
Abstract
Background:
Transcranial direct current stimulation (tDCS) is a promising tool for stroke rehabilitation. Yet, so far, results from the available clinical trials are inconclusive.
Objectives:
The primary objective of the present work was to test the efficacy of multiple sessions of tDCS combined with a highly standardized and progressive resistance training program of the affected upper limb in individuals in the chronic phase of recovery after a stroke. Secondary objectives were to test the safety and tolerability of these combined interventions.
Methods:
This two-arm parallel pilot trial recruited participants that were ≥18 years old, community-dwelling, and had sustained a supratentorial stroke ≥6 months prior to the study. They were allocated using a stratified randomization into two groups: 1) real tDCS + resistance training and 2) sham tDCS + resistance training. The resistance training program targeted the affected upper limb and consisted in 60 minutes of exercises, 3 times/week over 4 weeks. During each session, participants received either real- or sham-tDCS, using a bi-hemispheric montage for the first 20 minutes, and were blinded to the tDCS intervention. Outcome measures of clinical efficacy (Fugl-Meyer Assessment, Box and Block Test, Wolf Motor Function Test, grip strength, modified Ashworth scale and Motor Activity Log) were assessed by a blinded evaluator before and after the 4-week training program. Safety and tolerability were evaluated, respectively, by the number and characteristics of tDCS adverse events and dropout rates with their reasons.
Results:
From the 147 individuals screened for eligibility, 14 participants (68.9±10.0 years old; 70.9±57.6 months post-stroke) met the selection criteria and were allocated to real-tDCS (n = 7) or sham-tDCS (n = 7) groups. Both groups improved on the clinical outcome measures, but these changes were not significantly different between groups (p > 0.17). No dropout occurred throughout the study. Participants frequently reported mild skin tingling during the administration of both real- and sham-tDCS, and no group difference was noted for its frequency and intensity (p > 0.38). One participant having received real-tDCS complained about a mild skin burning sensation after two sessions. The a priori sample size analysis performed on the Fugl-Meyer Assessment scores revealed that 56 participants would be required in a future clinical trial to reach 80% power at a significance level of 0.05.
Conclusions:
In this pilot study, repeated sessions of bi-hemispheric tDCS coupled with resistance training were found safe and tolerable for individuals at the chronic phase post-stroke. However, the use of tDCS did not result in additional sensorimotor improvements when compared to sham-tDCS. Further research is needed to better assess the clinical benefits of combining non-invasive transcranial stimulation with rehabilitation after a stroke.
Keywords
Introduction
Stroke is one of the leading causes of physical disability world-wide (Krishnamurthi et al., 2015). Most survivors present chronic sensorimotor deficits that affect their functional independence and quality of life (Mayo, Wood-Dauphinee, Cote, Durcan, & Carlton, 2002). In particular, upper limb weakness (i.e. muscle paresis (Gracies, 2005)) can have devastating effects on day-to-day activities, work-related tasks, and social participation (Ada, O’Dwyer, & O’Neill, 2006; Kamper, Fischer, Cruz, & Rymer, 2006; Mercier & Bourbonnais, 2004). Progressive resistance training (PRT) is a core component of Canadian best practice guidelines for stroke rehabilitation (Hebert et al., 2016), and has been shown to be effective at improving muscle strength, physical fitness, motor function and independence in functional tasks (Ada, Dorsch, & Canning, 2006; Bohannon, 2007; Morris, Dodd, & Morris, 2004). Despite these lines of evidence, the impact of PRT has been shown to vary greatly across individuals (Harris & Eng, 2010; Patten, Lexell, & Brown, 2004), knowing that the potential for sensorimotor recovery of each person who had a stroke depends on the integrity of motor pathways and the remaining ability of the central nervous system (CNS) to undergo plastic changes in response to training (Cramer et al., 2007; Koski, Mernar, & Dobkin, 2004; Milot et al., 2014).
