
Abstract
Background:
Cognitive orientation to daily occupational performance (CO-OP) is a task-specific training applied using a cognitive behavioral approach to improve performance in daily activities and to enable the patient to overcome limitations related to them.
Objectives:
The purpose of this study was to investigate the effects of the CO-OP approach in comparison with task-specific upper extremity training (TUET) on performance related to daily and functional activities in individuals with chronic hemiparetic stroke.
Methods:
Forty-nine participants diagnosed with stroke for the first time underwent 30 minutes of either the CO-OP approach or TUET 5 days a week for 4 weeks. We evaluated their performance on the box-and-block test (BBT), Canadian occupational performance measure (COPM), and community integration questionnaire (CIQ) and Wolf motor function test-functional score (WMFT-F) before and after the training.
Results:
Our results show a significantly improvement in the WMFT-F, COPM-P, COPM-S, BBT, and CIQ scores after training in the CO-OP group, but only COPM-S score was significantly improvement after training in TUET group (p < 0.05). This study also found higher increases in the mean WMFT-F, COPM-P, COPM-S and BBT scores in the CO-OP group than in the TUET group, but CIQ score did not have a significantly higher increase between-group after training.
Conclusions:
The results of this study suggest that the CO-OP approach resulted in a positive therapeutic effect on self-selected occupational performance and daily and functional activities in individuals with chronic hemiparetic stroke.
Introduction
Stroke is a main cause of acquired long-term disabilities in adults, and can lead to neurological deficits related to cerebrovascular cause (O’Sullivan, Schmitz, & Fulk, 2014; Umphred, 2013). Survivors of stroke exhibit symptoms such as muscle weakness, reduction in sensory function, cognitive impairments, spasticity, excessive reflexes, apraxia, and agnosia. These symptoms increase the level of dependency in patients, restrict their participation in daily life, and may even lead to social isolation. Thus improving the quality of life by facilitating relief from the above symptoms is considered the most important therapeutic goals for stroke survivors (O’Sullivan, et al., 2014).
Recently, cognitive orientation to daily occupational performance (CO-OP) has been suggested to improve the motor performance of children with developmental coordination disorders and persons with stroke (Cameron et al., 2017; Jackman, Novak, Lannin, Galea, & Froude, 2018; Thornton et al., 2016). The CO-OP approach has its theoretical basis in Meichenbaum’s cognitive behavioral approach. It is defined as “a client-centered, performance-based, problem-solving approach that enables skill acquisition through a process of strategy use and guided discovery,” and superimposes cognitive elements on task-specific training (Missiuna, Mandich, Polatajko, & Malloy-Miller, 2001). The CO-OP approach transforms the focus of treatment protocols to improving performance in daily activities and generalizing and transferring on real-life activities rather than treating the underlying impairments (Wolf et al., 2016). In other words, the CO-OP approach is a top-down approach that improves participation and performance in daily activities, unlike the bottom-up approach that considers impairments (Wolf, et al., 2016).
The application of the CO-OP approach has been increasing since 2010 and has been shown to improve the daily and functional activities of patients who have undergone stroke (Dawson, Binns, Hunt, Lemsky, & Polatajko, 2013; Imms & Nott, 2012; McEwen et al., 2015). Dawson and colleagues reported that the CO-OP approach would have a broader positive effect on stroke recovery including upper extremity movement and cognitive flexibility than usual care in patients less than 3 months following stroke (Dawson, et al., 2013). McEwen and colleagues also reported that compared to usual occupational therapy, the CO-OP approach was associated with a greater effect on actual performance in trained and untrained self-selected functional activities in survivors of stroke that had occurred 3 months prior (McEwen, et al., 2015). All of the above studies involved patients in the acute or sub-acute phase of their rehabilitation period (less than 3 months following stroke).
As described above, the CO-OP approach adds cognitive elements to task-specific training. Task-specific training has been reported to show positive effects as a therapeutic approach for stroke rehabilitation (Lee, Kim, Choi, & Lee, 2013; Martins et al., 2017). In this study, we investigated whether the CO-OP approach is as effective as task-specific training in improving upper extremity function like in stroke survivors. More specifically, we studied the effects of the CO-OP approach on daily and functional activities in individuals with a chronic hemiparetic stroke.
