
Abstract
Purpose:
Patients with moderate-to-severe stroke-related upper limb impairment can benefit from repetitive robot-assisted training. However, predicting motor performance in these patients from baseline measurements, including robot-based parameters would help clinicians to provide optimal treatments for each individual.
Methods:
Forty-six patients with sub-acute stroke underwent a 16-session upper limb rehabilitation combining usual care and robotic therapy. Motor outcomes (Fugl-Meyer Assessment Upper Extremity (FMA) score) were retrospectively analysed and potential predictors of motor outcome (including baseline FMA scores, kinematics and number of repetitions performed in the first session etc.) were determined.
Results:
The 16-sessions upper limb combined training program led to significantly improved clinical outcomes (gains of 13.8±11.2 for total FMA score and 7.3±6.7 for FMA Shoulder/Elbow score). For the prediction model, time since stroke poorly explained the FMA total score (R2 < 35%). The model however found that time since stroke and initial value of FMA Shoulder/Elbow score were predictors of the FMA Shoulder/Elbow score: (R2 = 59.6%).
Conclusion:
This study found that clinical prediction of motor outcomes after moderate-to-severe upper-limb paresis is limited. However, initial proximal motor impairment severity predicted proximal motor performance. The value of baselines kinematics and of the number of repeated movements at initiation in the prediction would need further studies.
Introduction
The most common sequela of stroke is upper-limb paresis (Lawrence et al., 2001); approximately only one third of patients with stroke regain some hand dexterity within six months (Hendricks, Van Limbeek, Geurts, & Zwarts, 2002; Kwakkel & Kollen, 2007, 2013) to one year (Kong & Lee, 2013) after stroke.
Over the last decade, several studies have suggested that the pattern and the rate of motor recovery are unaffected by upper-limb therapy during the sub-acute phase of stroke (Byblow, Stinear, Barber, Petoe, & Ackerley, 2015; Krakauer, Carmichael, Corbett, & Wittenberg, 2012), and that spontaneous recovery follows a proportional recovery rule. This rule states that within 6 months, upper limb impairment resolves by a fixed proportion: 70% of each patient’s maximum possible improvement (Prabhakaran et al., 2008). These findings have, however, recently been challenged by other studies that found that the early prediction of recovery is limited by the naturally high variability of recovery in patients with severe impairment (Koh et al., 2015; Krakauer & Marshall, 2015; Winters, Van Wegen, Daffertshofer, & Kwakkel, 2015). Moreover, the results of a very recent study involving formal analyses and simulations suggested that the “proportional recovery model” is inflated (Hope et al., 2019).
The field of restorative neurorehabilitation has changed over the last 3 decades, becoming more evidence based. Results from animal experiments (Murphy & Corbett, 2009; Nudo, Milliken, Jenkins, & Merzenich, 1996) and human studies (Levy, Nichols, Schmalbrock, Keller, & Chakeres, 2001; Liepert, Graef, Uhde, Leidner, & Weiller, 2000; Takeuchi & Izumi, 2013) have shown that exercise-based programs can promote activity-dependent neural re-organization and that intense, highly repetitive and task-specific training can improve outcomes after an acute stroke (Buma, Kwakkel, & Ramsey, 2013; Bütefisch, Hummelsheim, Denzler, & Mauritz, 1995; Cooke, Mares, Clark, Tallis, & Pomeroy, 2010; Kwakkel et al., 2004; Kwakkel, Wagenaar, Twisk, Lankhorst, & Koetsier, 1999). Moreover, there appears to be a dose-response relationship between the amount of rehabilitation administered and motor outcomes (Han, Wang, Meng, & Qi, 2013; Lohse, Lang, & Boyd, 2014).
