
Abstract
Background:
A recently updated Cochrane review for mirror therapy (MT) showed a high level of evidence in the treatment of hemiparesis after stroke. However, the therapeutic protocols used in the individual studies showed significant variability.
Objective:
A secondary meta-analysis was performed to detect which parameters of these protocols may influence the effect of MT for upper limb paresis after stroke.
Methods:
Trials included in the Cochrane review, which published data for motor function / impairment of the upper limb, were subjected to this analysis. Trials or trial arms that used MT as group therapy or combined it with electrical or magnetic stimulation were excluded. The analysis focused on the parameters mirror size, uni- or bilateral movement execution, and type of exercise. Data were pooled by calculating the total weighted standardized mean difference and the 95% confidence interval.
Results:
Overall, 32 trials were included. The use of a large mirror compared to a small mirror showed a higher effect on motor function. Movements executed unilaterally showed a higher effect on motor function than a bilateral execution. MT exercises including manipulation of objects showed a minor effect on motor function compared to movements excluding the manipulation of objects. None of the subgroup differences reached statistical significance.
Conclusions:
The results of this analysis suggest that the effects on both motor function and impairment of the affected upper limb depend on the therapy protocol. They furthermore indicate that a large mirror, unilateral movement execution and exercises without objects may be parameters that enhance the effects of MT for improving motor function after stroke.
Introduction
Over the last 20 years, MT for treating hemiparesis after stroke has become increasingly popular (Ramachandran & Altschuler, 2009). During mirror therapy (MT), a mirror is placed in the patient’s mid-sagittal plane in such a way that the mirror image of the unaffected limb looks as if it were the affected one (Fig. 1). Several high quality randomized controlled trials in stroke patients have been performed and published, providing good evidence for the beneficial effect of MT - not only on motor function, but also on motor impairment. A recently published systematic review by Thieme and colleagues identified a total number of 62 randomized controlled trials and randomized cross-over trials with 1982 patients (Thieme et al., 2018).

Execution of mirror therapy with realistic perspective caused by a large mirror, while performing body positions unilaterally without the manipulation of objects.
In spite of this bulk of evidence for the effectiveness of MT, however, the precise procedure or therapy protocol is less clear (Bai et al., 2019; Kim et al., 2017; McCabe, 2011). For people suffering from hemiparesis after stroke, there are only few standardized MT protocols, which also differ from each other (Bieniok et al., 2011; Morkisch & Dohle, 2015; Rothgangel & Braun, 2013). The common basis of all therapy studies is the use of a mirror positioned as described above, though there are different sizes of mirrors, different mounts or boxes and sometimes even covers for the unaffected arm (Cacchio et al., 2009a; Hiragami et al., 2012; Michielsen et al., 2011; Mirela et al., 2015). The frequency and duration of the therapy as well as the tasks of the (un-) affected arm that have to be performed during therapy, differ between the researchers’ individual protocols (McCabe, 2011; Selles et al., 2014; Thieme et al., 2018). In particular, there are three major parameters that have to be distinguished in the application of mirror therapy: Size of the used mirror (full size mirror or “mirror box”-like setup), Movement execution (unilateral or bilateral), and Type of exercise (representation of body positions or manipulation of objects, or both in combination).
These parameters occurred in several trials in various combinations (e.g. Lee et al., 2012; Wang et al., 2015). So far, to the best knowledge of the authors, only two studies specifically compared different application variants of MT in patients after stroke (Bai et al., 2019; Selles et al., 2014). Bai and colleagues conducted a randomized controlled trial to compare the effects of MT with and without object manipulation, in patients with mild to moderate upper limb hemiparesis due to subacute stroke. All of these patients performed the movements or tasks bilaterally. The study group that did not manipulate objects, but exclusively represented body positions within the MT (e.g. wrist extension and flexion), showed a better effect on motor impairment measured with the Fugl-Meyer-Assessment (Bai et al., 2019; Fugl-Meyer et al., 1975). In a trial of Selles and colleagues, the effect of different types of movement execution within MT on movement time of a reaching task was investigated. In patients with chronic post-stroke upper limb paresis (Brunnstrom stages III and IV) movement time increases more when movement execution was performed unilaterally rather than bilaterally (Sawner & LaVigne, 1992; Selles et al., 2014). To our knowledge, no trial has investigated the effects of different mirror sizes during MT. Based on the recently published systematic review (Thieme et al., 2018), the aim of this quantitative analysis was to compare different parameters in therapy protocols in order to provide an evidence-based recommendation for the choice of three main points in the application of MT for upper limb hemiparesis after stroke: mirror size, uni- or bilateral movement execution, and type of exercise.