In response to rehabilitation after a stroke, brain plasticity occurs in distributed networks within the CNS. Human and animal models of stroke demonstrated that the primary motor cortex (M1) plays a key role in the recovery of motor functions (Arya, Pandian, Verma, & Garg, 2011; Beaulieu & Milot, 2017; Cramer & Riley, 2008; Grefkes & Ward, 2014; Xerri, Zennou-Azogui, Sadlaoud, & Sauvajon, 2014). In the past decade or so, the advent of non-invasive brain stimulators enabled researchers to experimentally modulate M1’s excitability with the goal of increasing the potential for neuroplasticity and sensorimotor recovery post-stroke (Braun et al., 2016; Di Pino et al., 2014; Klomjai et al., 2015). Transcranial direct current stimulation (tDCS) represents a safe, low-cost, and accessible neuromodulation method that received much attention in the past years (Elsner, Kwakkel, Kugler, & Mehrholz, 2017; Lefaucheur, 2016; Marquez, van Vliet, McElduff, Lagopoulos, & Parsons, 2015a). During tDCS, a constant electrical current of low amplitude is delivered to the scalp through a pair of soaked electrodes, which modulates the membrane potential of superficial cortical neurons without causing action potentials (Lefaucheur et al., 2017). After a short period of stimulation (usually less than 20 minutes), tDCS induces transient excitability changes, up to 90 minutes, in neurons under the electrodes (Lefaucheur et al., 2017). In general, excitation occurs under the anode and inhibition under the cathode, through long-term potentiation and long-term depression synaptic mechanisms (see reviews and guidelines for more details (Braun et al., 2016; Di Pino et al., 2014; Elsner et al., 2017; Klomjai et al., 2015; Lefaucheur, 2016; Lefaucheur et al., 2017; Marquez et al., 2015a)). Based on these observations, different tDCS protocols coupled with various motor training interventions have been applied in stroke survivors to improve sensorimotor recovery. In general, tDCS protocols are based on a particular model of maladaptive brain plasticity post-stroke, named “interhemispheric competition” (Nowak et al., 2009). This model postulates that stroke often translates into an unbalanced excitability between the lesioned (hypoactive) and unlesioned (hyperactive) hemispheres (Nowak et al., 2009; Perez & Cohen, 2009; Xerri et al., 2014). Based on this model, inhibiting the unlesioned primary motor cortex (M1) with transcranial stimulation should result in sensorimotor improvements, because the lesioned M1 is “released” from an exaggerated interhemispheric inhibitory influence from the unlesioned M1. The bilateral tDCS montage was specifically designed to simultaneously upregulate and downregulate the lesioned and unlesioned M1, respectively. Indeed, the excitatory anode is placed over the lesioned M1 and the inhibitory cathode over the unlesioned M1, hence resulting in plastic changes toward an overall re-balancing of interhemispheric activity between both primary motor cortices (Lefaucheur et al., 2017).
Recent systematic reviews and meta-analyses were realized on the several small clinical trials having tested the efficacy of tDCS coupled with motor training on sensorimotor function in stroke populations, but so far, the results are inconclusive. While some observed small to moderate levels of evidence in favor of real-tDCS versus sham-tDCS, others failed to detect superior effects of real-tDCS (cf. reviews on the topic (Di Pino et al., 2014; Elsner et al., 2017; Marquez et al., 2015a)). Conclusions are limited by the great heterogeneity across studies in terms of stroke population characteristics, methodological procedures, outcome measures, and interventions delivered. In particular, it was raised that the features of the motor training interventions are usually not standardized, hence increasing the risk of providing different training regimens between real-tDCS and control groups (Klomjai et al., 2015). Thus, further randomized controlled trials using better standardized procedures are still required to help determine the optimal tDCS parameters and protocols to use in combination with relevant motor training interventions to potentiate sensorimotor function post-stroke.
Given the clinical efficacy, feasibility and high standardization of PRT protocols and the potential of additive after-effects of tDCS over the motor cortex, it seems logical that the combination of PRT and tDCS over multiple sessions could lead to greater improvements of upper limb motor function. To the best of our knowledge, none of the previous studies mentioned above investigated the clinical interest of using this particular combination of interventions after a stroke, even though PRT is one of the recommended type of intervention to support sensorimotor recovery post-stroke (Hebert et al., 2016). Therefore, the main objective of the present pilot study was to test the efficacy of multiple sessions of tDCS combined to a 4-week PRT program of the affected upper limb in individuals in the chronic phase of recovery after a stroke. Moreover, secondary objectives were to test the safety (adverse events) and tolerability (dropout rates) of tDCS + PRT interventions. Based on the literature, we hypothesized that the combination of real-tDCS with PRT would represent a safe and tolerable method resulting in greater clinical efficacy than sham-tDCS combined with PRT.
Methods
This two-arm parallel pilot randomized controlled trial, realized in accordance to CONSORT statement for randomized pilot and feasibility trials (Eldridge et al., 2016), took place in Sherbrooke (Canada) from May 2015 to September 2017. No change to the methods occurred after pilot trial commencement.