Methods
Participants
Forty-nine individuals with hemiparetic stroke were recruited from a local rehabilitation unit for this study. The inclusion criteria for participation in this study were as follows: (1) Patients were diagnosed with the first onset of unilateral hemispheric stroke due to an ischemic or hemorrhagic attack 6 months prior to the study; (2) Patients had sufficient cognitive ability to understand and follow simple verbal instructions, as indicated by a mini-mental state examination score of 24 or higher; (3) Patients were capable of independent walking without any assistance for a distance of at least 10 meters; (4) Patients did not have visuoperceptual impairment; (5) Patients did not have any orthopedic conditions that affect the therapeutic effects; and (6) Patients did not have any other neurological diseases other than the first stroke (Folstein, Folstein, & McHugh, 1975; Wang et al., 2014). The exclusion criteria included severe depression, use of antidepressants and use of anti-epileptic drugs. The Chosun University Institutional Review Board (Permit No. 2-1041055-AB-N-01-2016-0032) approved the study protocol, and written informed consent was obtained from all the patients prior to their participation. Table 1 lists the demographic and clinical characteristics of the patients.
Demographic characteristics of study participants (N = 49)
Demographic characteristics of study participants (N = 49)
Values are presented as mean±standard deviation unless otherwise indicated. CO-OP, Cognitive Orientation to daily Occupational Performance; TUET, Task-specific upper extremity training; MMSE, mini-mental state examination.
This study used a two-group pretest-posttest design and a double blinded, randomized controlled trials with a 4-week intervention comprising the CO-OP approach with task-specific upper extremity training (TUET). The participants were divided randomly into the CO-OP (n = 25) and TUET groups (n = 25) by an independent person who selected the participants by picking out their assigned group names from sealed envelopes. An independent therapist concealed the allocation sequence. To prepare the training protocol, the participants selected three functional activities that would become the focus of CO-OP treatment or TUET during the Canadian Occupational Performance Measure (COPM) interview. The CO-OP group received cognitive training on the more affected side for 30 minutes per day, 5 times a week for 4 weeks, while the TUET group received task-specific training of upper extremity function for the same period. One participant in the TUET group did not complete the training; hence, the data collected from this patient was excluded from the analysis. Finally, 25 and 24 participants were included in the CO-OP and TUET groups, respectively. The outcome measures of this study were assessed 1 day before the training and 1 day after the training (Fig. 1). The same blinded therapist assessed participants at the beginning and end of the training, and the participants were blinded the features from their therapeutic groups throughout the training period.
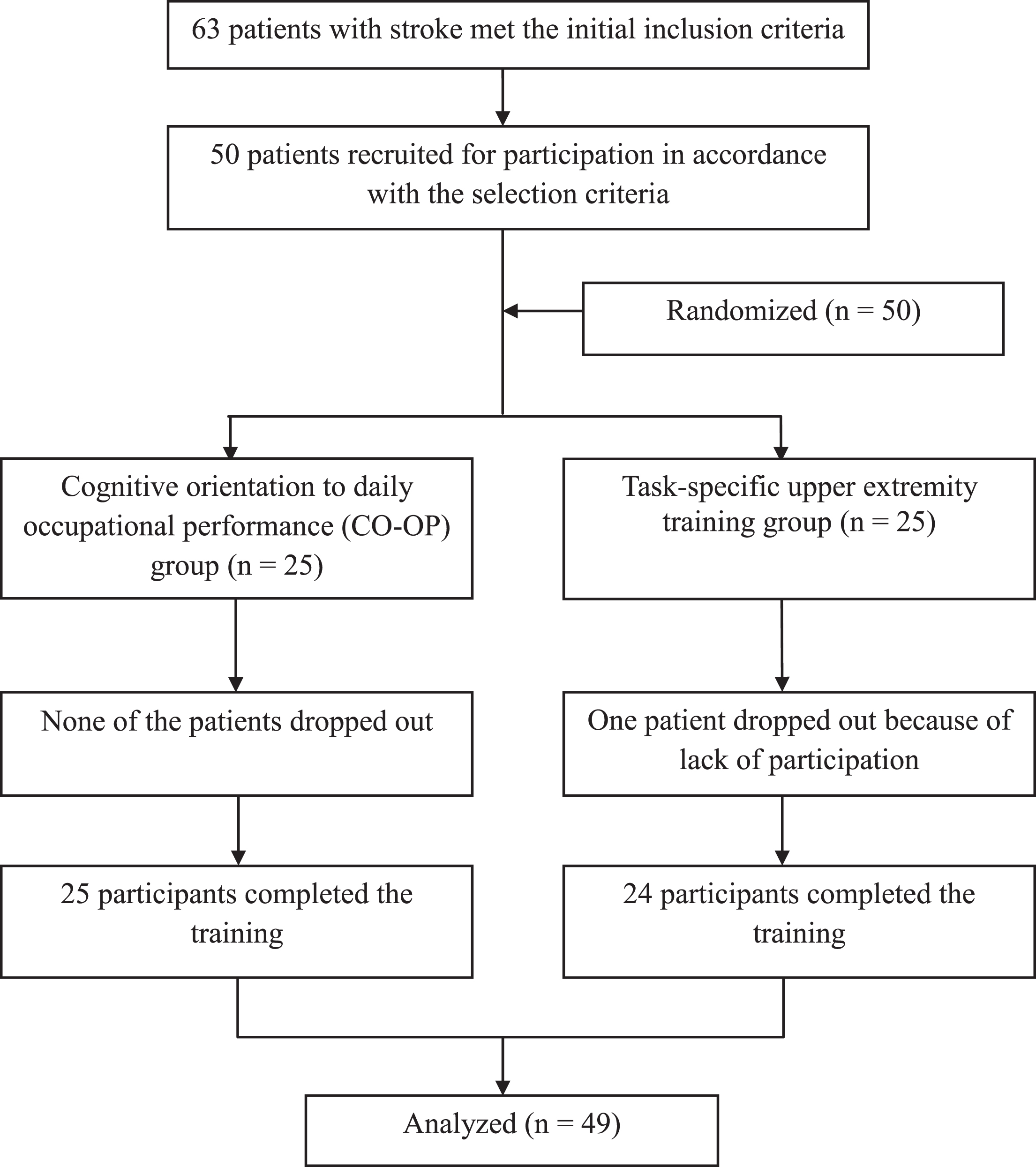
Flow of the study.
