
Abstract
Background:
Extracranial-intracranial (EC-IC) bypass surgery has been used to improve the conditions of cerebral ischemia symptoms for selected patients resulting from diverse complications such as stroke and atherosclerotic disease. However, several clinical trials showed EC-IC bypass surgery failed to prevent recurrent ischemic stroke in certain patients.
Objective:
Our clinical trial aimed to investigate whether there is a correlation between pre-surgery assessments and prognosis of patients received EC-IC bypass operation.
Methods:
We divided all patients into 4 groups according to their compensatory stages of cerebral ischemia. The values of cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT), time to peak (TTP), and oxygen extraction fraction (OEF) were obtained by computed tomography perfusion (CTP), single photon emission computed tomography (SPECT), and positron emission tomography (PET) at different time points before and after EC-IC bypass surgery. We assessed the correlations between the compensatory stage with modified Rankin scale (mRS) scores, survival rates, stroke and TIA incidences over the 12 months after surgery.
Results:
Patients with normal CBF, normal or increased CBV, and normal OEF tended to have a better prognosis after the EI-CI bypass operation than patients with abnormal CBF, CBV and OEF. However, patients with abnormal CBF and CBV, and increased OEF showed elevated mRS, less survival rates, and higher stroke and TIA incidences over the 12 months after surgery, compared to the groups with normal CBF, CBV and OEF.
Conclusions:
Our results suggest that a defined compensatory stage of cerebral ischemia might be useful for the prognosis of patients receiving EI-CI bypass surgery.
Keywords
Introduction
Extracranial-intracranial (EC-IC) bypass surgery has been used to improve the conditions of cerebral ischemia symptoms resulting from diverse complications such as stroke and atherosclerotic disease. For atherosclerotic patients with cerebrovascular insufficiency, EC-IC bypass surgery has been regarded as a late stage treatment choice when aggressive medical therapy fails (Baron et al., 1981; Chater, 1983; Derdeyn, Grubb, & Powers, 2005; Sundt, Whisnant, Fode, Piepgras, & Houser, 1985; Yasargil & Yonekawa, 1977). These patients commonly undergo “borderline” perfusion and have transient ischemic symptoms or stroke development when native collateral vessels fail to sufficiently perfuse the territory at risk. For this population of patients, the efficacy of cerebral revascularization remains debatable (Amin-Hanjani, Butler, Ogilvy, Carter, & Barker, 2005; Chater, 1983; Sundt et al., 1985; Yasargil & Yonekawa, 1977). A Japanese EC-IC bypass Trial (JET) study group investigated 196 patients with hemodynamic cerebral ischemia and major cerebral artery occlusive diseases to determine whether EC-IC bypass surgery could prevent recurrent stroke in these patients. They revealed that surgically treated group exhibited a significantly lower incidence of stroke recurrence compared to medically treated control group (p = 0.046) (Komatani, Okamoto, Aoki, Noguchi, & Morioka, 2017).
However, Powers WJ et al. demonstrated that 2 years after treatment, medical therapy cooperated with EC-IC bypass surgery failed to show significant reduction of the risk of recurrent ipsilateral ischemic stroke compared with medical therapy alone in patients with symptomatic atherosclerotic internal carotid artery occlusion (AICAO) and hemodynamic cerebral ischemia (Powers et al., 2011). The EC/IC Bypass Study Group further confirmed that EC-IC bypass surgery failed to prevent recurrent ischemic stroke in patients with symptomatic internal carotid artery occlusion (Group, 1985). In order the assess the value of EC-IC bypass surgery, Peerless SJ and colleagues conducted a large scale of clinical trial, in which they randomly recruited 1377 patients with symptomatic atherosclerosis. These patients received either medical care alone, or EC-IC bypass surgery with medical care. This study showed that immediately following surgery, surgical patients exerted more dysfunction in some activities such as dressing, cutting food, pouring beverages, sitting down, getting in bed, and speech fluency. At 4.5 months, surgical patients had no significant dysfunction in most activities except in toileting. However, six months after surgery, these two groups showed no dramatic differences. This study indicated that EC-IC bypass surgery lead to transient worse functional status (Dai et al., 2013).
Based on the controversial conclusion, we aimed to investigate whether preoperative assessment would improve the prognosis of patients underwent EC-IC bypass surgery. We selected 541 patients who present acute or recurrent cerebral ischemia symptoms. By the neuroimaging analysis, we found they had occlusion or stenosis of middle cerebral artery (MCA) or arteria carotis interna (ACI). Vessels with lesion were suffered from insufficient remote collateral circulation. They also exhibited insufficient cerebral perfusion and consequent cerebral ischemia. We divided the patients into 4 groups according to their compensatory stages of cerebral ischemia. The values of cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT), time to peak (TTP), and oxygen extraction fraction (OEF) were measured by computed tomography perfusion (CTP), single photon emission computed tomography (SPECT), and positron emission tomography (PET) at 5 time points: 1 day before surgery; 1 week, 3 months, 6 months and 12 months after EC-IC bypass surgery. The outcomes including survival rate, modified Rankin scale (mRS), the incidences of recurrent stroke and transient ischemic attacks (TIA) were evaluated in all patients over 12 months after surgery.
Methods
Patients
From Oct. 2015 to Apr. 2017, a total of 541 patients with acute or recurrent cerebral ischemia symptoms were enrolled in this study. In addition, 177 patients who did not receive surgery were included as control. Clinical manifestations of these patients include insufficient remote collateral circulation and cerebral perfusion, which are consistent with the symptoms of cerebral ischemia. Patients with immune diseases-caused vascular inflammation ischemia, such as thyroid disease and lupus erythematosus that appear in young females, were excluded. Detailed information of the patient characteristics were shown in Table 1. The indications for surgery basically include: 1) chronic or frequent episodes of cerebral ischemia; 2) occlusion or stenosis of middle cerebral artery or intracranial artery intracranial segment identified by digital subtraction angiography (DSA), magnetic resonance angiography (MRA) and computed tomographic angiography (CTA), and poor circulation of the distal end of the lesion; 3) cerebral hypoperfusin idenfified by CT or MR perfusion scanning, which is consistent with clinical ischemia; 4) ischemic ischemia caused by immune disease, such as female thyroid disease and lupus erythematosus. After the surgery, CTA, DSA, and MRA methods were used to observe and assure the patency of grafted vessels. Each patient received CTP, SPECT, and PET examinations 1 day before surgery and reexamination on 1 week, 3 weeks, 6 months, and 12 months after EC-IC bypass surgery. All patients were evaluated by mRS. Our study was approved by the local ethical committee of The Second Hospital of Hebei Medical University, and written informed consents were available.