Subjects
To be included in the study, individuals had to meet the following entry criteria: (i) aged 18 years old and up; (ii) supratentorial stroke >6 months (i.e. chronic phase) prior to study entry; (iii) level of sensorimotor recovery at the affected upper limb ≥35/66 on the Fugl-Meyer Stroke Assessment [FMA] scale (Fugl-Meyer, Jaasko, Leyman, Olsson, & Steglind, 1975). Subjects were excluded if presenting with: (i) important resistance to passive stretching in the affected shoulder extensors, elbows flexors, wrist flexors or finger flexors (modified Ashworth scale score >3 (Bohannon & Smith, 1987; Katz, Rovai, Brait, & Rymer, 1992)); (ii) major somatosensory deficit (revised Nottingham Sensory Assessment score ≤25/34 (Lincoln, Jackson, & Adams, 1998)); (iii) unilateral spatial neglect (>70% of unshaded lines on the Line Cancellation Test) (Albert, 1973); (iv) pain intensity at the affected upper limb ≥4/10 on the Visual Analog Pain Scale (Boonstra, Schiphorst Preuper, Balk, & Stewart, 2014); (v) apraxia (score >2.5 on the Alexander Test) (Alexander, Baker, Naeser, Kaplan, & Palumbo, 1992); (vi) neurological disorder other than a stroke; (vii) concomitant orthopaedic problems at the affected upper limb; (viii) attention or comprehension deficits (score ≥1 [question #1] or score of 3 [question #9] on the NIH Stroke scale) (Brott et al., 1989) and (ix) any contraindication to transcranial magnetic stimulation (TMS; listed in (Rossi, Hallett, Rossini, & Pascual-Leone, 2009)) and/or tDCS (Nitsche et al., 2003). Potential participants were first screened based on their medical records from the local health and social services center (CIUSSS de-l’Estrie-CHUS) and contacted by phone to verify their interest and eligibility. One week before the beginning of the intervention, recruited subjects were invited to our research laboratory to complete the baseline clinical evaluation (described below). Then, subjects were stratified based on their baseline FMA score into three strata: 35–45/66, 46–55/66 and ≥56/66. Within each FMA stratum, a blocked randomization, with a block size of 4, was used to randomize the subjects into one of the two tDCS groups (allocation ratio of 1:1 between groups): 1) real-tDCS + PRT program or 2) sham-tDCS + PRT program. The randomization procedure was performed using a computerized program by a statistician external to the project, and transmitted to the principal investigator (MH Milot) in the form of an encrypted electronic file. Only the principal investigator had access to the file, and informed the trained therapist about the participant’s allocation prior to the first intervention session. The person that enrolled participants did not have access to the allocation sequence. This project was conducted in accordance with the Declaration of Helsinki and approved by the CIUSSS de-l’Estrie-CHUS ethics board and all subjects signed a written consent form prior to their participation.
Efficacy-related outcome measures
One week before and after the 4-week PRT program combined with real- or sham-tDCS, clinical assessments were performed in our research laboratory by a blinded trained evaluator.
Clinical assessment
For the clinical assessment, the evaluator gathered sociodemographic data as well as clinical measures of the affected upper limb. The primary clinical outcome measure was the change in the upper limb motor score of the FMA (normal = 66 points). Secondary clinical outcome measures were gross manual dexterity (Box and Block Test [BBT]; number of blocks that can be moved in 60 seconds (Mathiowetz, Volland, Kashman, & Weber, 1985)), functional performance of the affected upper limb (Wolf Motor Function Test [WMFT]; normal = 5 (Wolf et al., 2005)), grip strength (average of 3 trials in kg with the JAMAR® dynamometer), resistance to passive stretching at the shoulder extensors, elbow flexors, wrist flexors and fingers flexors of the affected upper limb (modified Ashworth scale (Bohannon & Smith, 1987)), as well as the subjects’ self-reported amount and quality of use (i.e. “amount” and “how well” scales) of their affected upper limb in daily activities (Motor Activity Log [MAL]; normal = 5 (Uswatte, Taub, Morris, Light, & Thompson, 2006)).
Interventions
All interventions were realized in the research laboratory by an independent trained therapist in a one-to-one ratio with the participant.
PRT program
The PRT program comprised of resistance exercises of targeted upper limb muscles that play an important role in functional performance after a stroke, i.e. shoulder and elbow flexors, wrist extensors and grip muscles (Boissy, Bourbonnais, Carlotti, Gravel, & Arsenault, 1999). The training program lasted 4 weeks (3 times/week, 60 minutes/session) and followed the recommendations of the American Stroke Association (ASA) position stand on exercise prescription after a stroke (Billinger et al., 2014). Using free weights, the maximal load that an individual could lift once (1RM) was estimated by the 10RM (Brzycki, 1993) in order to limit the risk of tendino-muscular injuries and fatigue. To ensure optimal training intensity, training started at 50% of 1RM and increased by 10% each week to reach 80% of 1RM by week 4. Each training session began and ended by a 5-minute warm-up and relaxation period comprising active movements of the trained muscle groups.
tDCS procedures
Saline-soaked 5X7cm electrodes were used in a bilateral tDCS (Soterix Medical, USA) montage (Marquez et al., 2015a), with the active anode electrode placed over ipsilesional M1 and the cathode electrode placed symmetrically to the anode electrode, over the contralesional M1. Determination of the M1 site was realized with TMS, based on the protocol from Da Silva et al. (DaSilva, Volz, Bikson, & Fregni, 2011). After having cleaned the participant’s skin with alcohol, disposable pre-gelled EMG electrodes were positioned over the affected first dorsal interosseous (FDI) in a belly-tendon montage, and a ground electrode was positioned over the styloid process of the ulna. A swim cap was tightly fitted to the participant’s scalp with reference to the nasion, interaural lines, and inion. A 10X10 grid with sites spaced 1 cm apart was drawn on the cap to guide coil positioning during the determination of M1 location. A 70 mm figure-of-eight coil, connected to the TMS stimulator (Magstim 2002, Magstim Company, Dyfed, UK) was used to determine the hotspot, that is the optimal site eliciting the largest motor evoked potentials (MEP) at the lowest stimulus intensity in the resting FDI of the affected hand (Rossini et al., 2015). The hotspot location on the ipsilesional M1 and the symmetrical position over the contralesional M1 were identified on the swim cap with a marker. For the real-tDCS group, the tDCS was applied for the first 20 minutes of each of the 12 PRT sessions at an intensity of 2 mA (with progressive ramp up/down). For the sham-tDCS group, the tDCS was applied for the first 30 seconds only, to ensure an appropriate blinding of subjects (Gandiga, Hummel, & Cohen, 2006).