This analysis was a subgroup analysis of the 2018 published update of the Cochrane review “Mirror therapy for improving motor function after stroke” (Thieme et al., 2018). In addition to the original publication, the checklist in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was applied (Moher et al., 2009).
Data sources
All information sources for the search and the search algorithm are detailed in the original publication, whose searching process was completed in August of 2017. In that update, 62 randomized controlled trials and randomized cross-over trials were found and included in the qualitative synthesis and the risk of bias in individual trials judgement. 51 randomized controlled trials and randomized cross-over trials were included in the quantitative synthesis (Thieme et al., 2018).
Study selection
These 51 trials formed the basis for this secondary meta-analysis with a special focus on different parameters for the practical application of MT for paresis of the upper limb.
The inclusion criteria were as follows: Trials that provided data pertaining to motor function and / or motor impairment of the affected upper limb Trials that published information regarding the therapy protocol, at least one of the following attributes: Size of the mirror Unilateral or bilateral movement execution Type of exercise (representation of body positions and / or manipulation of objects)
All trials that combined MT with any type of electrical or magnetic stimulation or executed MT as group intervention or used Virtual / Augmented Reality were excluded. If this type of intervention concerned only one of several trial arms, data of this arm were excluded and the remaining at least two trial arms were analyzed (see the PRISMA flow chart, Fig. 2) (Moher et al., 2009).

PRISMA Flow Chart of the selection process.
The primary outcome was motor function at the end of the intervention phase. Motor impairment was defined as a secondary outcome (Thieme et al., 2018).
Intervention data, characteristics of participants of the qualitative synthesis and outcome data were used from the quantitative synthesis of Thieme and colleagues 2018 which was based on independent assessment of two raters (HT and NM). Additionally, for this review, two raters (NM and KJ) extracted and agreed upon protocol parameters if they were not collected in the Cochrane review process (Thieme et al., 2018).
The three therapy parameters were analyzed as following:
Mirror size
In the first subgroup analysis, the trials were allocated to two groups: use of a large or small mirror. For size classification, the definition by Kim and colleagues were used (Kim et al., 2017). A size of 50×40 cm (to reach eye level) as the minimum for a large mirror was defined. Each smaller height was defined as a small mirror.
Classification was primarily based on the specification of the size of the mirror in the text of the article. In case this information was not available, the image of the set-up was used for classification (if available). In these cases, two authors independently classified the available images. If both pieces of information were missing or unclear, the trial was not considered in this analysis. Studies with special set-ups to cover the unaffected hand were excluded from that analysis.
Uni- or bilateral movement execution
For the second analysis, the trials were allocated to two groups: unilateral or bilateral movement execution as provided in unambiguous terms or as a description in the text. If movements were exclusively executed by the unaffected upper limb, they were classified as a unilateral movement. The classification bilateral movements was used if both the unaffected and the affected upper limbs executed movements during MT.
Trials that used any other form of movement execution, e.g. passive movements of the affected arm by the therapist, were not allocated to either of the two groups.
Type of exercise
For the third analysis, movement instructions regarding excluding or including the manipulation of objects were used as contrast. Representation of body positions (e.g. wrist extension) without using objects were classified as movements excluding the manipulation of objects.
If there was a combination of the representation of body positions with manipulation of objects (e.g. cups), this trial was classified as movements including the manipulation of objects.
Data analysis
The Review Manager (Review Manager (RevMan), 2014) (Version 5.3) was used for analysis of the continuous data with a random effect model for motor function and motor impairment at the end of the intervention phase. The calculated standardized mean difference (SMD) with 95% confidence intervals (CI) of each trial were pooled through calculation of the overall SMD and 95% CI. The three subgroup analyses were performed for each outcome, motor function and motor impairment, separately.
Results
Outcome data of 51 randomized controlled trials or randomized cross-over trials were analyzed in the meta-analysis of Thieme and colleagues (Thieme et al., 2018). Six of these trials focused on lower extremity, and thus were not considered (Arya et al., 2017; In et al., 2016; Kumar, 2013; Marquez et al., 2012; Mohan et al., 2013; Sütbeyaz et al., 2007).
Of the remaining 44 randomized controlled trials and one randomized cross-over trial (Tezuka et al., 2006) that focused on the upper limb, two trials (Moustapha & Rousseaux, 2012; Pandian et al., 2014) provided no data for any of the motor outcomes. Ten trials (Cha & Kim, 2015; Cho & Cha, 2015; Kim et al., 2014; Kim & Lee, 2015; Kojima et al., 2014; Lee et al., 2016; Nagapattinam, 2015; Schick et al., 2017; Yun et al., 2011) were excluded because the therapy protocol contained a combination of MT with any type of electrical or magnetic stimulation. One trial employed a Virtual Reality set up (In et al., 2012). For five trials, one of the trial arms had to be excluded due to the use of any type of electrical or magnetic stimulation in four trials and the use of MT as a group intervention in one trial (Amasyali & Yaliman, 2016; Ji et al., 2014; Lin et al., 2014; Thieme et al., 2013; Wang et al., 2015).