This study was to provide two different therapeutic interventions- the CO-OP approach and task-specific approach. The CO-OP approach consisted of two distinct phases, cognitive strategy of goal-plan-do-check and motor-based tasks in the repetitive action. The participants selected and designed to enable performance they need to, want to, or are expected to achieve independently as part of their daily activities. The participants and their therapists (one occupational therapist and one psychologist) worked together to recognize their problems or disabilities, discussed why the patients were unable to perform the selected activities, and designed a problem-solving approach to facilitate better performance in the self-selected activities. The patients then performed the self-selected activities repetitively, and their performances were evaluated by their therapists (Table 2).
Classification of self-selected occupational performance in the CO-OP group
Classification of self-selected occupational performance in the CO-OP group
ADL, activities of daily living; CO-OP, Cognitive Orientation to daily Occupational Performance.
The TUET involved performed goal-directed, repetitive, and self-selected activities related to the upper extremity. It was based on the examination of motor function and activity performance as indexed by the COPM score. The patient and therapist selected target tasks depending on the patient’s performance level on activities, and modified the task demands based on his/her limitations. After selecting the target tasks, the patient received repetitive, selected target tasks, 10 repetitions with a 1-minute rest period per task. The patient took a 3 minute break after performing a task in order to prevent fatigue. After completing 1 task, the patient moved to the next task on the self-selected target task list.
This study used four different outcome measures, all of which were collected at baseline and at the end of the treatment protocol. The instrument used in the present study was the Wolf Motor Function Test functional score (WMFT-F), which measures upper extremity motor ability through functional tasks. The COPM comprised the occupational performance problems experienced by the participants. The Box-and-Block Test (BBT) was used to identify gross manual dexterity, while the Community Integration Questionnaire (CIQ) was used to measure the community integration and social role limitations of the participants.
The Wolf Motor Function Test (WMFT) is a performance-based instrument that quantitatively measures upper extremity motor ability through timed and functional tasks for assessing the motor status of higher-functioning patients who had chronic stroke and traumatic brain injury. The original version of the WMFT was developed by Wolf, Lecraw, Barton, and Jann in 1989, and its widely used version consists of 17 items modified by Taub, Blanton, and McCullough from the UAB CI Therapy Research Group. The first 6 items involve timed functional tasks, items 7–14 are measures of strength, and the remaining 9 items are used for analyzing movement quality when completing various tasks. The tool uses a 6-point ordinal scale from 0 (does not attempt with the affected arm) to 5 (arm can move, or arm movement appears normal). The maximum score is 75 points, and lower scores are indicative of lower functioning levels. The WMFT should be performed as quickly as possible and was, therefore, truncated to 120 s (Morris, Uswatte, Crago, Cook, & Taub, 2001; Wolf et al., 2001). This study measured WMFT-F only for analyzing the therapeutic effects.