Safety and tolerability outcome measures
Safety and tolerability of tDCS applied over several weeks were evaluated by documenting participants’ discomfort, occurrence, and intensity of tDCS-related symptoms, as well as dropout rates. After each training session, participants were questioned about the presence of symptoms during the training, the intensity and their perception about the relation between their symptoms and tDCS with the use of a home-developed structured questionnaire, listing the following possible answers: headache; neck pain; skull pain; tingling; itching; skin burning; skin redness; drowsiness; difficulty to concentrate; mood changes; other symptoms (please describe); none. For each symptom, the participant had to rate its intensity (absent; mild; moderate; severe; not applicable) and its perceived relatedness to tDCS (not related; distantly related; possibly related; probably related; definitively related; not applicable). Moreover, the number and reason for each dropout were documented.
Statistical analysis
Because of the relatively small sample size and the use of ordinal scales for most of our outcome measures of efficacy, safety and tolerability, non-parametric analyses were performed (Ghasemi & Zahediasl, 2012). Demographic and stroke lesion characteristics, as well as baseline clinical outcomes were compared between real- and sham-tDCS groups with a Mann-Whitney U Test.
For the efficacy analysis, intra-group change was assessed by a Wilcoxon signed-rank test. Afterwards, for inter-group comparison, data was first expressed in amount of change (i.e. Post-training value minus Baseline value) and then, the amount of change between real-tDCS and sham-tDCS groups was compared using a Mann-Whitney U test.
For the safety and tolerability analysis, the dropout rates, total number of tDCS-related symptoms and their median intensity and median “perceived relatedness to tDCS” were summarized and compared between groups with a Mann-Whitney U test.
Finally, an a priori analysis was performed to obtain the estimated sample size to inform future tDCS clinical trials. Using an α level = 0.05 and β= 0.20, calculations were based on the differential amount of change, between the real- and sham-tDCS groups, on the FMA scale, our primary outcome measure of clinical efficacy (i.e. means and standard deviation values of pre- and post-FMA measures). All analyses were performed using SPSS (Version 24) and G*Power 3.1 software with significance level set at P < 0.05.
Results
From the 147 individuals screened for eligibility, 14 participants (mean age 68.9±10.0 years; time since stroke 70.9±57.6 months) met the selection criteria and were allocated to real-tDCS (n = 7) or sham-tDCS (n = 7, see CONSORT flow diagram in Fig. 1) groups.
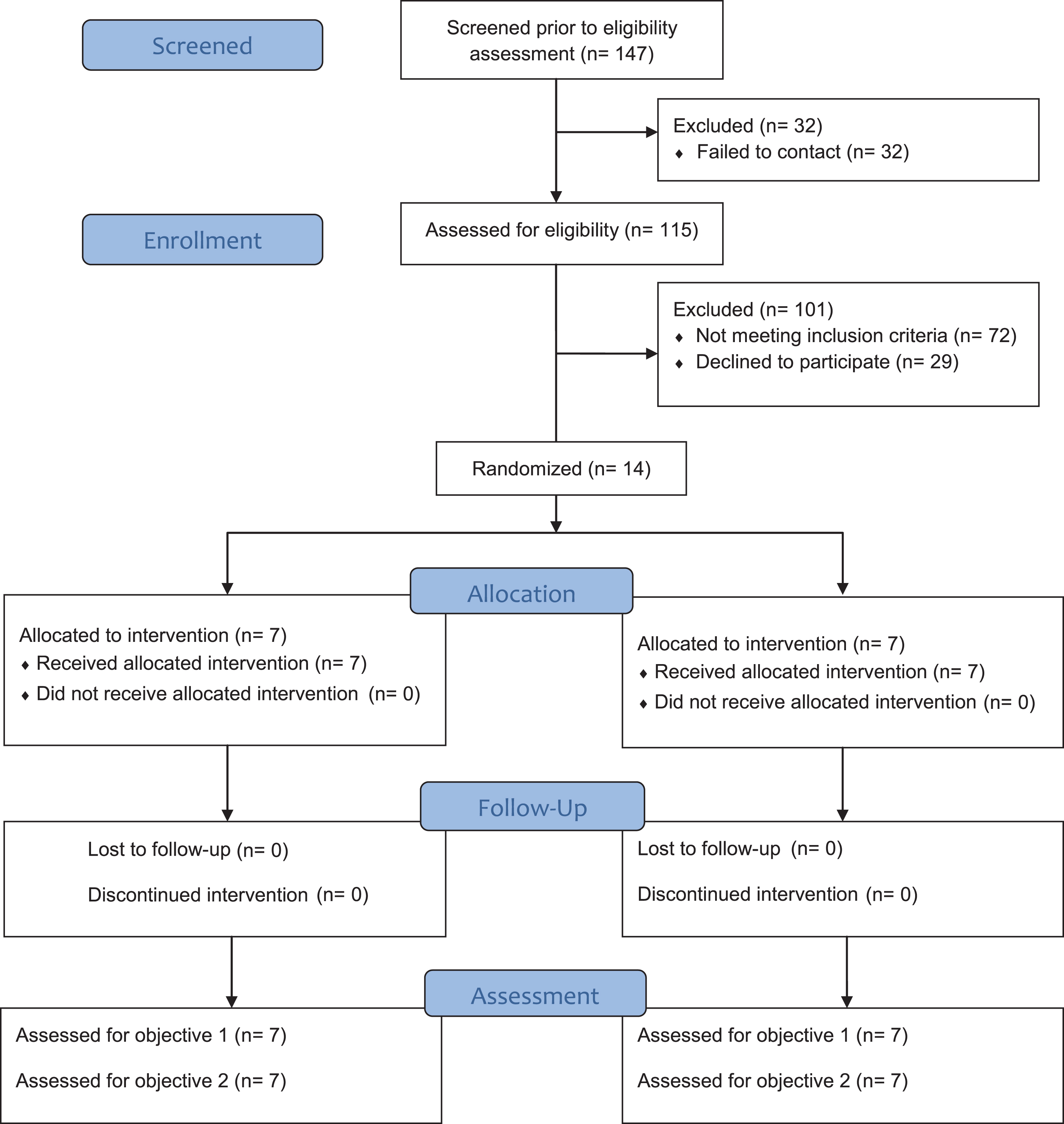
CONSORT diagram of participant flow.