Finally, a total number of 31 randomized controlled trials and one randomized cross-over trial with 1031 participants fulfilled the inclusion criteria and were included in the quantitative analysis, even though information about all three aspects was not available for every trial (Table 1, Fig. 2).
Overview of trials‘ therapy protocols
Overview of trials‘ therapy protocols
1Provided no information on the mirrors’ size; 2Could not be included into this analysis due to different design of the set up or the type of execution.
All three subgroup analyses could only be performed for 20 trials (62.5 %). Data on motor impairment for the trial of Hiragami and colleagues, that could not be included in the Cochrane review of Thieme and colleagues, could be included in this meta-analysis because the contact with the authors was resumed (Hiragami et al., 2012; Thieme et al., 2018). The mean age of the participants (58.4 years) ranged from 46 years (Arya et al., 2015) to 68 years (Acerra, 2007). There were more males (60%) than females, more participants with an ischemic stroke (70%) than a hemorrhagic stroke, and more participants with a left-sided paresis (53%) than a right-sided paresis of the upper limb included in those trials. The sample size ranged from 14 (Hiragami et al., 2012) to 94 (Tyson et al., 2015) participants.
The size of the mirror was the least published information (78 %), but showed the greatest variance in the design, for example: different self-made constructions, or stool-like covers to prevent looking at the unaffected arm (Cacchio et al., 2009a; Hiragami et al., 2012; Michielsen et al., 2011; Mirela et al., 2015).
Tezuka and colleagues provided no data on the mirror size, but cited the trial of Sütbeyaz and colleagues (not included, see results) which published the size of the mirror in the text of the article (Sütbeyaz et al., 2007; Tezuka et al., 2006). Thus, the trial of Tezuka and colleagues was included with these data (Tezuka et al., 2006). Two trials provided no information about the set-up (Bae et al., 2012; Gurbuz et al., 2016). Five trials published insufficient information, therefore a classification was not possible (Alibakhshi et al., 2016; Cacchio et al., 2009b; Colomer et al., 2016; Park et al., 2015; Piravej et al., 2012). Three trials used a cover over the unaffected hand and were excluded from this analysis (Lim et al., 2016; Michielsen et al., 2011; Yavuzer et al., 2008).
Thus, a total of 22 trials could be included in this analysis - 17 trials for the outcome motor function and 21 trials for the outcome motor impairment (Table 1).
Effect on motor function
In this analysis, the experimental groups (EXP) of nine trials (317 participants: 156 EXP, 161 CON (control group)) (Acerra, 2007; Cacchio et al., 2009a; Dohle et al., 2009; Invernizzi et al., 2013; Kim et al., 2016; Lin et al., 2014; Thieme et al., 2013; Wang et al., 2015; Yoon et al., 2014) used a large mirror and the experimental groups of eight trials (241 participants: 134 EXP, 107 CON) (Amasyali & Yaliman, 2016; Hiragami et al., 2012; Ji et al., 2014; Lee et al., 2012; Rodrigues et al., 2016; Samuelkamaleshkumar et al., 2014; Seok et al., 2010; Tyson et al., 2015) used a small mirror. MT performed with a large mirror had a statistically significant effect on motor function (SMD 0.77, 95% CI 0.20 to 1.33; I2 = 82 %) in participants with paresis of the upper limb following stroke. A considerably smaller, but nevertheless statistically significant effect on motor function was found for the use of a small mirror (SMD 0.28, 95% CI 0.02 to 0.54; I2 = 0%) (Fig. 3). The difference between subgroups was statistically non-significant (P = 0.12).