The COPM is a personalized, patient-specific instrument designed to identify the occupational performance problems experienced by him/her. It measures a person’s self-perceived occupational performance within three occupational performance areas, namely self-care, productivity, and leisure. During a semi-structured interview, the occupational therapist initiates the COPM process by engaging the clients in identifying daily occupations of importance that they want to do, need to do, or are expected to do but are unable to accomplish. The importance of each occupation is rated on a scale of 1 to 10 (10 being very important). Next, the participants prioritize a maximum of 5 most important occupations and rate their performance and satisfaction with their performance for each on a scale of 1 to 10 (a higher score reflected better performance or higher satisfaction). The mean COPM score was calculated by adding the performance or satisfaction scores for all the occupations and dividing this number by the number of prioritized occupations (Cup, Scholte op Reimer, Thijssen, & van Kuyk-Minis, 2003; Phipps & Richardson, 2007; Yang, Lin, Lee, & Chang, 2017).
The BBT assesses unilateral gross manual dexterity and is scored by counting the number of blocks carried over the partition from one compartment to the other during the 1-minute trial period. Participants are seated at a table, facing a rectangular box (2.5-cm colored wooden cubes) divided into 2 square compartments of equal dimension by means of a partition. To administer the test, the examiner is seated opposite the participants to observe test performance. The participant’s hand must cross over the partition for a point to be given, and blocks that drop or bounce out of the second compartment onto the floor are still rewarded with a point. Higher scores on the test indicate better gross manual dexterity (Chanubol et al., 2012; Platz et al., 2005; Slota, Enders, & Seo, 2014). This test was performed 3 times, and the mean of the 3 measurements was used for the statistical analysis.
The CIQ was developed by Barry Willer to provide a measure of individual integration and social role limitations in home and family life, social activity, and productive activity after a traumatic brain injury. The CIQ contains 15 items for assessing community integrations across 3 domains, including home integration (i.e., market, meal preparation, household activities, and finance; 5 items for 0–10 points), social integration (i.e., shopping, avocation, and going out; 6 items for 0–12 points), and productive activity (i.e., work, school and volunteer activity; 4 items for 0–7 points). Most items of the CIQ are scored in a scale of 0 to 2 points, with 2 points representing greater independence and community integration. The CIQ is a valid and reliable tool for assessing community integration of neurological disorders (Glenn, Goldstein, Selleck, Rotman, & Jacob, 2006; Tomaszewski & Mitrushina, 2016; Willer, Ottenbacher, & Coad, 1994).
Statistical analysis
The independent variables of this study were the CO-OP approach and TUET, and the dependent variables were WMFT functional score, COPM, BBT, and CIQ scores. This study collected the demographic characteristics of the participants, including information on stroke-related history. An independent t-test was used to analyze pretest differences in dependent variables between the two groups. An ANOVA was used to analyze differences in the pre-test and post-test values of the dependent variables between the two groups. And then, a receiver operating characteristic (ROC) curve was used to obtain the minimal clinically important difference (MCID) of WMFT-F, COPM, BBT, and CIQ scores. Optimal cutoff values were determined at the point of the greatest sensitivity (Sn) and specificity (Sp). The accuracy of the cut-off value was discriminated by the area under the curve (AUC) from the ROC curve. PASW version 18.0 (SPSS Inc., Chicago, USA) was used for all the statistical analyses. A p-value of <0.05 was considered statistically significant.
Results
Upper extremity function and community integration before training
We found no significant differences in the pre-test scores for any of the clinical measures between the groups (p > 0.05). In mean pre-test WMFT-F for CO-OP and TUET groups were 56.96 and 57.29, respectively. The mean pre-test COPM-P and COPM-S scores were 3.31 and 1.92, respectively, for the CO-OP group, and 2.71 and 1.94, respectively, for the TUET group. The mean pre-test BBT score for CO-OP and TUET groups were 22.30 and 31.06 respectively. The pre-test CIQ scores for the CO-OP and TUET groups were 6.28 and 5.79, respectively (Table 3).