Baseline characteristics between groups
No significant difference was noted across groups for sociodemographic and stroke lesion characteristics (Table 1), and for baseline clinical outcome measures (Table 2). The random allocation based on FMA stratum resulted in: (i) 35–45/66 stratum = no participant for both real and sham tDCS groups; (ii) 46–55/66 stratum = two participants allocated in real-tDCS and one in sham-tDCS groups; (iii) ≥56/66 stratum = five participants allocated in real-tDCS and six in sham-tDCS groups. TMS of the lesioned M1 resulted in detectable MEP in all participants, hence ensuring an appropriate positioning of the tDCS anode.
Demographic and stroke lesion characteristics of participants
Demographic and stroke lesion characteristics of participants
tDCS = transcranial direct current stimulation n = number; SD = standard deviation.
Baseline clinical outcome measures
SD = standard deviation; FMA = Fugl-Meyer Assessment; WMFT = Wolf Motor Function Test; BBT = Box & Block Test; MAL = Motor Activity Log; mAS = modified Ashworth scale; IQR = interquartile range (75th-25th).
Table 3 presents mean changes±standard deviation (SD) and effect sizes for all clinical outcome measures, and p values obtained for statistical comparisons of change between groups. The real-tDCS group significantly improved on the FMA (Fig. 2A, p = 0.018), the WMFT score (Fig. 2B, p = 0.027), the MAL “how well” (Fig. 3A, p = 0.046) and grip strength (Fig. 3B, p = 0.028). Sham-tDCS group significantly improved on the WMFT weight to box (Fig. 2C, p = 0.027), the MAL “how well” (Fig. 3A, p = 0.043) and the BBT (Fig. 3C, p = 0.016). However, no difference was observed between groups for these changes (p > 0.17, cf. Table 3).
Change in clinical outcome measures
Change in clinical outcome measures
SD = standard deviation; FMA = Fugl-Meyer Assessment; WMFT = Wolf Motor Function Test; BBT = Box & Block Test; MAL = Motor Activity Log; mAS = modified Ashworth scale; IQR = interquartile range (75th-25th).

Mean ± standard deviation of clinical outcome measures at baseline (BL) and post-training (PT) coupled with real or sham transcranial direct current stimulation (tDCS). FMA = Fugl-Meyer Assessment; PRT = progressive resistance training; WMFT = Wolf Motor Function Test; *=significant statistical difference (p < 0.05) compared to BL results.
