee et al., 2004), and 2) Korean Version of the Beck Depression Inventory (K-BDI) score (Han, Yeom, & Shin, 1986).
This study was approved by the Institutional Review Board of the Kangwon National University Hospital (IRB No. 2017-04-017-006) and written consent was obtained from all the participants. Additionally, this study is registered at the Clinical Research Information Service (CRIS, http://cris.nih.go.kr), number KCT0002366.
Figure 2 shows the DTI experimental protocol that was used in the study. Three computerized experiments (a cognitive, a motor, and a dual task) were randomly performed by participants after a brief preparation period (Superlab pro v.4.0 software, Cedrus Corporation, San Pedro, CA). The two different instructions (pressing or releasing the buttons) in each trial were also randomized. All participants practiced pressing button 1 (BT1) during the preliminary period.
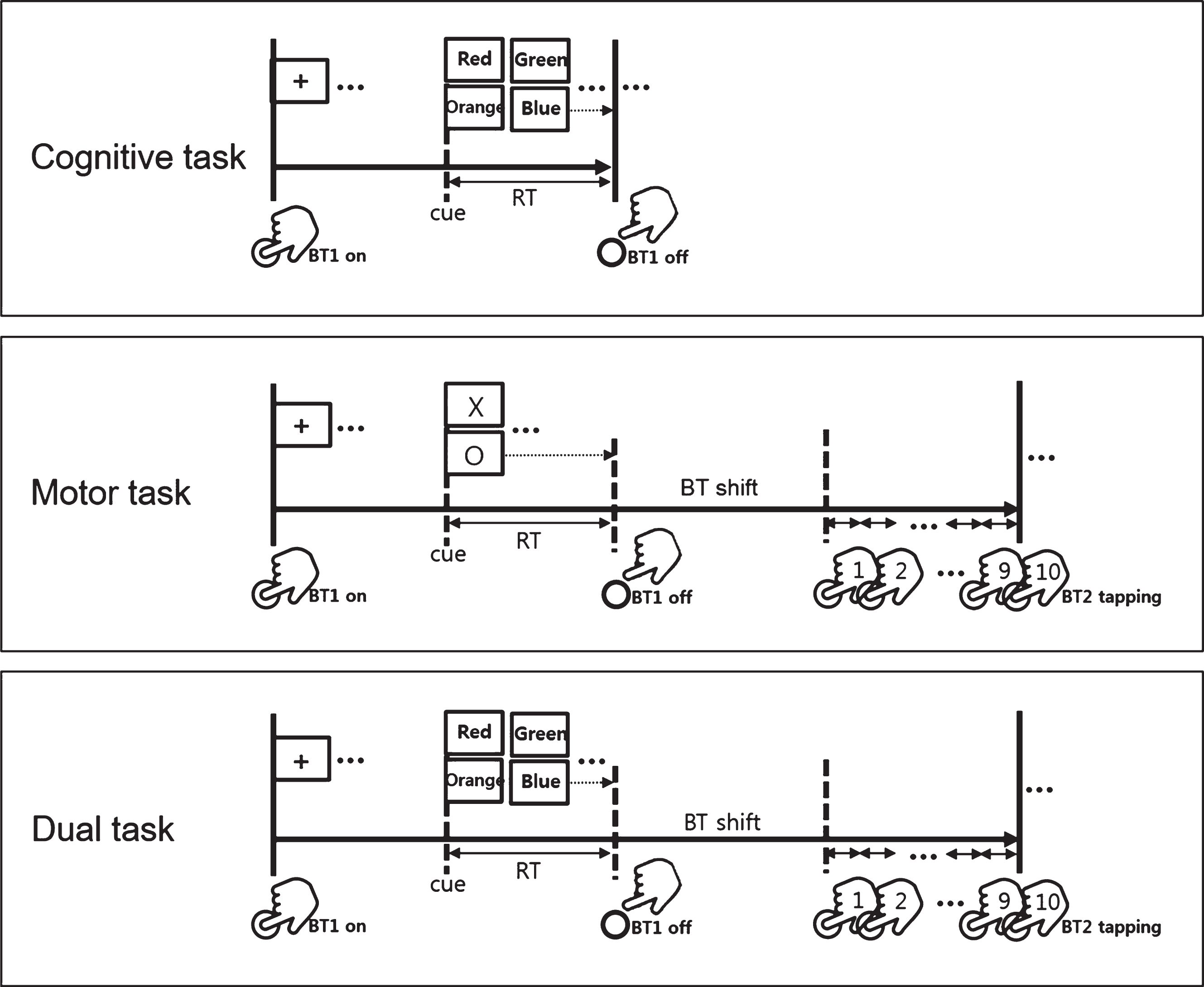
Experimental design of cognitive, motor, and dual tasks.