Modulation of upper extremity function, postural balance, and community integration in the CO-OP and TUET groups (N = 49)
Modulation of upper extremity function, postural balance, and community integration in the CO-OP and TUET groups (N = 49)
Values are presented as mean±standard deviation unless otherwise indicated. CO-OP, Cognitive Orientation to daily Occupational Performance; TUET, Task-specific upper extremity training. WMFT, Wolf motor function test; COPM-P, Canadian Occupational Performance Measure–Performance; COPM-S, Canadian Occupational Performance Measure–Satisfaction; BBT, box-and-block test; CIQ, Community Integration Questionnaire. *significant difference pre-test vs. post-test CO-OP group. †significant difference pre-test vs. post-test TUET group. ‡significant difference between-group comparison.
Between-group comparison revealed a significantly higher increase in the mean WMFT-F, COPM-P, COPM-S and BBS scores after 4 weeks of training in the CO-OP group than in the TUET group (p < 0.05) (Table 3). The WMFT-F increased by 7.12 in the CO-OP group and 3.71 in the TUET group after training. The COPM-P score increased by 1.90 in the CO-OP group and 0.18 in the TUET group after training. The COPM-S score increased by 1.91 in the CO-OP group and 0.59 in the TUET group after training. Finally, the BBT score increased by 9.58 in the CO-OP group and 2.45 in TUET group after training. However, the increase CIQ score after training was not significantly different between the two groups (p > 0.05) (Table 3).
Minimal clinically important difference in the CO-OP and TUET groups
MCID revealed a significantly different in the WMFT-F, COPO-P, COPM-S and BBT after 4 weeks of training in the CO-OP group, but not TUET group. In the CO-OP group, the AUC of the ROC curves in WMFT-T, COPM-P, COPM-S, BBT, and CIQ was 0.740, 0.810, 0.871, 0.686, and 0.631 respectively. The Sn in WMFT-T, COPM-P, COPM-S, BBT, and CIQ was 0.680, 0.680, 0.720, 0.560, and 0.560, and the Sp in them was 0.680, 0.680, 0.840, 0.560, and 0.560 respectively. All of them indicate moderate accuracy (Table 4).
MCID estimates for WMFT-F, COPM-P, COPM-S, BBT and CIQ scores, AUC, Sn, and Sp
MCID estimates for WMFT-F, COPM-P, COPM-S, BBT and CIQ scores, AUC, Sn, and Sp
MCID, minimal clinically important difference; AUC, area under the curve; CI, confidence interval; Sn, sensitivity; Sp, specificity. CO-OP, Cognitive Orientation to daily Occupational Performance; TUET, Task-specific upper extremity training. WMFT, Wolf motor function test; COPM-P, Canadian Occupational Performance Measure–Performance; COPM-S, Canadian Occupational Performance Measure–Satisfaction; BBT, box-and-block test; CIQ, Community Integration Questionnaire.
In this study, we examined differences in the effects of the CO-OP approach and TUET on upper extremity function, community integration, and independence in patients with hemiparetic stroke. We found that the CO-OP approach to significantly greater therapeutic effects on functional activities and occupational performance than the TUET, although improvements in individual postural balance and social integration after training were not significantly different between the two groups.
Contemporary top-down approaches such as task-specific and cognitive interventions to improve the physical performance of stroke survivors focus on individuals’ post-stroke limitations in daily and functional activities and social integration and emphasize the role of problem solving in motor skill development (Jackman, Novak, & Lannin, 2014; O’Sullivan, et al., 2014). Concentrated and repetitive task-specific training methods such as constraint-induced movement therapy (CI therapy) are used to induce the utilization of the more affected upper extremity of patients with neurological diseases (Jackman, et al., 2014; O’Sullivan, et al., 2014). CI therapy applies a transfer package of adherence-enhancing behavioral methods, and constraining the more-affected upper extremity (Morris, Taub, & Mark, 2006; O’Sullivan, et al., 2014). CI therapy engages the patient in self-monitoring of target behaviors, problem-solving, behavioral contracting, and social support strategies (Morris, et al., 2006). The CO-OP approach focuses on improving functional activities in everyday life and consists of two comprehensive stages including a goal-setting stage based on the patient’s degree of occupational performance (Wolf, et al., 2016). The similarities between CI therapy and the CO-OP are repetitive training of target tasks used in every daily life situation and problem solving to identify obstacles and generate potential solutions. However, there are some differences between two approaches. The CI therapy constrains the more-affected upper extremity to induce intensive movement of the less-affected upper extremity, so the therapy involves unilateral manipulation. The CO-OP approach, on the other hand, can involve unilateral manipulation as well as bilateral movement if the patient selects the movement. Another main difference lies in the intensity of treatment in CI therapy and the CO-OP approach, because with CI therapy being an intensity practice of the more affected upper extremity for up to 6 hours a day, and the CO-OP approach regularly providing intervention sessions along with some homework (Mark & Taub, 2004). Our results demonstrate positive therapeutic effects of the CO-OP approach on upper extremity function, functional activities, and occupational performance for patients with stroke as in CI therapy, despite the protocol not involving intensive training.