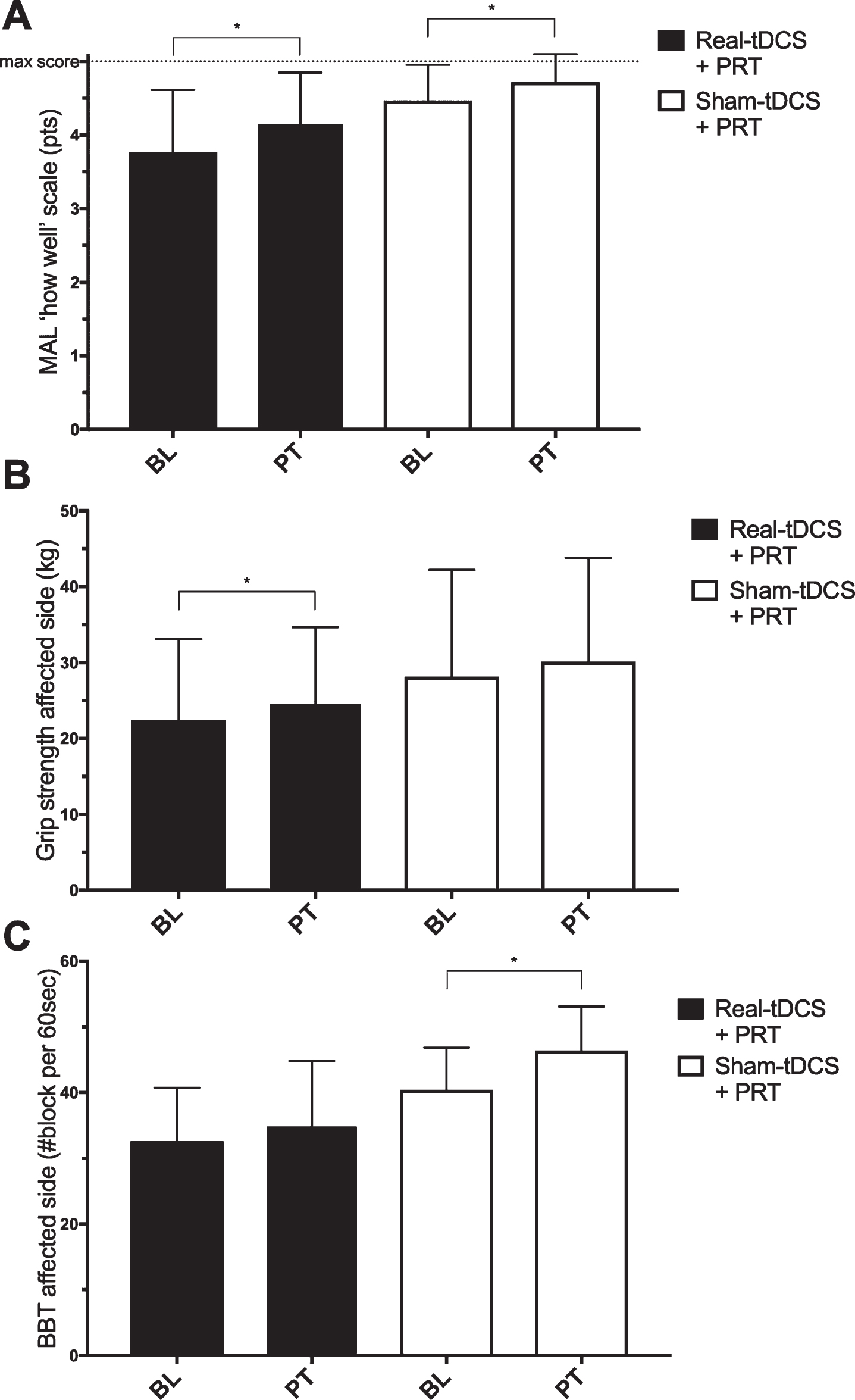
Mean±standard deviation of clinical outcome measures at baseline (BL) and post (PT) training coupled with real or sham transcranial direct current stimulation (tDCS). PRT = progressive resistance training; MAL = Motor Activity Log; BBT = Box & Block test; *=significant statistical difference (p < 0.05) compared to BL results.
Participants attended all assessments and training sessions and no dropout occurred throughout the study. Also, for both groups, the most reported tDCS-related symptom was skin tingling. Precisely, the total number of sessions per participant where skin tingling was perceived ranged between 7/12 and 12/12 sessions (median = 10 sessions for the real-tDCS group and 12 for the sham-tDCS group). The tingling intensity was always rated ‘mild’ and was noted by the participants as ‘possibly’ to ‘probably’ related to tDCS (median = ‘possibly’). No statistical difference between real- and sham-tDCS groups was found for the skin tingling frequency and intensity (p values >0.38). Only one participant in the real-tDCS group reported the perception of mild skin burning during the 4th and the 8th sessions, which was ‘possibly’ related to tDCS according to the subject. No other symptom was reported.
Sample size estimation for future clinical trials
The a priori analysis to estimate the sample size that would be needed in future trials using similar methods resulted in a total of 56 participants, that is 28 participants in each group.
Discussion
In this pilot randomized controlled study, we investigated if a PRT coupled with real-tDCS versus sham-tDCS could lead to greater clinical improvements in terms of sensorimotor recovery of the affected upper limb in individuals at the chronic stage of recovery after a stroke. We also explored the tolerability and safety of repeated sessions of tDCS with resistance training and estimated the minimal sample size that would be required in a future trial to demonstrate, with adequate statistical power, that real-tDCS + PRT is clinically superior to sham-tDCS + PRT. Results showed that tDCS (bi-hemispheric montage) applied over several weeks of PRT was safe and tolerable for the participants. However, results did not support our primary hypothesis, as the real-tDCS group failed to show greater clinical improvements than the control group. Furthermore, we found that a sample of nearly 60 participants would be needed to demonstrate the efficacy of tDCS with PRT on our primary outcome measure of upper limb sensorimotor recovery. Altogether, the present results raise questions that will need to be answered in the future before considering tDCS as an effective adjunct therapy to clinical treatment post-stroke.