Characteristics of patients
Characteristics of patients
Categorical variables were compared by χ2 and Fisher tests. Group I: Normal CBF and CBV, prolonged MTT and TTP, normal OEF. Group II: Normal CBF and increased CBV, prolonged MTT and TTP, normal OEF. Group III: Reduced CBF and increased CBV, prolonged MTT and TTP, increased OEF. Group IV: Increased CBF and CBV, decreased MTT and TTP, increased OEF.
As shown in Fig. 1, patients were divided into 4 groups according to the diagnostic values of CBF, CBV, MTT, TTP, and OEF. Group I: Patients showed normal CBF and CBV, prolonged MTT and TTP, normal OEF; Group II: Patients showed normal CBF and increased CBV, prolonged MTT and TTP, normal OEF; Group III: Patients showed reduced CBF and increased CBV, prolonged MTT and TTP, increased OEF; Group IV: Patients showed increased CBF and CBV, decreased MTT and TTP, increased OEF. One day before surgery, the degree of neurological disability of patients were assessed using mRS. Follow-up examinations were conducted on 1 week, 3 months, 6 months, and 12 months postoperatively, which included mRS assessment, stroke relapse rate, TIA incidence, and survival rate.
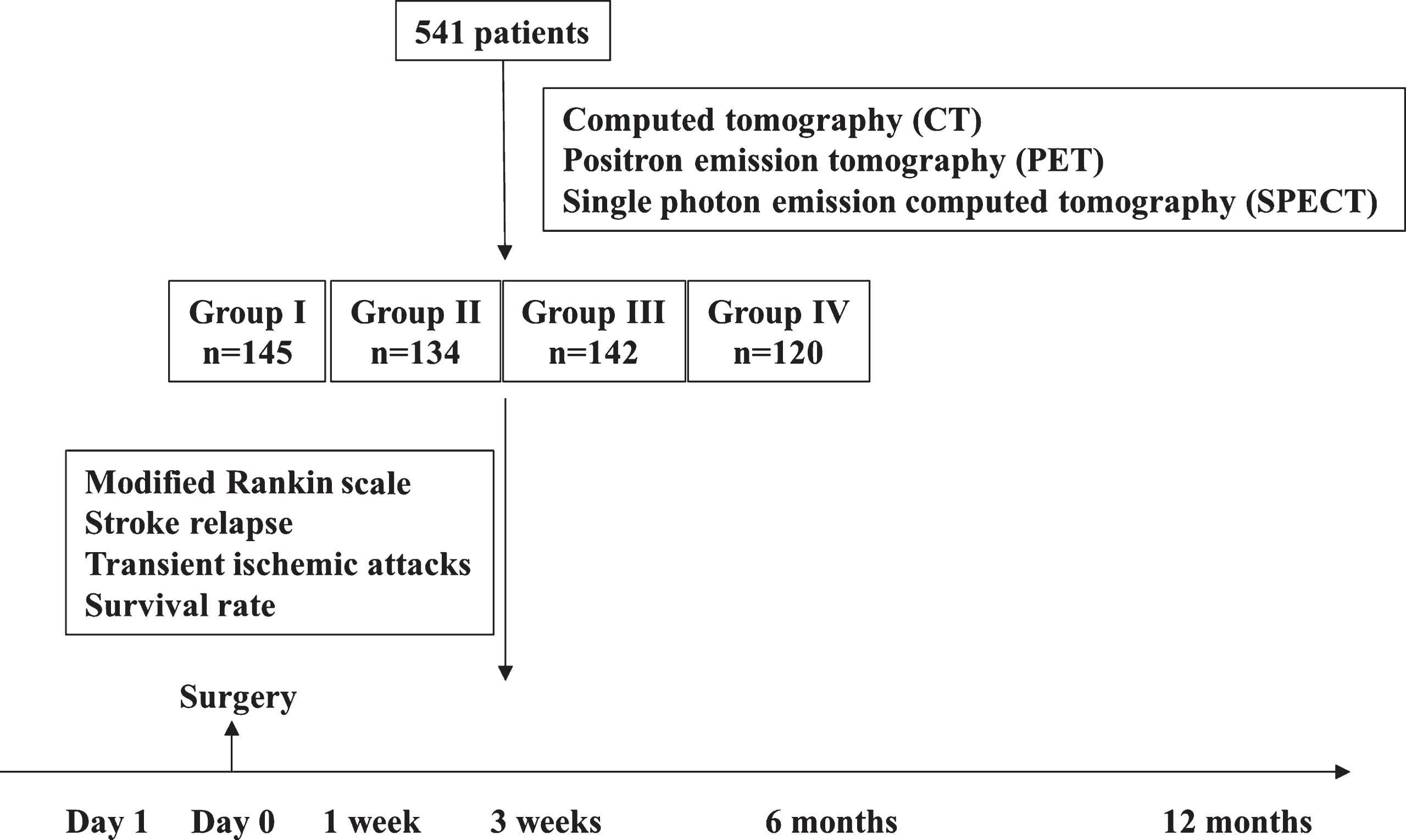
The study design. The patients were divided into 4 groups according to the diagnostic values of cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT), time to peak (TTP), and oxygen extraction fraction (OEF). Group I: Normal CBF and CBV, prolonged MTT and TTP, normal OEF; Group II: Normal CBF and increased CBV, prolonged MTT and TTP, normal OEF; Group III: Reduced CBF and increased CBV, prolonged MTT and TTP, increased OEF; Group IV: Increased CBF and CBV, decreased MTT and TTP, increased OEF. One day before surgery, the degrees of neurological disability of patients were assessed by mRS. Follow-up examination were conducted at 1 week, 3 months, 6 months, and 12 months postoperatively, which included mRS assessment, stroke relapse rate, transient ischemic attafcks (TIA) incidence, disability rate and survival rate.
The method was previously described by Dai et al. (2013). Briefly, CTP scan was performed in the transverse plane using the equipment, a 64-slice multi-detector CT scanner (SOMATOM AS 128; Erlangen, Germany) (Dai et al., 2013). CTP consisted of a 60-s series, with 30 gantry rotations performed in cine mode during the intravenous administration of iodinated contrast material (Dai et al., 2013). Images were acquired and reconstructed at a temporal sampling rate of 1 image per 2 s, resulting in a series of 20 images for each assessed section (Dai et al., 2013). After unenhanced CT scan of the whole brain, eight adjacent, 8-mm-thick sections were selected by starting at the level of the basal ganglia (Dai et al., 2013). A 50-ml bolus of nonionic contrast media (Ultravist 370, Schering Health Care Ltd., Burgess Hill, UK) was administered into an antecubital vein by using a power injector (Stellant Injection System; Indianola, PA, USA) with an injection rate of 5 ml/s (Dai et al., 2013). Volume shuttle scanning mode, which can get 80 mm cerebral perfusion image in one time, was used to display range from basal ganglia region to brainstem region. At the same time, a CTA image could also be obtained.