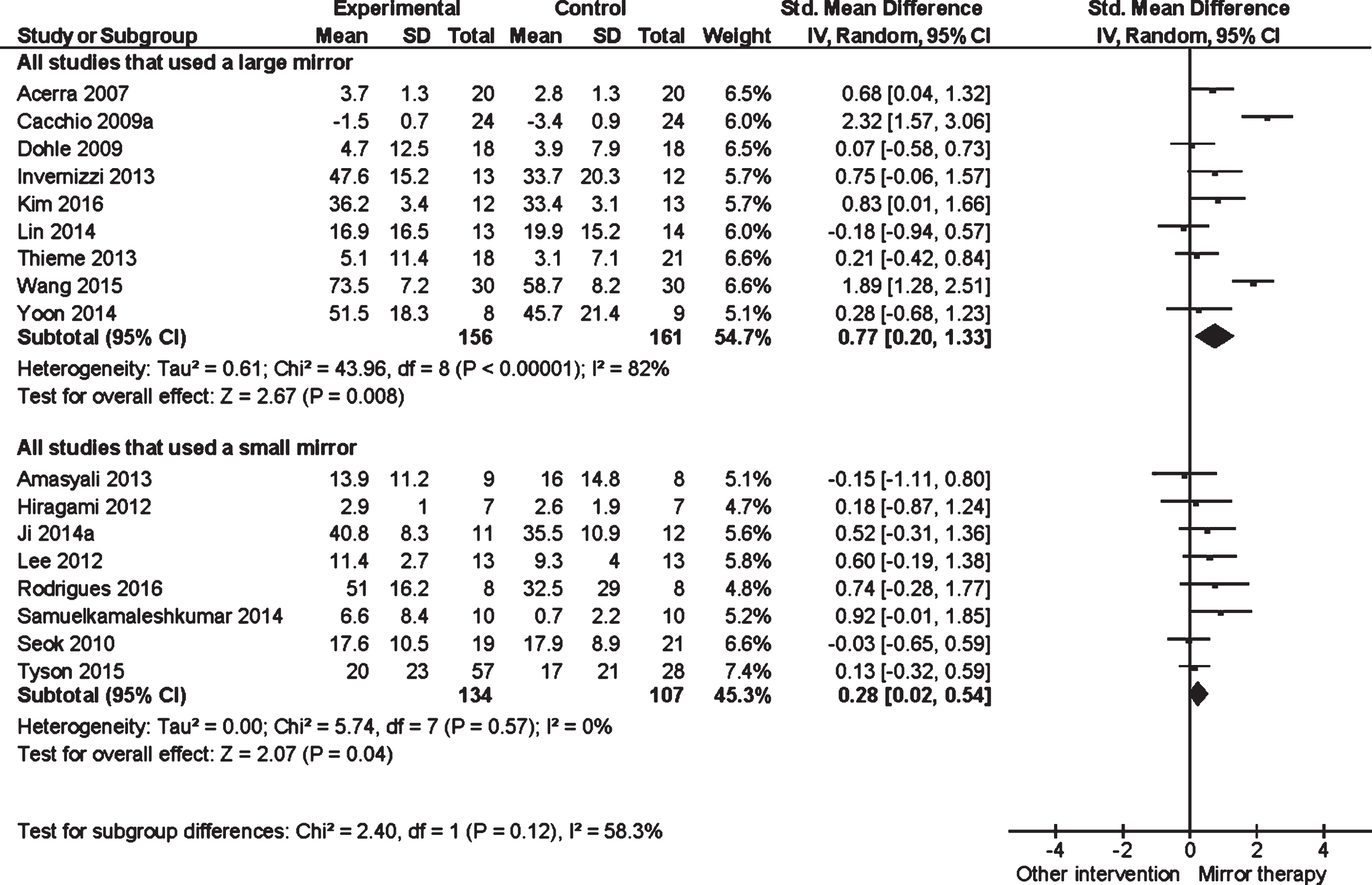
Forest plot of all trials that used a large mirror versus all trials that used a small mirror (Outcome: Motor function).
The experimental groups of 12 trials (372 participants: 185 EXP, 187 CON) (Acerra, 2007; Arya et al., 2015; Dohle et al., 2009; Invernizzi et al., 2013; Kim et al., 2016; Kuzgun et al., 2012; Lin et al., 2014; Tezuka et al., 2006; Thieme et al., 2013; Wang et al., 2015; Wu et al., 2013; Yoon et al., 2014) used a large mirror. The analysis showed a statistically significant effect on motor impairment in participants with upper limb paresis after stroke (SMD 0.62, 95% CI 0.27 to 0.98; I2 = 62%). In the analysis of using a small mirror within the MT, nine trials with a total of 256 participants (141 EXP, 115 CON) (Amasyali & Yaliman, 2016; Hiragami et al., 2012; Ji et al., 2014; Lee et al., 2012; Mirela et al., 2015; Rodrigues et al., 2016; Samuelkamaleshkumar et al., 2014; Seok et al., 2010; Tyson et al., 2015) were included. There was a statistically non-significant effect on motor impairment for this type of device (SMD 0.26, 95% CI –0.06 to 0.57; I2 = 28%). Subgroup differences did not demonstrate statistical significance (P = 0.13).
Effects of uni- or bilateral movement execution
Two trials provided no information on a uni- or bilateral upper limb movement execution (Kuzgun et al., 2012; Piravej et al., 2012). The trial of Tezuka and co-workers was not included, because the therapist passively moved the affected side (Tezuka et al., 2006).