Advanced robotic systems meet evidence-based-practice guidelines for the need to develop methods and strategies to deliver intensive, repetitive, reproducible and quantifiable training for the paretic limb. Furthermore, these systems provide objective measurements of kinematic metrics that can be used to assess motor performance over time (Gilliaux et al., 2014; Krebs et al., 1999; Zollo et al., 2011). Kinematic measurements provide additional information to clinical assessments as they measure specific, objective movement characteristics, such as accuracy and smoothness, that have been shown to be sensitive to change (Duret, Courtial, & Grosmaire, 2016). Since 1997, several studies have reported that robotic therapy reduces upper-limb motor impairment in all phases of recovery: acute, subacute (Aisen, Krebs, Hogan, Mcdowell, & Volpe, 1997; Masiero, Armani, Ferlini, Rosati, & Rossi, 2014; Sale et al., 2014; Volpe et al., 2000) and chronic phases (Klamroth-Marganska et al., 2014; Lo et al., 2010; Lum, Burgar, Shor, Majmundar, & Van der Loos, 2002). Robotic therapy has also been shown to be particularly useful for the rehabilitation of individuals with severe impairment (Hesse et al., 2005; Volpe et al., 2000). It provides a means of intensive training for this group for whom intensive practice is otherwise difficult to implement (Duret, Hutin, Lehenaff, & Gracies, 2015).
Several studies have examined potential predictors of upper-limb motor recovery following stroke, demonstrating that the best predictor of upper limb recovery following stroke is the initial severity of the motor impairment (Coupar, Pollock, Rowe, Weir, & Langhorne, 2012; Kwakkel, Kollen, Van der Grond, & Prevo, 2003; Stinear et al., 2007). However, in order to refine neurorehabilitation methods based on evidence-based practice, a large number of baseline variables are needed to accurately predict the effects of specific types of rehabilitation (training modalities, systems targeted etc.) in identified subgroups of patients with stroke (based on initial motor impairment, associated symptoms etc.).
The aim of this study, therefore, was to examine a range of variables in order to identify reliable indictors of upper-limb motor performance following an intensive rehabilitation program that combined 16 sessions of robot-assisted training (3 days/week) with usual care during the sub-acute phase in patients with moderate-to-severe upper-limb paresis following stroke.
Materials and methods
Subjects
Forty-six patients who underwent rehabilitation at the Neurorehabilitation unit of “Les Trois Soleils” Rehabilitation Centre (Boissise Le Roi, France) between October 2010 and October 2018 were retrospectively included in this study. Data from patients who fulfilled the following inclusion criteria were included: over 18 years old, with moderate-to severe upper-limb paresis defined as a Fugl-Meyer Assessment (FMA) score for the upper-limb of less than 35 points at the onset of the therapy, in the acute/sub-acute phase (less than 6 months post-stroke) of a first-ever stroke confirmed on CT scan or MRI, and with sufficient understanding to participate in rehabilitation exercises. The clinical characteristics of the patients are summarized in Table 1. All patients included had participated in an intensive upper-limb rehabilitation program for stroke patients with moderate to severe motor impairments which involved robot-assisted therapy sessions.
Patient characteristics; Results are expressed as means (SD); H, haemorrhagic; I, ischemic
Patient characteristics; Results are expressed as means (SD); H, haemorrhagic; I, ischemic
This study was conducted in accordance with the Declaration of Helsinki (2008), Good Clinical Practice guidelines and local regulatory requirements. This retrospective study used data collected during routine care and therefore did not require patient consent to be obtained.
The InMotion 2.0 Arm robot (Interactive Motion Technologies, Inc., Watertown, MA) was used to provide the robotic training. This manipulator, a commercial version of the MIT Manus device (Krebs et al., 2004), has two active translational degrees-of-freedom to assist shoulder (flexion/extension) and elbow (flexion/extension) movements in the horizontal plane. It uses an interactive system with a low mechanical inertia and a performance-based algorithm to emphasize motor recovery and/or motor performance in individuals with CNS (Central Nervous System) damage. This robot not only provided repetitive, goal-directed movement-based therapy but it also used hand trajectory sensors to collect kinematic data.