Positron emission tomography measurements
PET measurements were conducted in each patient by a PET scanner, GE Advance (GE Healthcare, Milwaukee, Wisconsin). Images were processed by a transmission scan with germanium-68/gallium-68. Then, 15O-gas tests were performed. Briefly, patients were continuously delivered C15O2 and C15O2 by a mask during the 5-minute scan. The value of CBV was obtained by measuring bolus inhalation of C15O with 3 minutes of scan. A previous steady-state method was used to obtain the values of CBF and OEF. MTT and TTP were calculated.
Statistical analysis
Categorical variables were compared by χ2 and Fisher tests. Nonparametric multigroups comparisons were performed using the Kruskal-Wallis test. The log-rank test was used to assess differences in survival curves. Chi-square test was used for verify the significance of the differences in the incidence of stroke and TIA. P≤0.05 was considered to be statistically significant.
Results
Totally 541 patients with acute or recurrent cerebral ischemia and received surgery were recruited and 177 patients who did not receive surgery were included as control. They exhibited occlusion or stenosis of MCA or ACI, insufficient remote collateral circulation of vessels with lesions, insufficient cerebral perfusion, and consequent cerebral ischemia. We divided the 541 patients into 4 groups based on their diagnostic values of CBF, CBV, MTT, TTP, and OEF, as demonstrated in methods, and 177 patients in control group who showed same situations as group I, but did not receive the surgery. As shown in Tables 1 and 2, there was no significant difference in the characteristics of patients between the 4 groups and control group. Patients who died during the study were not included for the analysis of mRS.
Characteristics of patients
Characteristics of patients
Categorical variables were compared by χ2 and Fisher tests. Control and Group I: Normal CBF and CBV, prolonged MTT and TTP, normal OEF.
One day before surgery, the 4 groups showed similar distributions of mRS scores. However, after 3 weeks of surgery, both Group I and Group II showed lower mRS compared to Group III and Group IV (p < 0.01, Table 3 and Fig. 2). The mRS of control group was higher than Group I during the whole observation period (Fig. 3 and Table 4). It was observed that less than 70% of patients in Group III and IV who had abnormal CBF, CBV, MTT and TTP and increased OEF were evaluated to mRS 0-1 whereas the percentage was larger in Group I and II. After 12 months of surgery, only 8% of patients in Group II were on mRS 4-5, which was much less than the percentages in other groups. However, patients in group II with normal CBF and OEF, elevated CBV, and prolonged MTT showed a higher occupancy in the lower scores of mRS than patients in other groups (p < 0.01). Patients in Group I exhibited a slowly increasing trend of mRS over the one year after surgery, which led to a significant higher mRS compared to Group II on 12 months (p < 0.05).
Modified Rankin score
Modified Rankin score
Among this modified Rankin scale, 6 (death) was not included. Group I: Normal CBF and CBV, prolonged MTT and TTP, normal OEF. Group II: Normal CBF and increased CBV, prolonged MTT and TTP, normal OEF. Group III: Reduced CBF and increased CBV, prolonged MTT and TTP, increased OEF. Group IV: Increased CBF and CBV, decreased MTT and TTP, increased OEF.
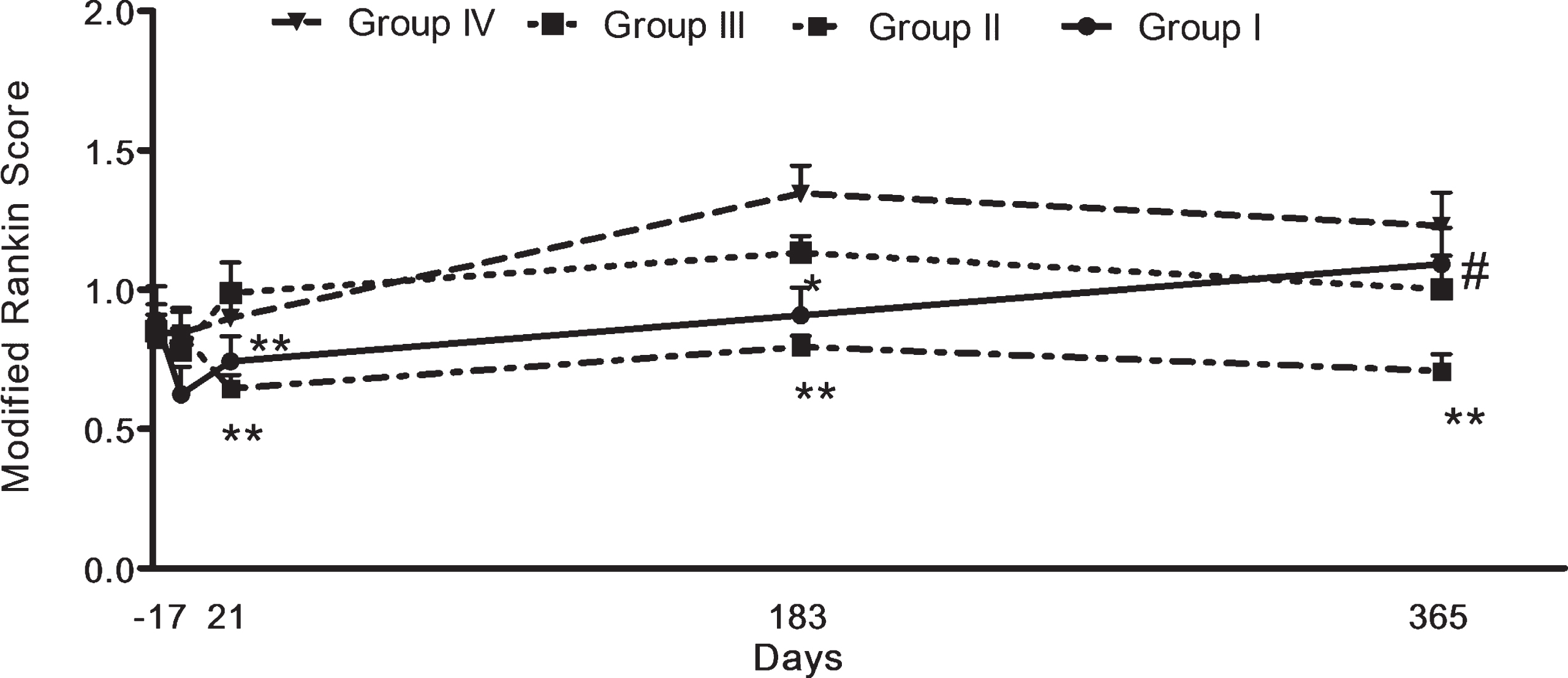
Functional outcomes after extracranial-intracranial bypass surgery. Patients of the Group I and II showed an obviously preferable mRS trends compared to the other three groups. The comparisons between multigroups were performed using the Kruskal-Wallis test. *p < 0.05, **p < 0.01, was compared to Group III or Group IV. #, p < 0.05 was compared to Group I. P≤0.05 was considered to be statistically significant.