In summary, a total of 29 trials could be included in this subgroup analysis- 23 trials for the outcome of motor function and 25 for the outcome of motor impairment (Table 1).
Effect on motor function
In 12 trials with a total of 360 participants (174 EXP, 186 CON) (Amasyali & Yaliman, 2016; Cacchio et al., 2009a, 2009b; Colomer et al., 2016; Invernizzi et al., 2013; Ji et al., 2014; Kim et al., 2016; Park et al., 2015; Samuelkamaleshkumar et al., 2014; Seok et al., 2010; Wang et al., 2015; Yoon et al., 2014) unilateral movements were executed within MT. The analysis showed a statistically significant effect on motor function (SMD 0.69, 95% CI 0.11 to 1.27; I2 = 84%). In the analysis of trials executing bilateral movements within MT, 11 trials with a total of 367 participants (196 EXP, 171 CON) (Acerra, 2007; Alibakhshi et al., 2016; Bae et al., 2012; Dohle et al., 2009; Hiragami et al., 2012; Lee et al., 2012; Lin et al., 2014; Michielsen et al., 2011; Rodrigues et al., 2016; Thieme et al., 2013; Tyson et al., 2015) were included. A considerably smaller, but nevertheless statistically significant effect on motor function was also found for the bilateral execution of movements within the MT (SMD 0.36, 95% CI 0.14 to 0.59; I2 = 12%) (Fig. 4). The test for subgroup differences did not reach statistical significance (P = 0.31).
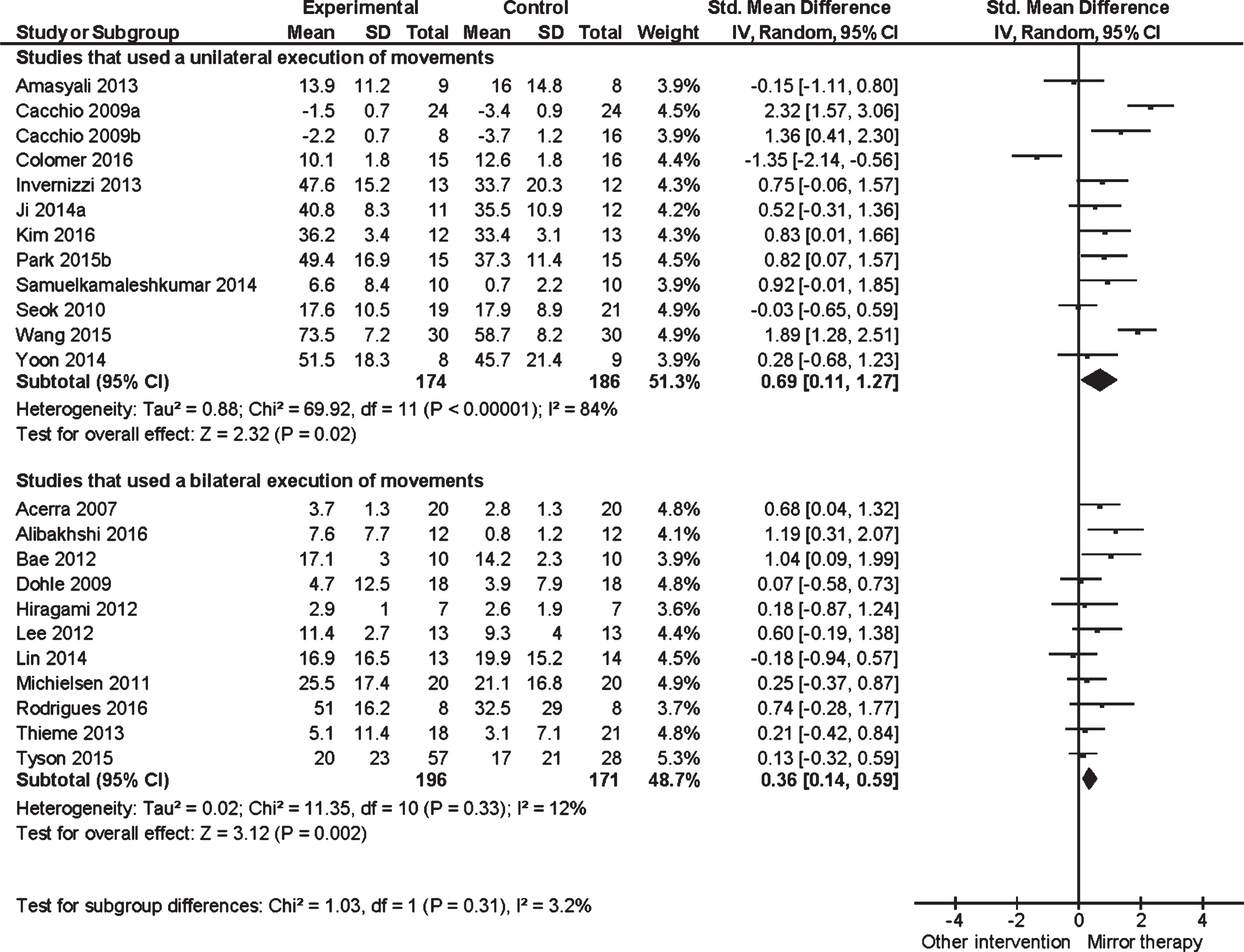
Forest plot of all trials that used unilateral movement execution versus all trials that used bilateral movement execution (Outcome: Motor function).