In the cognitive tasks (CT), a computerized Stroop test was used to assess the cognitive load. Participants were instructed to release BT1 as rapidly as possible if there was a match in the font color of a displayed word and its meaning (n = 48, Go trial), or to continuously press BT1 if there was a mismatch (n = 48, No-go trial).
In the motor tasks (MT), participants were required to release BT1, and then tap BT2 (17 cm from BT1) 10 times, as rapidly as possible, if the symbol “○” (n = 48, go trial) appeared, or continuously press BT1 if the “X” (n = 48, No-go trial) appeared. For the DT, elements of the CT and MT were combined; participants were instructed to release BT1, and then tap BT2 10 times as fast as possible, when the font color of a word and its meaning were congruent (n = 48, Go trial), or to continuously press BT1 if it was incongruent (n = 48, No-go trial).
We measured the reaction time (RT) of correct releases (RTCR) of BT1 during all tasks. During the MT and DT, we measured the latency period between releasing BT1 and pressing BT2, and we measured the finger tapping rate.
The demographic data of male and female participants in this study were compared by independent t-tests, while ANOVA and post-hoc Bonferroni tests were applied to compare the differences between the measurements in CT, MT, and DT. Further, paired t-tests were applied to compare the differences between the measurements in MT and DT. The DTI was obtained by calculating the ratio of RTCR in CT and MT divided by the RTCR in DT. To measure the level of cognitive load in CT/MT compared to DT, the ratios of the RTCR, BT shifting time, and the finger tapping rate in CT/MT were divided by these ratios in DT. To evaluate the impact of the cognitive load on subjects, the % CT/DT, % MT/DT, and % DT/DT were compared by ANOVA and Bonferroni post-hoc tests, while the % MT/DT and % DT/DT were compared using paired t-tests. Pearson’s correlation coefficients were calculated to assess the correlation between the measured variables of the computerized tasks and demographic data. All the statistical analyses were performed using the SPSS 22.0 statistics software for Windows (SPSS Inc., Chicago, IL,USA).
Results
Table 1 shows the demographic data of the male and female farmers recruited in the study. Hand grip strength was significantly higher in males than in females (35.8±5.9 vs. 23.4±6.4, F = 0.006, p < 0.001), while age, BMI, and total score on the MMSE-K, K-BDI, and SPPB were not significantly different between the two groups.
Demographic data of study participants
Demographic data of study participants
Values are presented as mean±SD. BMI, Body mass index; MMSE-KC, Korean version of the Mini-Mental State Examination; K-BDI, Beck Depression Inventory Korean version; SPPB, Short Physical Performance Battery.
Table 2 shows the computerized task measurements as well as intergroup comparisons. The RTCR increased in the following order (F = 21.9, p < 0.001 by one-way ANOVA): MT (1199.2±194.5 ms), CT (1292.7±378.6 ms), and DT (1658.1±435.0 ms), and was significantly different among the three task conditions (CT vs. DT, p < 0.001; MT vs. DT, p < 0.0014; CT vs. MT, p = 0.612 by Bonferroni post hoc test). The BT shifting time (F = 45, p = 0.065) and finger tapping rate (F = 45, p = 0.170) were similar between MT and DT.
Results of computerized task measurements with comparisons between cognitive, motor, and dual tasks
Values are presented as mean±SD. CR, correct release. Analyzed by *one-way ANOVA with Bonferroni post-hoc test and **paired t-test.
Figure 3 shows the ratios of RTCR in CT and MT tasks compared to the ratio of RTCR in DT, which are presented as % CT/DT, % MT/DT and % DT/DT. The ratios of RTCR were higher in MT (74.2±10.1%) and in CT (78.6±13.0%) compared to DT (100%), and the differences were significant (F = 97.3, p < 0.001 by one-way ANOVA, CT vs. DT, p < 0.001; MT vs. DT, p < 0.001; CT vs. MT, p = 0.083 by Bonferroni post hoc test). The ratio of BT shifting time in MT was significantly lower (92.0±23.7%, F = 45, p = 0.027 by paired t-test), and the ratio of finger tapping rate was significantly higher (106.1±19.1%, F = 45, p = 0.036 by paired t-test) than in DT (100%).