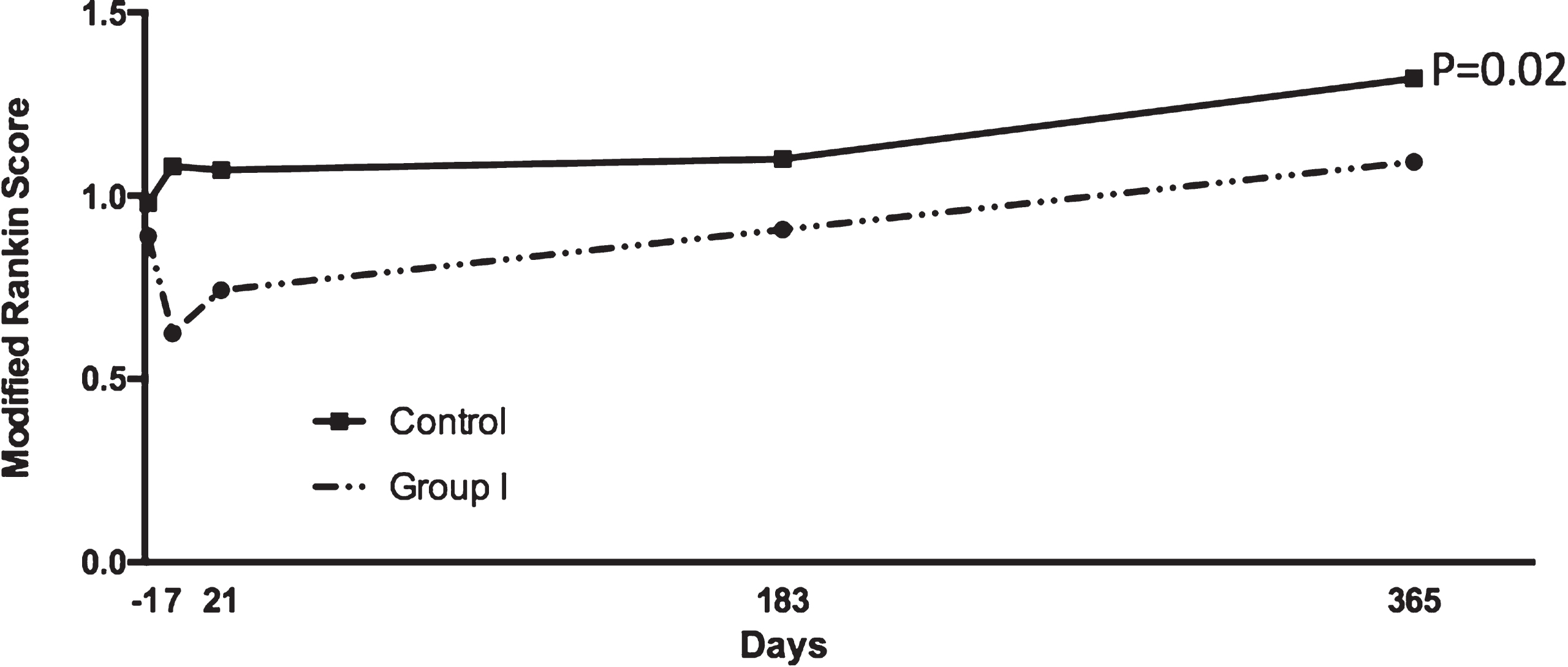
Functional outcomes after extracranial-intracranial bypass surgery. Patients of the Group I showed lower mRS compared to control group. The comparisons between two groups were performed using the t-test. **p < 0.02, P≤0.05 was considered to be statistically significant.
Modified Rankin score
Among this modified Rankin scale, 6 (death) was not included. Control and Group I: Normal CBF and CBV, prolonged MTT and TTP, normal OEF.
We analyzed the survival rates among all of the 4 Groups (Fig. 4) as well as the control group (Fig. 5). The one-year survival rates were shown in Fig. 4. About 85% (95% CI 0.79–0.94) patients survived in Group I, which was significantly higher than Group II (72%; 95% CI 0.65–0.76), Group III (66%; 95% CI 0.55–0.76) and Group IV (52%; 0.42–0.64). The survival rate of control group was significantly lower than Group I (Fig. 5), demonstrating that those patients could benefit from the surgery.