Data for motor impairment were presented in 11 trials with a total of 322 participants (160 EXP, 162 CON) (Amasyali & Yaliman, 2016; Arya et al., 2015; Colomer et al., 2016; Gurbuz et al., 2016; Invernizzi et al., 2013; Ji et al., 2014; Kim et al., 2016; Samuelkamaleshkumar et al., 2014; Seok et al., 2010; Wang et al., 2015; Yoon et al., 2014) that executed unilateral movements within the MT. This analysis showed a statistically significant effect on motor impairment in participants with paresis of the upper limb after stroke (SMD 0.56, 95% CI 0.10 to 1.03; I2 = 75%). In 14 trials with a total of 493 participants (257 EXP, 236 CON) (Acerra, 2007; Alibakhshi et al., 2016; Dohle et al., 2009; Hiragami et al., 2012; Lee et al., 2012; Lim et al., 2016; Lin et al., 2014; Michielsen et al., 2011; Mirela et al., 2015; Rodrigues et al., 2016; Thieme et al., 2013; Tyson et al., 2015; Wu et al., 2013; Yavuzer et al., 2008) bilateral movements were executed within the MT. The analysis showed also a statistically significant effect (SMD 0.40; 95 % CI 0.15 to 0.64; I2 = 40%). The subgroup differences did not demonstrate statistical significance (P = 0.53).
Effects of type of exercise
Two of trials provided no information on type of exercise, therefore they were excluded from this analysis (Alibakhshi et al., 2016; Kuzgun et al., 2012).
A total of 30 trials presented information about the type of exercise - 23 trials for the outcome motor function and 27 for the outcome motor impairment (Table 1).
Effect on motor function
In ten trials the participants (276 participants: 133 EXP, 143 CON) (Amasyali & Yaliman, 2016; Bae et al., 2012; Cacchio et al., 2009a, 2009b; Dohle et al., 2009; Invernizzi et al., 2013; Ji et al., 2014; Lee et al., 2012; Seok et al., 2010; Yoon et al., 2014) were asked to represent body positions, excluding the manipulation of objects within MT. In thirteen trials with a total of 460 participants (242 EXP, 218 CON) (Acerra, 2007; Colomer et al., 2016; Hiragami et al., 2012; Kim et al., 2016; Lin et al., 2014; Michielsen et al., 2011; Park et al., 2015; Piravej et al., 2012; Rodrigues et al., 2016; Samuelkamaleshkumar et al., 2014; Thieme et al., 2013; Tyson et al., 2015; Wang et al., 2015), the execution of both exercise types was required within MT, representation of body positions and manipulation of objects. The subgroup analysis presented a statistically significant effect on motor function (SMD 0.67, 95% CI 0.18 to 1.16; I2 = 73 %), when the manipulation of objects was excluded within MT. There was a statistically non-significant effect on motor function, when the required movements contained the manipulation of objects (SMD 0.39, 95 % CI –0.03 to 0.80; I2 = 77 %) (Fig. 5). However, subgroup differences did not demonstrate statistical significance (P = 0.39).