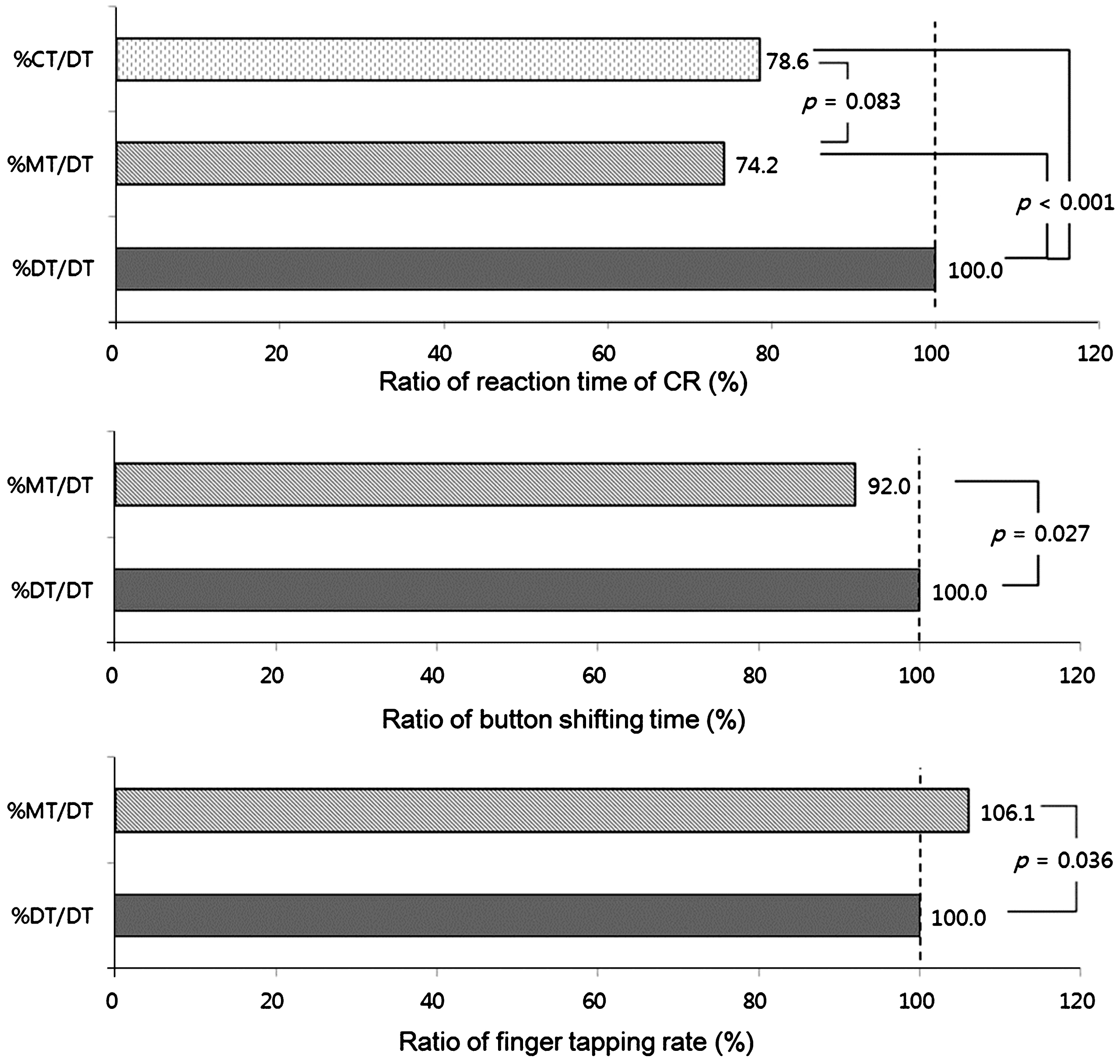
Dual task interference in the cognitive, motor, and dual tasks expressed as ratios.
Table 3 shows the Pearson’s correlation coefficients for the results of the computerized tasks and demographic data. There was a significant correlation between the total MMSE score and % MT/DT of RTCR (r = 0.304, p = 0.04), and the total MMSE score and % MT/DT of button shifting time (r = 0.293, p = 0.048); significant correlations between other parameters, however, were not observed.
Pearson’s correlation coefficients between ratio of computerized task measurements and demographic data, adjusted by education period and grip strength
RT, reaction time; CR, correct release; BT, button; CT, cognitive task; DT, dual task; MT, motor task; BMI, body mass index; MMSE-KC, Korean version of the Mini-Mental State Examination; K-BDI, Beck Depression Inventory Korean version; SPPB, Short Physical Performance Battery.
Daily activities, such as walking and driving are DTs composed of cognitive and motor tasks, which may induce DTI. This study focused on investigating the DTI in hand tasks by using single and dual tasks, separately, which has not been done in previous DTI studies, even though this is crucial in understanding the processes involved in dailyactivities.