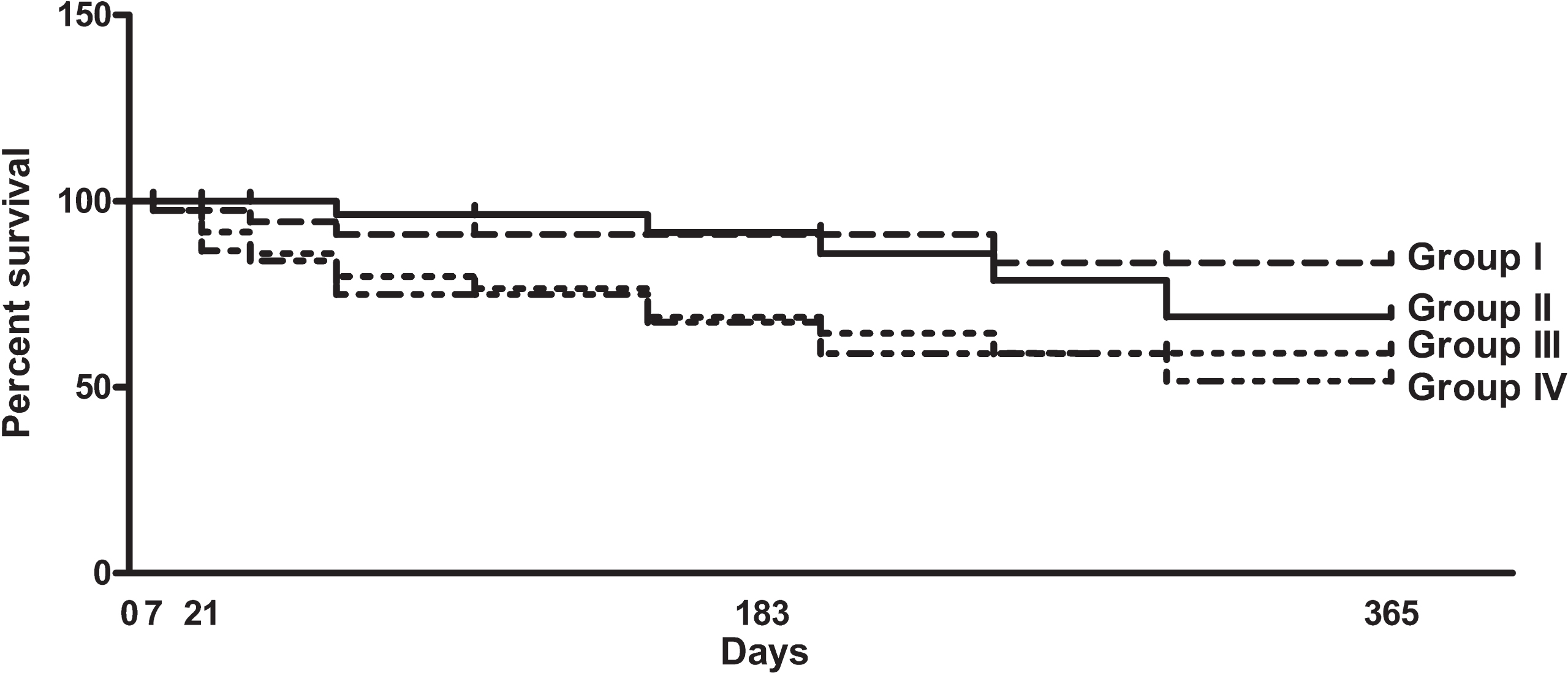
Survival rates after extracranial-intracranial bypass surgery. The survival rates in Group I (85%; 95% CI 0.79–0.94), Group II (72%; 95% CI 0.65–0.76), Group III (66%; 95% CI 0.55–0.76) and Group IV (52%; 0.42–0.64). The log-rank test was used to assess differences in survival curves.
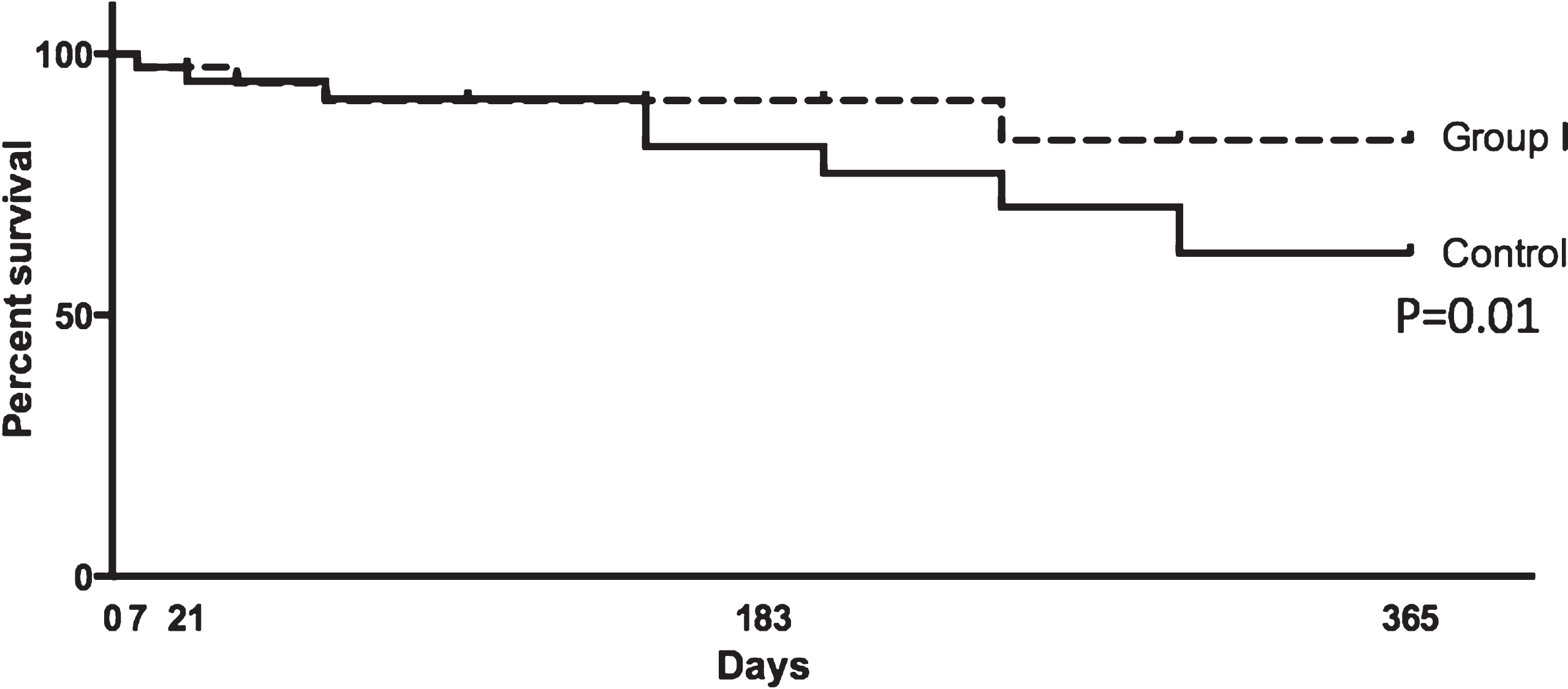
Survival rates after extracranial-intracranial bypass surgery. The survival rates in Group I (85%; 95% CI 0.79–0.94), and control group. The log-rank test was used to assess differences in survival curves.
We further analyzed the incidences of stroke and TIA during the follow-up period. Higher percentages of patients who exhibited stroke and TIA in Group III and Group IV (p = 0.0248). Additionally, patients from Group I underwent a significant decrease of stroke incidence after 6 months of surgery (p = 0.0211). The stroke incidence of patients from Group III and IV was steadily increased after EI-CI bypass surgery (Fig. 6). Similar trends were observed in the incidence of TIA. However, TIA incidence in patients of Group II was significantly higher than that of the Group I after 6 months of surgery, but was still dramatically lower than that of the Group IV (Fig. 7, p = 0.0183). The incidences of both stroke and TIA of Group I were lower than that of control group (Figs. 8 and 9).