Clinical evaluations
Upper-limb motor impairment was measured by skilled evaluators from the therapy team both before and after the training using total upper-limb and subcomponent Fugl-Meyer Assessment (FMA) scale scores (Fugl-Meyer, Jääskö, Leyman, Olsson, & Steglind, 1975; Hamrin & Lindmark, 1988). The FMA scale is an impairment-based measurement scale which provides reliable, validated and responsive measures of upper-limb impairment in individuals with subacute stroke (Lin, Huang, Hsieh, & Wu, 2009). It is widely used in studies of robotic rehabilitation (Sivan, O’Connor, Makower, Levesley, & Bhakta, 2011). The FMA scale individually measures the capacity of the shoulder, elbow, wrist and hand to carry out selective movements. The performance of each item is rated on a 3-point ordinal scale (0, 1, 2) with a maximum score of 66 points including 36 points for Shoulder/Elbow FMA subscale.
A minimum clinically important difference (MCID) has been determined for the FMA scale and subscales, showing that an improvement of more than 9 points (for FMA total scale) or 5 (for Shoulder/Elbow FMA scale) in the subacute phase of stroke constitutes a difference that improves daily living (Narayan Arya, Verma, & Garg, 2011). We therefore sought to determine if baseline FMA variables could predict a MCID outcome.
Three associated stroke-symptoms were also evaluated as it was considered they could impact the outcome of physical rehabilitation, using a binary score. The first measured overall sensation in the arm (significant impairment = 1 and no significant impairment = 0). The second associated symptom, unilateral spatial neglect (USN), was evaluated using the Azouvi method (at least one sign = 1 and no signs = 0) (Azouvi et al., 2006). The third associated symptom, aphasia, was evaluated by speech and language therapists using the MT86β Aphasia Battery (presence of impairment, score = 1 and no impairment = 0) (Nespoulous et al., 1992).
Robot-based outcome measures
All patients underwent upper-limb kinematic assessments both before (baseline) and within the few days following the last training session. The assessment involved the patient performing 80 point-to-point reaching movements towards 8 visual targets, each 14 cm from the centre of the targets. These movements were not assisted by the robotic device. From these data, four kinematic measures were computed (Krebs et al., 2003) (Fig. 1):

InMotion 2.0 Arm robotic device; a) Patient using the robotic system; b) Interface for point-to-point reaching movements task.
a) mean movement speed (cm.s–1); b) movement path error, which was the mean deviation from the straight line (cm); c) active range of motion, calculated as the average distance between the movement end point and the peripheral target (cm) and d) a smoothness metric, calculated from the average speed divided by peak speed.
The intensive rehabilitation therapy period lasted for 5 weeks (mean 4.6±1.4).
Standard upper-limb rehabilitation consisted of one-hour occupational therapy sessions, 5 times per week. Each session involved passive stretches of the paretic limb, active assisted movements, reaching movements with or without elbow support as well as grasp-and-release tasks tailored to each patient’s abilities.
All patients received 16 robot assisted sessions in total, on average 4 times per week (3.7±0.9). These sessions were provided in addition to the standard rehabilitation care program. During the sessions, patients performed series of 320 assist-as-needed goal-directed movements (adaptive mode) towards 8 targets that were displayed on a monitor in 8 compass directions. The patient was encouraged to perform as many accurate movements as possible in the allocated time (about 45 minutes) by a trained therapist who supervised the session. The number of movements performed during the first, eighth and sixteenth sessions, and the total number for all the sessions were recorded for analysis.
Statistical analysis
Pre-and post-treatment values of the clinical outcome measures and the kinematic variables were compared using a Wilcoxon signed-rank test (α= 0.05). The capacity of selected baseline variables (see Table 3 for details) to predict change in FMA scores was assessed by multiple regression. We also assessed the capacity of the same variables to predict change in FMA Shoulder/Elbow scores using multiple regression. The capacity of baseline measures to predict attainment of the MCID (a FMA total score increase of at least 9 points or 5 points for Shoulder/Elbow FMA score) was assessed by logistic regression.