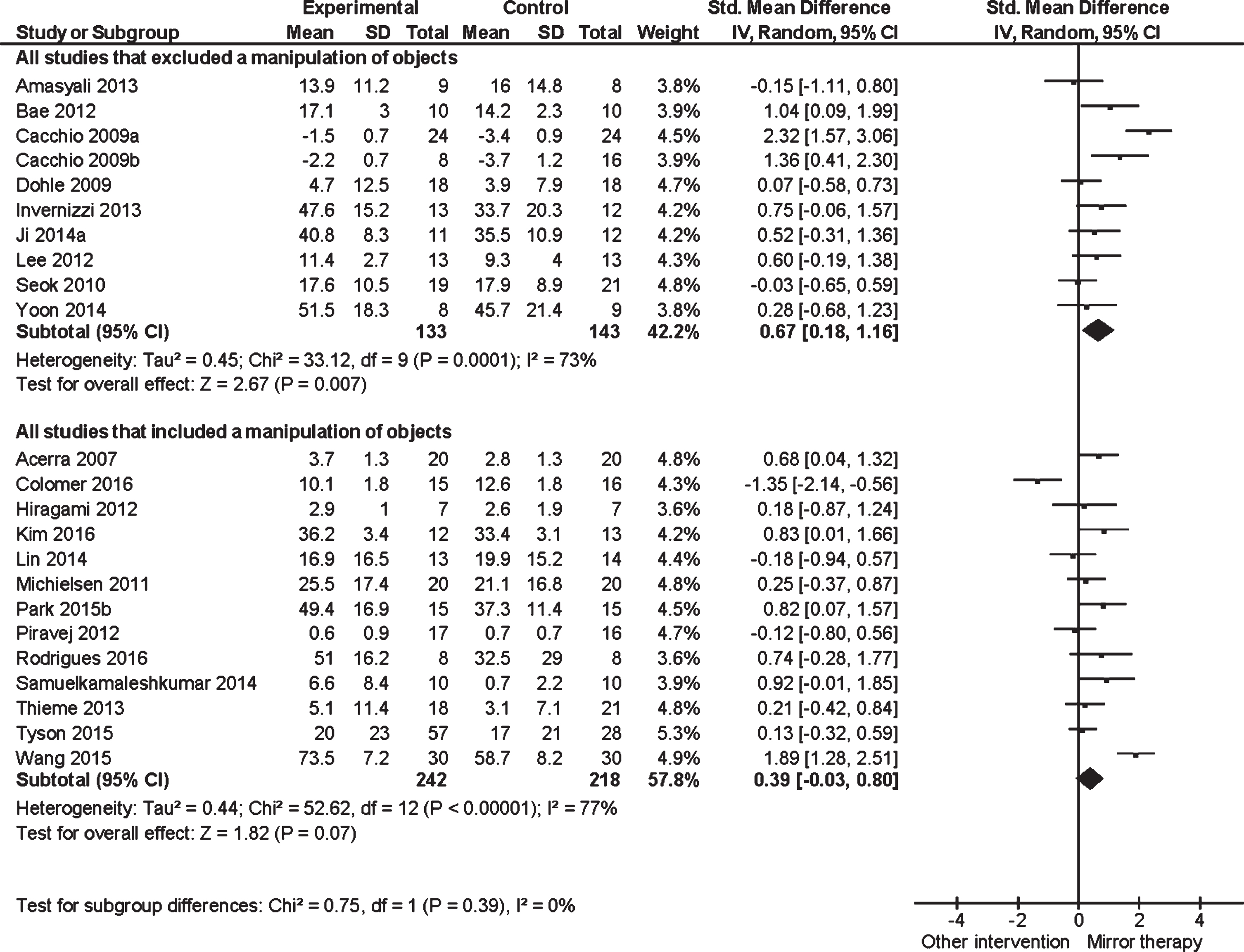
Forest plot of all trials that excluded manipulation of objects versus all trials that included manipulation of objects (Outcome: Motor function).
The experimental groups of 11 trials (286 participants: 141 EXP, 145 CON) (Amasyali & Yaliman, 2016; Dohle et al., 2009; Gurbuz et al., 2016; Invernizzi et al., 2013; Ji et al., 2014; Kuzgun et al., 2012; Lee et al., 2012; Mirela et al., 2015; Seok et al., 2010; Yavuzer et al., 2008; Yoon et al., 2014) excluded object manipulation while performing the movements within MT. The analysis showed a statistically significant effect on motor impairment in participants with upper limb paresis after stroke (SMD 0.42, 95% CI 0.18 to 0.67; I2 = 7 %).
In the analysis of a combination of object manipulation and representation of body positions within the MT, 16 trials with a total of 573 participants (300 EXP, 273 CON) (Acerra, 2007; Arya et al., 2015; Colomer et al., 2016; Hiragami et al., 2012; Kim et al., 2016; Lim et al., 2016; Lin et al., 2014; Michielsen et al., 2011; Piravej et al., 2012; Rodrigues et al., 2016; Samuelkamaleshkumar et al., 2014; Tezuka et al., 2006; Thieme et al., 2013; Tyson et al., 2015; Wang et al., 2015; Wu et al., 2013) were included. There was also a statistically significant effect on motor impairment for this type of exercise (SMD 0.43, 95 % CI 0.10 to 0.75; I2 = 70%). Between subgroups, there was a statistically non-significant difference (P = 0.99).
Discussion
The aim of this meta-analysis was to gain knowledge about the effect of different parameters in MT protocols for upper limb paresis after stroke. The results suggest that both motor function and motor impairment of the affected upper limb depend on the therapy protocol. Despite the lack of significant differences between subgroups, the results indicate that a large mirror, unilateral movement execution and exercises without objects lead to better results regarding motor function and motor impairment.