DTI can be explained as a distraction from the primary task, while focused on another task being performed simultaneously (S. Ghai, I. Ghai, & A.O. Effenberg, 2017). The performance of DTs may result in impaired performance, as opposed to when one is performing a single task because the requirement of cognitive processing is higher in DTs; this is explained by the bottleneck and central sharing model theories (Shashank Ghai et al., 2017). Another model that support this notion is the limited capacity model (Lang, 2000), which states that although one of the tasks may have access to sufficient resources for information encoding, storage or retrieval, there may be insufficient resources for the other task that is being performed simultaneously (Yang et al., 2017). The DTI measured in this study shows a delay in the RTCR during the performance of simultaneous tasks; which concurs with both the bottleneck and the limited capacity models.
In this study, we found that the RTCR in MT was significantly higher than in DT, which may indicate that the cognitive load was higher prior to the cognitive task. We also found a significantly higher RTCR in CT than in DT, which also indicates the presence of a higher cognitive load. The increased BT shifting time and reduced finger tapping rate in DT compared to MT could reflect the presence of a residual cognitive load following the computerized Stroop test in DT. This residual cognitive load was gradually reduced from 25.8% (RTCR) to 8% (BT shifting time) to 6.1% (finger tapping rate) in % MT/DT compared to % DT/DT. In other words, a higher cognitive load induced a reduction in performance in CT and DT than in MT. Assuming that the cognitive load present at the intuitive cue (in an eidetic task that does not involve cognitive load) in MT is the baseline, we investigated the residual cognitive load of CT and cognitive load present prior to BT shifting in DT by calculating the DTI. Serial decomposition of single or dual tasks in this study potentially showed the presence of a cognitive load at each stage of a task (see results in Fig. 4).

Proposed dual task interference pattern of cognitive, motor, and dual tasks.
Performance reductions from single- to dual-task conditions are called dual task costs (Schaefer, 2014). When comparing the measurements of the computerized tasks, only the RTCR between CT and DT, and MT and DT show significant differences. However, the calculated percentages relative to DT showed additional significant differences between % CT/DT and % MT/DT for RTCR, and % MT/DT and % DT/DT for BT shifting time and finger tapping rate. When standardized values for the measurements of the computerized tasks were not used, performances were more varied among participants, which may have resulted in non-statistically significant differences. Thus, we decided to evaluate the calculated DTI using individual calculated ratios of taskmeasurements.
The pattern of DTI was investigated in this study to understand if the extent of DTI depends on the type of task being performed. The design of the DT training and daily activities were in alignment with the purpose and level of the tasks. The degree of interference varied based on the type of cognitive task. A higher cognitive load was observed in spontaneous speech and visuomotor reaction tasks (Patel & Bhatt, 2014; Plummer-D’Amato et al., 2008). Moreover, the difficulty level of the tasks were related to the interference of DT (Yang et al., 2017). In this study, we observed cognitive-related motor interference, which means that more attention resources were allocated to the cognitive task, and less to the motor task (Yang et al., 2017). Thus, the type of task should be considered carefully to help achieve the goal.
This study has several clinical and research implications. First, a DT performance in healthy subjects could be a more specific screening marker in assessing decreasing daily performances as opposed to a single task performance. Second, even though the results of this study were promising in showing a high cognitive load in DT, the DTI may be dependent on the type of task. Thus, specific motor or cognitive dysfunctions that affect typical daily activities may be reduced by safe, appropriate training exercises. Third, in a normal setting, to reduce the DTI caused as a result of the preceding cognitive load, clinical interventions are required to help enhance task prioritization. For example, an event-based intention with specific cues, self-initiated processing, and specification of intention by prepositioning exercise with self-driven tasks may be ways of reducing DTI (Schaefer, 2014). Finally, DT training is very important for improving cognitive and motor performance as it enables the modulation of consciousness-dependent motor activities to a more automatic state, and thereby reduces DTI (Caruso, 2005).
In conclusion, this study investigated the DTI by comparing a single task with a DT using serial decomposition, which may be an easy way to observe the individual inference patterns in task processing. The results of our study showed the different residual and preceding cognitive loads during the processing of each task, and could be used to measure the DTI when these tasks are performed simultaneously. In the future, for people’s safety, DT with cognitive or motor tasks with various levels of difficulty should be investigated to determine the pattern and level of DTI before developing daily training tasks.
Footnotes
Acknowledgments
This work was carried out with the support of Cooperative Research Program for Agriculture Science and Technology Development (Project No: PJ0125092018), Rural Development Administration, Republic of Korea.