Results
Baseline characteristics, motor and kinematic outcomes
Pre-training mean FMA total score was 18.2±9.4. 24 patients had sensory impairments, 6 patients had signs of unilateral neglect and 14 had aphasia. All FMA scores and sub-scores improved after the training. There was an increase of 13.8±11.2 points in FMA total score during the training period (see Table 2).
Clinical measures of motor outcome; Results are expressed as means±SD; FMA, Fugl-Meyer Upper Extremity Assessment
Clinical measures of motor outcome; Results are expressed as means±SD; FMA, Fugl-Meyer Upper Extremity Assessment
*Statistically significant difference between baseline and post-therapy (p value <0.001).
The number of movements increased significantly from 629±298 to 933±344 between the first and the last sessions, and all kinematic parameters improved significantly (see Fig. 2).
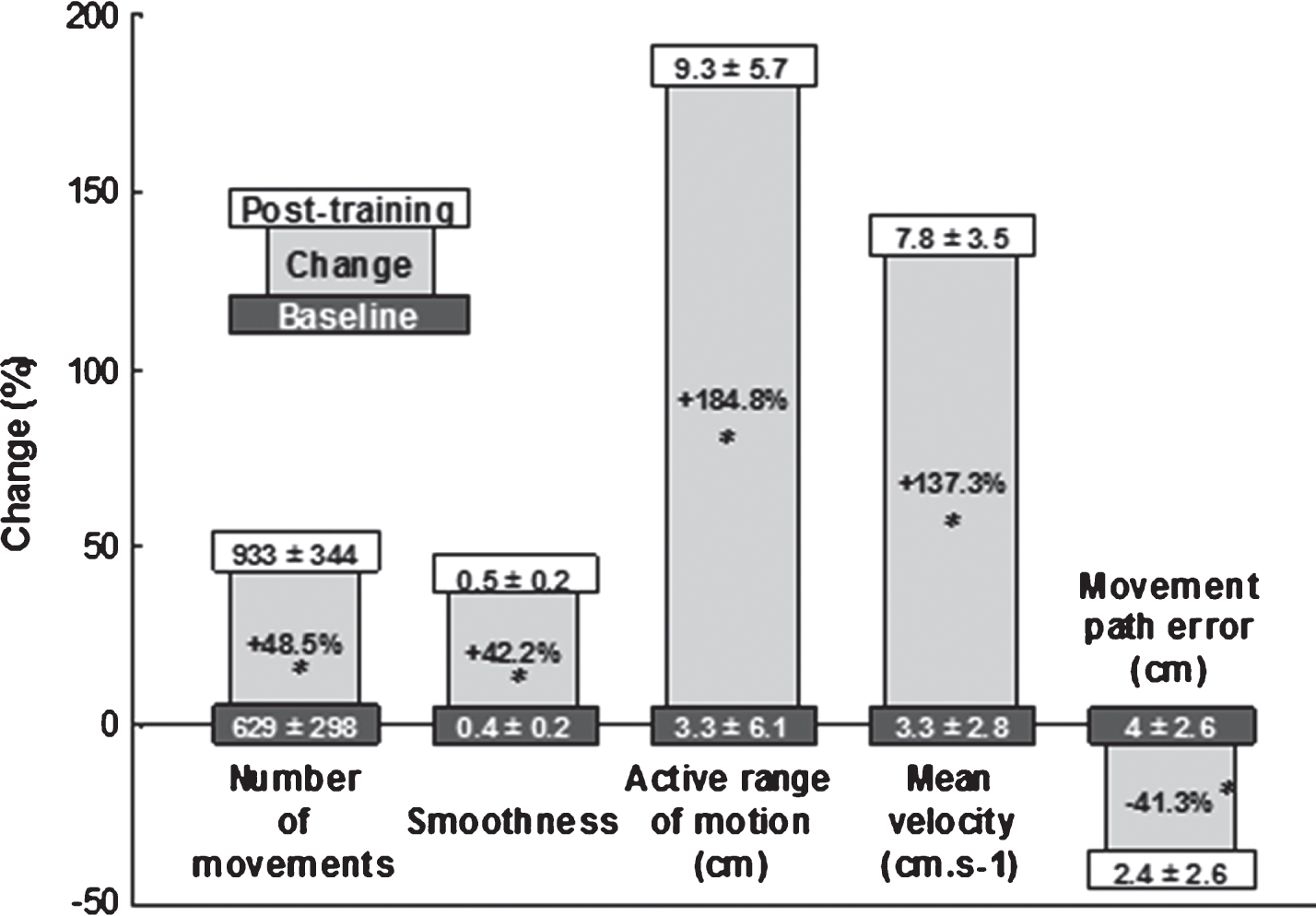
Pre/post kinematic measures; Results are expressed as means±SD (*: statistically significant difference between baseline and post-therapy (p-value <0.01)).