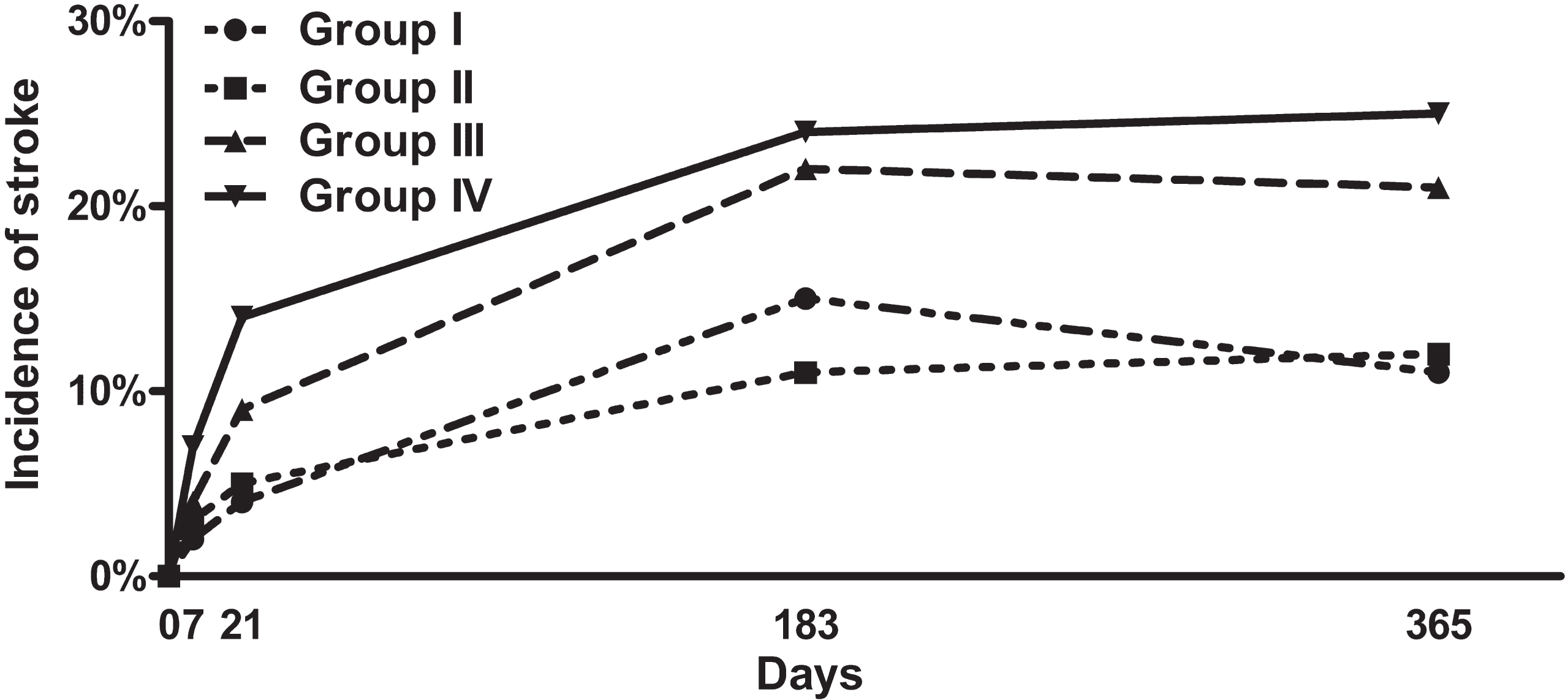
The incidence of stroke after extracranial-intracranial bypass surgery. Higher percentages of patients who exhibited stroke and TIA in Group III and Group IV (p = 0.0248). Patients from Group II underwent a significant decrease of stroke incidence since 6 months after surgery (p = 0.0211). Patients of Group III had a slight but not significant reduction of stroke incidence at 12 months after surgery, while the stroke incidence of patients from Group IV steadily increased after EI-CI bypass surgery. Chi-square test was used for verify the significance of the differences.
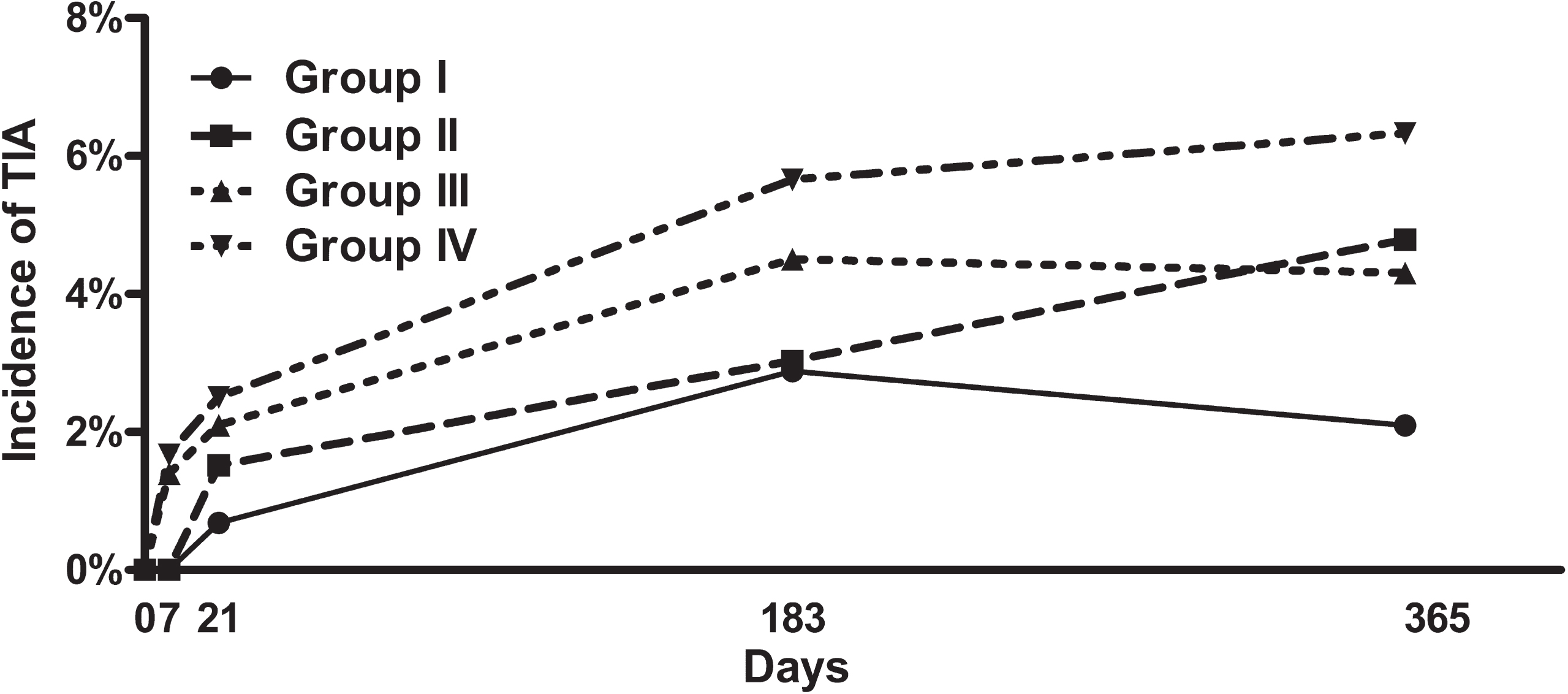
The incidence of TIA after extracranial-intracranial bypass surgery. TIA incidence in patients of Group II was significantly higher than that of the Group I after 6 months of surgery, but was still dramatically lower than that of the Group IV (p=0.0183). Chi-square test was used for verify the significance of the differences.