Previous studies have provided evidence to support the use of cognitive interventions such as the CO-OP approach to supplement the limitations of the task-specific approach in improving functional performance in activities of daily living, education, work, leisure, and social participation among stroke survivors (Ahn et al., 2017; Henshaw, Polatajko, McEwen, Ryan, & Baum, 2011; Imms & Nott, 2012; McEwen, et al., 2015). We investigated the effects of the CO-OP approach on upper extremity function and social integration. The CO-OP group received repetitive, induced activities of self-selected goals for 4 weeks over, 20 sessions. The patients selected activities of daily living such as dressing, bathing and showering, feeding, and personal hygiene and grooming, and instrumental activities of daily living such as meal preparation, cleaning up, and home management and maintenance, with emphasis on individually meaningful occupational goal settings and application of a problem-solving strategy. After the CO-OP training, the patients showed greater improvement in their upper extremity function, occupational performance, and manual dexterity than those in the TUET group. This study provides two different therapeutic approaches, namely the CO-OP approach and TUET. The main differences between the two therapeutic approaches are that the CO-OP approach has a self-selected goal, has guided discovery-enabling principles, and allows for generalization and transfer steps (McEwen, et al., 2015).
Poulin and colleagues studied the feasibility and preliminary efficacy of the CO-OP approach and computerized executive function training for persons with stroke-related executive dysfunction. They reported that patients of the study expressed high levels of satisfaction with both interventions, and two groups showed large improvements in self and significant other-rated performance and satisfaction with performance on their goals immediately post-intervention as well as at follow-up (Poulin, Korner-Bitensky, Bherer, Lussier, & Dawson, 2017). A recent study by Skidmore et al. has reported the effects of global strategy training methods on apathy symptoms over the first 6 months after training. The study suggests several reasons for why global strategy training such as that involving goal-directed behavior, planning, self-monitoring, and problem solving may influence apathy symptoms in the acute phase after stroke. The study also reported that the incorporation of self-selected goals may enhance interest and motivation for goal-directed activities while the development of goal planning, self-monitoring, and problem-solving skills may promote activation and perseverance (Skidmore, Whyte, Butters, Terhorst, & Reynolds, 2015). In this study, the TUET group showed improvements in upper extremity function, performance and satisfaction of self-selected activities, and unilateral gross manual dexterity and social integration. However, the improvements in upper extremity function and occupational performance, except postural balance and social integration, were significantly higher in the CO-OP. Participants in the CO-OP group repeated self-selected, goal-directed behaviors with interest and motivation throughout the training period. Our results suggest that the interest and motivation among patients resulted in a significantly higher improvement in upper extremity function, performance and satisfaction of self-selected activities, and gross manual dexterity in the CO-OP group than in the TUET group. Our results also point to the presence of additional cognitive process in the CO-OP approach that may lead to more positive therapeutic effects on daily and functional activities than in the TUET group.
We have some limitation of the study. First, none of the authors attended any CO-OP workshops, although the second author, a psychologist, has professional knowledge related to taxonomic analysis of human movement. Second, the study did not measure therapeutic retention through follow-up test. Third, our study was not large enough to generalize our findings over a population, because only stroke survivors participated in this study. More studies recruiting patients with acute and chronic stroke exhibiting greater variation the types of self-selected activities must be conducted in order to increase our understanding in clinical rehabilitation settings.
Conclusions
We evaluated the comparative therapeutic effects of the CO-OP approach and the TUET on upper extremity function and performance of daily activities in patients with hemiparetic stroke. We found a significantly higher increase in the WMFT-F, COPM-P and COPM-S scores, but not BBT and CIQ scores in the CO-OP group than in the TUET group after training. Our results suggest that the CO-OP approach shows higher therapeutic potential for improvement in the performance of daily and functional activities as well as on community integration for patients with subacute stroke than task-specific upper extremity training.
Disclosure
The authors have no financial conflicts of interest.
Footnotes
Acknowledgments
This study was supported by research funds from Chosun University, 2016.