Clinical and kinematic predictors of motor changes
Time since stroke was the only predictor of the FMA total score (34.7% of variance). For the FMA Shoulder/Elbow score, which are the joints that are the most targeted by the robotic therapy, two predictors were determined by the model, accounting for 59.6% of the variance: “time since stroke” and initial value of FMA Shoulder/Elbow score (Table 3).
Predictors of Shoulder-Elbow Fugl Meyer Assessment score; Adjusted R2 was used to account for multicollinearity
Predictors of Shoulder-Elbow Fugl Meyer Assessment score; Adjusted R2 was used to account for multicollinearity
In contrast, the regression analysis did not indicate that any other clinical or kinematic parameter contributed significantly to the variance of change in FMA total score or FMA Shoulder/Elbow score.
The MCID of the FMA total score was attained in 25 patients and the MCID of the FMA Shoulder/Elbow score in 27 patients following the robot-enhanced rehabilitation programme, however none of the variables tested significantly predicted this achievement.
Discussion
To our knowledge, this is the first study in patients with moderate-to-severe, stroke-related upper-limb impairment to consider motion kinematics, the number of movements performed and associated symptoms (loss of sensation, USN and aphasia) as potential predictors of motor outcome after an intensive rehabilitation protocol that combined routine and robotic therapy. We found that only the time since the stroke occurred was a significant predictor of outcome (as indicated by the change in FMA total score). However, time since stroke at initiation of robotic training and the initial proximal motor impairment were predictors of FMA Shoulder/Elbow score after the training. The number of movements performed during the first session, baseline movement path error and active range of motion were close to significance as predictors. No variables predicted achievement of the MCID for the FMA total score.
Rate of motor recovery
The present study found that intensive, highly repetitive training was associated with a magnitude of change in FMA total score greater than that which would normally be expected or seen in subacute stroke patients with moderate-to-severe upper-limb paresis (initial FMA score lower than 35 points) (Duncan, Min Lai, & Keighley, 2000; Jorgensen, 1996; Lee et al., 2015). Other studies have reported that upper-limb recovery is relatively rapid during the first 4 weeks post-stroke, after which improvements may continue, but at a slower pace, between the 2nd and 3rd months (Duncan et al., 2000; Lee, Hsieh, Wu, Lin, & Chen, 2015; Verheyden et al., 2008). This time-course is similar for subgroups with severe impairment, who may continue to recover for up to 6 months (Duncan et al., 2000; Hendricks et al., 2002; Mirbagheri & Rymer, 2008). This study confirmed previous results from our own group that showed that significant motor improvement occurred following an intensive robot-assisted rehabilitation program in patients in the late sub-acute phase of stroke (Pila et al., 2017).