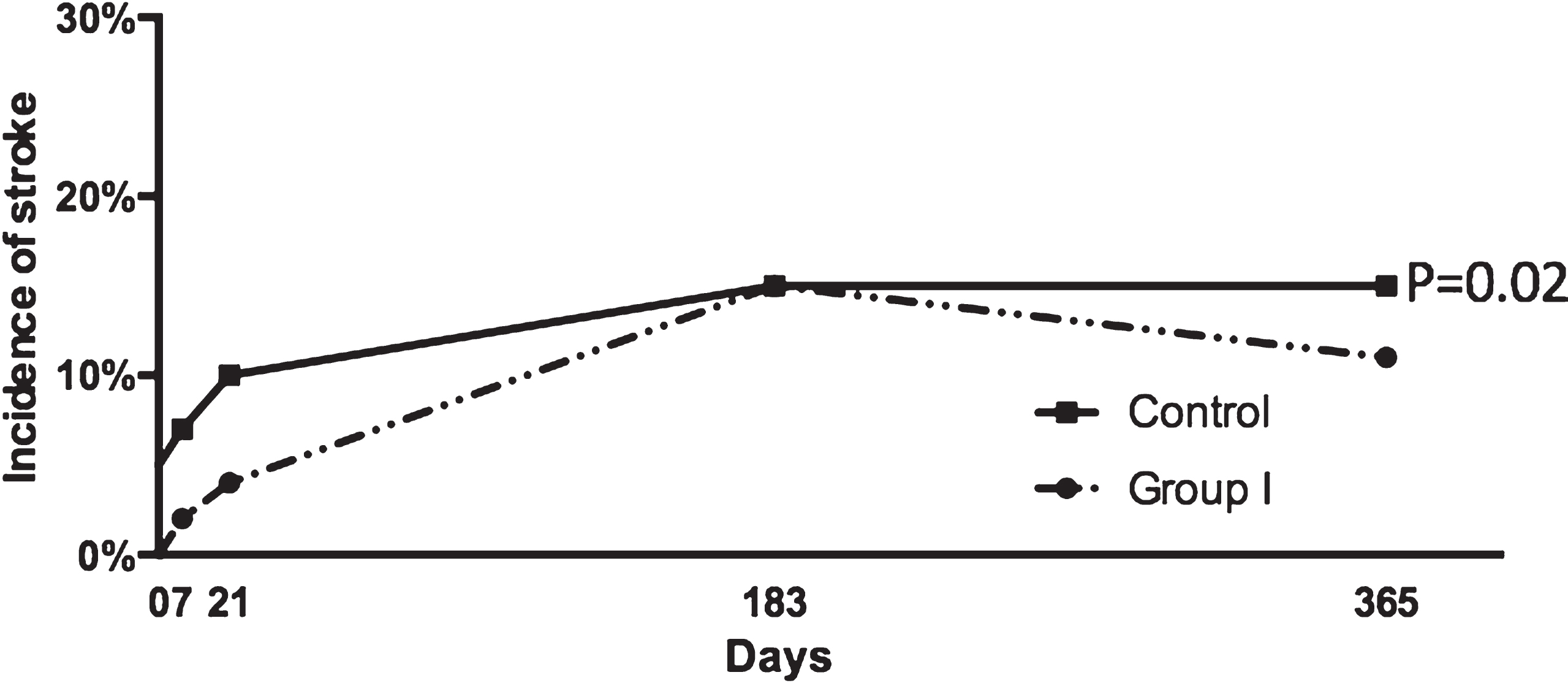
The incidence of stroke after extracranial-intracranial bypass surgery. Higher percentages of patients who exhibited stroke in control Group compared to Group I (p = 0.02). Chi-square test was used for verify the significance of the differences.

The incidence of TIA after extracranial-intracranial bypass surgery. Higher percentages of patients who exhibited TIA in control Group compared to Group I (p = 0.02). Chi-square test was used for verify the significance of the differences.
The cerebrovascular diseases are among the leading threatens to public health worldwide (Krishnamurthi et al., 2013; Writing Group et al., 2016). Even though ischemic stroke might be the wide known end-organ effect, abnormality of the cerebral circulation is the main cause of hemorrhagic stroke and other types of neurological dysfunction and degeneration (Iadecola, 2013; Korczyn, 2015; Wardlaw, Smith, & Dichgans, 2013). Initially, ischemic stroke derives from carotid and cerebrovascular diseases. The progression of ischemic stroke is normally chronic and depends on diverse factors. Specifically, the cerebrovascular diseases include both small-vessel disease and large vessel disease. During small-vessel disease, macrovascular changes and lead to ischemia and microbleeds at certain small regions (Akoudad et al., 2016). After initiated, both small-vessel disease and large vessel disease progress slowly over several years. The rate of progression is influenced by aging and the vascular risk factors, such as hypertension, inactivity, smoking, diabetes, obesity, etc (Hu, De Silva, Chen, & Faraci, 2017).