The main novelty of the present study is that tDCS was combined with PRT in individuals with a stroke; a therapy extensively used by clinicians and being part of stroke best practice recommendations (Hebert et al., 2016). Previous studies rather combined tDCS with various motor training protocols such as constraint-induced movement therapy (Bolognini et al., 2011), motor skill learning (Lefebvre et al., 2012), robotic training (Hesse, Schmidt, Werner, & Bardeleben, 2003), virtual reality training (Lee & Chun, 2014) and conventional physical/occupational rehabilitation (e.g. task-oriented training, stretching and strengthening (Khedr et al., 2013; Kim et al., 2010)). Because of the great heterogeneity in training protocols combined to tDCS, the potential benefits of tDCS are highly variable across studies and so far inconclusive (Di Pino et al., 2014; Elsner et al., 2017; Kang, Summers, & Cauraugh, 2016; Marquez et al., 2015a; Tedesco Triccas et al., 2016). By using PRT, our intent was to minimize one potential source of variability originating from the use of unstandardized motor training interventions (Klomjai et al., 2015). While PRT resulted in positive sensorimotor improvements in our recruited sample of individuals at the chronic stage post-stroke, we have found no convincing evidence supporting the plus-value of bi-hemispheric tDCS combined to a resistance training. To the best of our knowledge, the efficacy of combining tDCS with PRT has been evaluated only in healthy individuals, using an anodal tDCS montage, with mitigate results (Hendy & Kidgell, 2013; Hendy, Teo, & Kidgell, 2015; Maeda et al., 2017). A recent study failed to demonstrate greater improvement in voluntary knee muscle strength for the anodal tDCS group as compared to the sham-tDCS one (Maeda et al., 2017). Another study showed that the combination of a 3-week resistance training program of wrist extensors with anodal tDCS induced a greater increase of corticospinal excitability and decrease of M1 intracortical inhibitory mechanism, as assessed with TMS, compared to sham-tDCS (Hendy & Kidgell, 2013). However, the authors could not link these neurophysiological effects to functional measures of sensorimotor function, because both sham- and real-tDCS groups showed a similar improvement in wrist extensors strength. These results are in line with our findings with the stroke population and suggest that the expected neurophysiological effects of tDCS on networks involved in motor control do not interact in a meaningful way with resistance training. Studies combining tDCS with different approaches of motor practice and physical training like the present one generally share a common rationale: tDCS influences the lesioned and unlesioned motor cortices via similar mechanisms than those observed during motor learning, i.e. long-term potentiation/depression of synaptic activity (Jackson et al., 2016; Simonetta-Moreau, 2014). The ability of tDCS to modulate cortical excitability is deemed to open a therapeutic window during which the lesioned M1 is in a better state to undergo plastic changes in response to training (Di Pino et al., 2014; Kang et al., 2016). However, the lacking efficacy of tDCS coupled with training interventions, as found in the present study and others, might suggest that our understanding of fundamental mechanisms related to non-invasive neuromodulation is still incomplete. As an example, the appropriateness of the interhemispheric model of maladaptive plasticity has been recently challenged in light of the equivocal evidence from tDCS literature in stroke (Di Pino et al., 2014; Tazoe, Endoh, Kitamura, & Ogata, 2014). A recent longitudinal study with stroke participants found no causal evidence linking interhemispheric inhibition mechanisms and motor impairments across the different stages of recovery post-stroke (Xu et al., 2019). The authors concluded that it is not necessarily that non-invasive neurostimulation techniques are not promising tools for neurorehabilitation treatments, but instead that the underlying rationale and mechanisms should be investigated further. In this line, new models of recovery and plasticity are now proposed in an attempt to reconciliate the variable neurophysiological and clinical effects obtained across studies when combining tDCS with rehabilitation interventions. For instance, the “vicariation model” rather considers that the unlesioned hemisphere plays a key compensatory role post-stroke, and that trying to inhibit its excitability could be detrimental to sensorimotor control of the affected limbs (Di Pino et al., 2014). Di Pino and colleagues proposed another model called the “bimodal balance–recovery” (Di Pino et al., 2014). The idea behind is to estimate the structural reserve of the lesioned hemisphere with neuroimaging techniques to determine, for each person, which of the two models (interhemispheric competition vs. vicariation) best applies (Di Pino et al., 2014). Further studies are needed to test the validity of this new model, but it could help to improve tDCS efficacy by tailoring non-invasive brain stimulation protocols to each stroke survivor’s structural cortical reserve.
Moreover, recent publications argue that the choice of tDCS stimulation parameters, such as dosage or electrode placement, are not based on sufficient evidence (Chhatbar et al., 2016; McCambridge, Stinear, & Byblow, 2018; Tedesco Triccas et al., 2016). Future studies are needed to help determine the best parameters to apply with the stroke population, and eventually to better individualized tDCS procedures. Furthermore, the potential influence of brain lesion on electrical current spreading in the cortex can be an important confounding factor that is often not considered in neuromodulation studies, although it could drastically impact tDCS efficacy across individuals (Minjoli et al., 2017). The efficacy of tDCS coupled with training interventions could also depend on the trained muscle groups (upper vs. lower limb), the tDCS protocol (anodal vs. bi-hemispheric), and the time of measurements (immediately after vs. after a retention period) (Di Pino et al., 2014; Kang et al., 2016). Further research is required to better understand how the neurophysiological mechanisms underlying tDCS after-effects interact with those resulting from motor practice, along with the potential influence of tDCS protocol and stroke lesion characteristics on response to transcranial stimulation.