Predictor of motor changes
None of the patient characteristics, including motor impairment at initiation of robotic training, predicted change in FMA total score following therapy in this sample of 46 patients with moderate-to-severe upper-limb paresis. However, our results indicated that the initial severity of the proximal motor impairment was a significant predictor of proximal motor performance after Shoulder/Elbow robot-assisted training. This latter finding is consistent with some published studies, which found that the initial severity of the motor impairment was the best predictor of motor outcome at three or six months (see review by Coupar et al., 2012). This suggests that the change in FMA proximal score found after the combined intensive therapy is the result of both spontaneous recovery processes and therapy-related effects, which could be confounding factors for the prediction of recovery in this very early phase after stroke. This result also indicated that most improvement occurred in specifically-trained limb segments as seen previously in Pila et al. (Pila et al., 2017).
However, our results contrast with several other studies that showed that the motor recovery of patients with moderate-to-severe upper-limb paresis is so widely variable that the prediction of outcome from clinical measurements is difficult (Byblow et al., 2015; Koh et al., 2015). They also contrast with a study that showed that proportional recovery models did not accurately predict arm recovery following severe motor impairment after stroke (Prabhakaran et al., 2008). However, in a very recent study, Hope et al. argued that the empirical support for the proportional recovery model is weaker than previously reported (Hope et al., 2019).
With regard to intensive, robot-assisted therapy, previous researches have indicated that the best predictor of motor outcomes is initial motor ability in the distal part of the affected upper-limb (Franceschini et al., 2018; Huang et al., 2014; Lin et al., 2009). However, in the present study the wrist-hand FMA sub-score did not significantly predict outcome (measured by total FMA score) at the end of the intensive therapy. We propose that this difference could be attributed to a lesser severity of impairment in the participants in those other studies (mild to moderate vs severe in our study). Those patients were able to carry out more functional evaluations, such as the Box and Block Test, on which the predictor calculations were based (Franceschini et al., 2018; Huang et al., 2014).
One interesting finding in the current study that has not been reported elsewhere in the literature was the statistical trend that might suggest an association between the number of movements performed during the first therapy session and the observed change in FMA score. As the number of movements is an easy measure to obtain during robotic therapy since it is recorded automatically, this data may help clinicians to select those patients who are more likely to benefit from robotic training.
Another important result from the present study is the confirmation of Horn et al.’s finding that the shortest possible time between stroke onset and initiation of rehabilitation most positively impacts motor outcomes (Horn et al., 2005).
In line with other work from our own group (Duret, Hutin, Lehenaff, & Gracies, 2015), motor outcomes after therapy were not found to be correlated with associated symptoms of stroke such as aphasia and USN, confirming the suitability of robotic rehabilitation therapy for a broad range of patients with sub-acute stroke. These findings differ from the results of Nijboer et al. who found a negative impact of USN on upper limb motor recovery in the first 10 weeks after stroke (Nijboer, Kollen, & Kwakkel, 2014) as well as results from Gialanella et al. who found that language disabilities were negative factors for functional outcomes (Gialanella, Bertolinelli, Lissi, & Prometti, 2011).
None of the kinematic measures significantly predicted motor performance after the robot-assisted therapy if we consider the FMA total score. However, there was a statistical trend between both baseline movement accuracy (path error) and active range of motion and the change in FMA Shoulder/Elbow score. This latter result was not surprising since kinematic measures have previously been shown to be correlated with clinical measures of motor outcome (Duret et al., 2016) and sensitive to changes in patient performance (Alt Murphy, Willén, & Sunnerhagen, 2013).
Prediction of MCID
None of the baseline clinical or kinematic measurement variables were able to predict achievement of the MCID. In other words, it was impossible to identify patients who would have significantly benefited from the intensive robot therapy based solely on their clinical and kinematic variables at the start of the study. It is possible that other clinical assessments would have provided a different result: Hsieh et al., for example, found that patients with stroke who had greater manual dexterity measured by the box-and-blocks test, but not the FMA distal score, had a higher probability of achieving clinically significant motor and functional outcomes after robotic therapy (Hsieh et al., 2014). These findings suggest that future work in this area should evaluate a wider range of clinical assessments in order to identify which particular assessments would act as predictors of motor therapy outcome. It is possible that predictive assessments might vary depending on the particular clinical characteristics of different sub-groups of patients with stroke.