The occlusion of intracranial or cervical vessel normally initiate acute ischemic stroke (AIS) as in most cases the occlusion reduces blood flow to an area of brain, resulting in infarction of that portion of brain tissue. When CBF is dramatically decreased, various cellular consequences pursue, such as excitoxicity, mitochondrial dysfunction, oxidative stress, post-ischemic inflammation, and microvascular injury blood-brain barrier (BBB) damage (Puyal, Ginet, & Clarke, 2013). The mechanisms of ischemic injury are different in brain areas with few or no CBF and more modest reductions of CBF. Moreover, the temporal evolution of ischemic injury is also distinct. The brain tissue regions suffering from initially moderate CBF reduction are possible to be salvaged (Bardutzky et al., 2005). These potentially salvageable ischemic tissues are addressed as ischemic penumbra. The basis of the acute stroke therapy is to save part or even all of the ischemic penumbra (Fisher & Bastan, 2012). While the ischemic tissues that progress to irreversible damage is called the ischemic core. Both ischemic penumbra and ischemic core can be identified by CT and magnetic resonance imaging (MRI) techniques (Fisher & Albers, 2013). AIS therapies such as drugs targeted at the ischemic cascade, enhancing collateral blood flow, and quickly reestablishing CBF to the ischemic region can affect the evolution of the ischemic core and penumbra. Besides, some other factors such as temperature, collateral blood supply, and metabolic components can also influence the evolution of the ischemic core and penumbra (Heiss, 2012). Currently, the enhanced understanding of the basic pathophysiology of ischemic damage, optimized imaging techniques, improved therapeutic strategies to restore blood flow, and advanced drug delivery systems ensure more effective therapy for AIS patients.
In this study, although we aimed to included patients with similar health status prior surgery, there are still several differences found between the 4 groups. For example, patients from group IV showed a higher rate of hypertension while group III showed more patients who had a history of cerebral infarction and higher body mass index (BMI) compared to other groups. In addition, the number of patients with coronary artery disease was higher in group II compared to other groups. Thus, it is possible that patients with reduced CBF and increased OEF are suffering from a higher risk of cerebral infarction. As we known that occlusion of intracranial arteries is able to lead to CBF reduction and cause cerebral infarction while acute stage of cerebral infarction could increase OEF, it is suggested that patients with a history of cerebral infarction may show a worse prognosis of bypass surgery compared to those without. On the other hand, patients with hypertension may be also under a high risk of poor prognosis of bypass surgery whereas ischemic stroke may be not an important factor. Generally, patients in group I and II showed normal values of OEF, CBF and CBV, demonstrating that these patients may not be necessary to receive bypass surgery. However, according to the complicated factors involved in the pathophysiology of ischemic damage, it could be difficult to determine whether bypass surgery is necessary. Therefore, we used the compensatory stages of cerebral ischemia to reveal whether the stage could suggest influence of bypass surgery on patients with a risk of ischemic stroke.
Cerebral ischemia patients usually received EC-IC bypass operation for cerebral revascularization. However, the option of EC-IC bypass surgery depends on diverse factors, including the availability and accessibility of particular donor and recipient vessels, as well as the goals of the operation. As the efficacy of EC-IC bypass operation remains controversial (Komatani et al., 2017; Powers et al., 2011), we aimed to establish a novel system to assess the prognosis of EC-IC bypass operation, in order to effectively enhance the recovery rate of cerebral ischemia. The parameters of CBF, CBV, MTT, TTP, and OEF were acquired by CTP, PET, and SPECT. Theoretically, when perfusion pressure decreases, the value of MTT, TTP and OEF have two possible changes: MTT and TTP prolong with normal OEF; and MTT and TTP prolong with enhanced OEF. The cerebral metabolic imaging of healthy people shows that the OEF value of grey matter and white matter is 0.49 and 0.48 respectively. MTT and TTP values of different individuals differ significantly. Determining whether MTT and TTP values prolong is to compare the left and right sides.
In this study, patients from Group I and II presented preferable mRS than those from Group III and IV, which indicated that patients from Group I and II had better functional outcomes compared to patients from Group III and IV. Moreover, patients of Group I and II showed higher survival rate, and lower stroke incidence compared to patients from Group III and IV. Group I patients presented lowest TIA incidence among all the four groups. Even though Group II patients experienced increasing TIA incidence during the follow-up, the morbidity of TIA in Group II patients was comparable with that of Group III patients and lower than that of Group IV patients. However, we found that although Group II showed a higher incidence of TIA than Group I, the mRS scores of Group I was significantly lower than them of Group II. It is possible that patients in Group II exhibited an enhanced compensatory ability, which needs more evidences.
These results indicate that patients from Group I and II had a better prognosis than patients from Group III and IV did. Group I and II share a common feature of normal OEF, while the rest two groups had increased OEF. Previous studies supported that increased OEF was associated with higher stroke risk. For example, Jordan LC and colleagues used magnetic resonance imaging methods to determine whether increased OEF was uniquely present in patients who have higher levels of cerebrovascular impairment, and whether OEF could be utilized as a candidate biomarker of stroke risk. They assessed the physiological relationships between OEF, CBF, and clinical markers of cerebrovascular impairment in adults with sickle cell anaemia. Their results supported the hypothesis that OEF but not CBF was enhanced in patients with higher levels of cerebrovascular impairment. This indicated that OEF might be a viable marker for evaluating stroke risk in adults (Jordan et al., 2016). Similarly, Derdeyn CP et al. collected the data from 81 patients with symptomatic carotid occlusion, in order to study the relationship of CBV to CBF, OEF and CMRO2, and to stroke risk. They found 52.6% of patients with increased OEF and normal or reduced CBV suffered from ipsilateral strokes during follow-up, while 77.8% of patients underwent ipsilateral strokes with increased OEF and CBV. Their results presented a positive correlation between the ischemic stroke risk and the value of OEF and CBV. This indicates that for patients with increased OEF and CBV, the haemodynamic compromise degree is severe than those with increased OEF and normal CBV. For patients with increased OEF and chronic carotid occlusion, enhanced CBV might suggest obvious vasodilation due to exhausted autoregulatory vasodilation (Derdeyn et al., 2002).
Conclusions
Our results and the previous studies indicated that cerebral ischemic-derived compensation function indeed showed influences on the outcomes of EI-CI bypass surgery. Specifically, patients with normal CBF, normal or increased CBV, and normal OEF tended to have a preferable prognosis after the EI-CI bypass operation. While patients with abnormal CBF and CBV, and increased OEF exhibited worse mRS conditions, poorer survival rates, and higher incidences of stroke and TIA. According to our clinical trial results, it is suggested that the pre-operation evaluation may be an important factor to predict and improve the prognosis of patients receiving EI-CI bypass surgery.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This work was supported by the Planning Project of Science and Technology Department of Hebei Province (152777165). Key Science and Technology Research Projects of National Health and Family Planning Commission of Hebei Province (1120140146).
Footnotes
Acknowledgments
None.