From a clinical perspective, our study confirmed that PRT represents an effective intervention in people at the chronic stage of recovery after a stroke. Resistance training holds a central place in rehabilitation treatments, stroke best practice guidelines and both primary and secondary prevention of stroke (Brogardh & Lexell, 2012; Hebert et al., 2016). Beyond its positive impact on musculoskeletal function and sensorimotor impairments (Brogardh & Lexell, 2012; Morris et al., 2004), resistance training can also have an impact on functional abilities and social participation (Brogardh & Lexell, 2012; Elsner et al., 2017; Morris et al., 2004). More importantly, PRT is a highly standardized intervention with explicit guidelines ensuring optimal training characteristics to all participants (e.g. intensity level, frequency), tailored to their baseline strength. We are thus confident that the absence of additional benefits resulting from the use of tDCS in the present study does not result from a variable training regimen across participants, which has been raised as one of the main confounding factors that can explain the actual equivocal findings on the efficacy of tDCS in a stroke population (Tedesco Triccas et al., 2016). Another important finding of this study is that the combination of tDCS with an intensive PRT program of the affected upper limb was safe and tolerable. This gives additional proof supporting the feasibility of tDCS after a stroke (Aparicio et al., 2016; Russo, Souza Carneiro, Bolognini, & Fregni, 2017). Indeed, recent meta-analysis in stroke and other populations concluded that tDCS typically evokes only mild and transient adverse effects, such as itching, burning sensation, headache or tingling (Aparicio et al., 2016; Russo et al., 2017). Unfortunately, only a small percentage of available publications on tDCS do report information regarding the side effects and dropout rates, along with their reasons. Future studies are encouraged to carefully collect detailed information about tDCS side effects and dropouts, to explicitly document the safety of tDCS. This will become especially important considering the current trend of increasing stimulation intensities, based on evidence of a dose-response relationship between tDCS efficacy and sensorimotor recovery after a stroke (Chhatbar et al., 2016). In light of the efficacy of PRT and the safety/feasibility of tDCS combined to PRT, we recommend that future work should replicate our pilot study protocol using a larger sample size (i.e. at least 28 participants per group based on our sample size estimation). However, a better tailoring of tDCS procedures based on neurophysiological profile of each stroke survivor should be considered, as it could help maximizing tDCS effects on brain plasticity post-stroke.
Limitations
Some limitations of this pilot study require caution when interpreting the results. The small sample size may have increased the risk of both Type I & II errors (Portney & Watkins, 2009). As recently highlighted (Grefkes & Fink, 2016), the field of neuromodulation in stroke rehabilitation is probably ready to move to larger randomized trials. Yet, pilot trials such as this one are of crucial importance when exploring new therapeutic avenues, since they can help shape future larger multicenter trials. Our sample size estimation to thoroughly assess the impact of repetitive tDCS combined to a PRT on sensorimotor recovery of the affected upper limb (n = 28 per subgroup) seems doable for future clinical trials wanting to pursue the evaluation of neuromodulation after a stroke to allow individuals to recover to their full potential. This is possibly due to the fact that the effect size for FMA change was slightly (although not significant) larger with real-tDCS (1.26) compared to sham-tDCS (0.85) group. Another limitation of our study is related to the comparability of the real and sham groups at baseline. Although real- and sham-tDCS groups did not statistically differ in terms of sociodemographic & stroke-related characteristics and baseline clinical outcomes, the real-tDCS group included a higher ratio of haemorrhagic vs. ischemic strokes than the sham-tDCS group. Haemorrhagic and ischemic strokes can show different profiles of functional recovery (Schepers et al., 2008), hence potentially affecting the comparability between real- and sham-tDCS groups. Furthermore, since participants had mostly well recovered from their stroke based on their relatively high baseline FMA scores, a possible ceiling effect of the clinical tools used to assess the affected upper limb could have prevented us from detecting the superiority of real-tDCS over sham-tDCS.
Conclusion
The present study intended to test the clinical efficacy, safety, and tolerability of an intervention combining tDCS with a PRT program over 12 sessions. The intervention was proven feasible with limited adverse events and no dropout. However, tDCS did not result in superior efficacy than sham tDCS, as both groups showed similar sensorimotor improvements of the affected upper limb post-training. While this pilot study supports the positive effects of a standardized resistance training program in individuals at the chronic phase post-stroke, further research in the field of neurostimulation post stroke is needed (Elsner, Kugler, & Mehrholz, 2018), for instance to improve our understanding of the neurophysiological mechanisms underlying non-invasive brain stimulation applications in stroke.
Footnotes
Acknowledgments
This study was supported by a grant from the Quebec Rehabilitation Research Network (REPAR). The research was conducted at the Laboratoire d’évaluation cérébrale et de la douleur at the Research Center on Aging, in Sherbrooke, Quebec, Canada. The authors offer their heartfelt thanks to the research staff (Marie-Claude Girard, Marilyn Tousignant and Marie-Philippe Harvey). The authors also thank Antoine Guillerand and Mathieu Hamel for their technical support. Louis-David Beaulieu held a scholarship from the Research Center on Aging, as well as the Fonds de la recherche du Québec-Santé. Marie-Helene Milot and Catherine Mercier respectively hold a junior 1 and emeritus research scholar of the Fonds de la recherche du Québec-Santé