Treatment Dose Effects
In the present study, the treatment dose administered during robotic sessions in terms of the number of movements performed during each 45-minute session was recorded automatically. On average, participants performed more than 600 repeated movements during the first session and over 900 movements during the last session. This number is consistent with the number of movements reported in other studies of robotic therapy (Duret, Courtial, Grosmaire, & Hutin, 2015; Pila et al., 2017).
Although there is currently not a recommended “number of movements” needed to achieve motor recovery, it seems likely that there would be a “threshold movement-dose” for rehabilitation to effectively activate endogenous recovery processes, as has been demonstrated in animal models (Jeffers et al., 2018; MacLellan et al., 2011). We would argue that this threshold figure is probably greater than 300 or 400 movements per session and that the number of movements currently delivered in typical human rehabilitation paradigms is normally far below this requirement (Lang et al., 2009). Indeed Lang et al. demonstrated that there was no evidence of a dose-response effect between 100, 200 and 300 movements performed during training sessions (Lang et al., 2016). Under-dosed therapy in terms of the number of movements performed could explain the negative results of many studies investigating the effects of so-called “intensive” therapy on upper-limb motor outcomes. This is probably the case in the study by Lang et al. (Lang et al., 2016), as well as the study by Winstein et al, who reported only session duration without any details regarding the number of movements achieved or the modalities used to perform the movements (Winstein et al., 2016).
It is therefore important that future studies into intensive therapy programs should report both the number and modality of movements carried out during the sessions, particularly since data from the present study revealed a statistical trend existed between the number of movements practiced during the first therapy session and motor outcomes. Unfortunately, despite the large number of repeated movements performed by participants, this study did not address the issue of a dose-effect relationship which should be the focus of future studies (Krakauer et al., 2012).
Study limitations
It should be noted that the study was retrospective and thus constrained by the dataset available. It was also uncontrolled. The kinematic evaluations were carried out on a planar robotic device, in 2D space. This may not be representative of movement kinematics in 3D and may have affected the predictive value of these parameters.
Nevertheless, we believe that the findings present a valuable record of a well-documented intensive training programme undertaken in patients with subacute, severe stroke. This study provided insights regarding potential predictors (as well as areas for future study) of motor outcome after intensive movement-based therapy.
Conclusion
This study found that the clinical prediction of motor outcomes after moderate-to-severe upper-limb paresis is still of limited accuracy and that baseline kinematics do not provide added value to the clinical measures that are currently routinely recorded. However, the initial severity of the proximal motor impairment was a significant predictor of proximal motor performance after a Shoulder/Elbow robot-assisted training, a finding which might help clinicians to select patients with moderate-to-severe impairment who are more likely to benefit from robotic therapy. The number of movements performed during the first session of robotic therapy as well as some robot-based kinematics (accuracy and active range of motion) might also be helpful to enhance selection in this sub-group of patients. Further work is required to elucidate the variables that will more accurately predict motor recovery in patients with severe stroke-related upper-limb impairment. In the meantime, because motor outcomes do not depend on routinely measured clinical parameters and, as a result of the observed changes in FMA total scores recorded in this study, we recommend that intensive rehabilitation should be provided for all patients with severe stroke-related impairment, especially if they are able to perform at least 400 movements in the first session. Further studies should explore the critical issue of a “minimal threshold movement-dose”.
Declaration of conflicting interests
The authors have no conflict of interest to declare, or any financial or other interest in the manufacturer or distributor of the device used in the present study.
Funding
This research received no specific grant.
Footnotes
Acknowledgments
We are grateful to the team of therapists at “Les Trois Soleils” hospital for their excellent work with the patients. We would also like to thank Jennifer Dandrea Palethorpe and Johanna Robertson for English language improvement.