Effects of mirror size
Regarding the outcome parameters, motor function as well as motor impairment, the effects of a large mirror were greater than the effects of a small mirror within the included trials.
The mirror illusion is produced during the observation of the moving reflected limb in the mirror (Fig. 1). A large mirror enables a realistic perspective to be formed. That means it supports the perception that the mirror image complements the body of the person. Results of studies in the field of Virtual Reality showed the importance of body presentation design and its influence on presence and body ownership (Gonzalez-Franco et al., 2010; Sanchez-Vives & Slater, 2005; Waltemate et al., 2018).
The benefit of having a large mirror might be that it allows a less distracted unilateral visual feedback. That means the observation of the mirror image is less distracted by the moving unaffected arm, whereas a small mirror tends to produce bilateral visual feedback. From a therapeutic point of view, it is important to adapt the physical and cognitive demands of the therapy content to the patients. A large mirror offers another advantage in that case. As proximal parts of the arm could also be included, an adaptation of the content of therapy, called Shaping, is possible (Hömberg, 2013; Morkisch et al., 2017a, 2017b). For example, the standardized therapy protocol developed by Morkisch and Dohle provided up to 125 potential combinations of distal and proximal parts of the arm for adaption of the therapy content. The number of combinations is selected on the basis on the patients’ level of performance. That shaping mechanism could optimize the patients’ visual attention to observe the mirror illusion (Bieniok et al., 2011; Morkisch & Dohle, 2015; Morkisch et al., 2017b). Using a small mirror does not provide this opportunity: In that case, only a very low number of different tasks can be required, which bears the risk of introducing repetitive tasks that do not require constant attention towards the mirror image.
Effects of uni- or bilateral movement execution
In our analysis, a unilateral movement execution showed a greater effect on both motor function and motor impairment than a bilateral movement execution. This is in accordance with a study of Selles and co-workers that directly compared different therapy variants in patients with an upper limb paresis after stroke. In their analysis of improvement of movement time, unilaterally executed MT did not statistically differ from a training of the affected arm only. However, bilaterally executed MT was less effective. The authors assumed greater fatigue of the affected arm in those conditions (Selles et al., 2014).
Furthermore, bilateral execution requires split attention to both body sides and thus may reduce attention to the affected arm (and its image). This consideration is also true for conventional bilateral training (without a mirror), as indicated in three recent systematic reviews (Hatem et al., 2016; Pollock et al., 2014; Veerbeek et al., 2014). However, for MT, there might be a selection effect as well. “True” bilateral performance of MT is only possible for mild paresis when active movements of the affected limb are possible at all. In this context, McCabe and colleagues already showed in 2011 that not exactly identical movements of the arm in front of and behind the mirror can lead to unpleasant sensations and even pain, possibly further degrading the therapy effect (McCabe, 2011).
The advantage of the mirror illusion is to influence the brain’s networks without moving the affected upper limb at the same time. Several imaging studies showed a sufficient neural activation in the observation of unilateral self-performed, mirrored movements without movements of the affected limb at all (Dohle et al., 2004; Mehnert et al., 2013; Wang et al., 2013).
Effects of type of exercise
Regarding motor function, realization of MT without object manipulation showed a greater effect than therapy variants including object manipulation. For the outcome parameter motor impairment, the effects of inclusion or exclusion of object manipulation were similar. This is in line with a recently published randomized controlled trial that compared MT variants with and without use of objects in patients with mild to moderate hemiparesis. The authors reported a tendency for greater improvement in motor impairment for MT without the manipulation of objects (Bai et al., 2019).
This view was recently challenged by an fMRI study of Manuweera and co-workers, reporting greater activation of the superior parietal lobe extending into the intraparietal sulcus and its coupling with the primary motor cortex in mirrored conditions with object (target) compared to conditions without an object (target) (Manuweera et al., 2019). It should be considered, however, that this study only reported brain activation measures during performance of the task, but no behavioral data on the effect of mirror training under these conditions. Up to now, it is unclear whether this increased brain activation does in fact transform into behavioral improvement or just reflects compensatory activity due to an increase in task complexity. In fact, there were other areas in the primary somatosensory cortex and bilateral insula that are more active in the conditions without a target.
Beyond that, the results of this subgroup analysis seem to contradict common assumptions on motor learning. A recently published systematic review on motor rehabilitation to upper limb paresis after stroke recommended the incorporation of task-oriented approaches into the rehabilitation process (Veerbeek et al., 2014). However, Hatem and colleagues argued that the motor enhancements were not translated into the activities of daily living (Hatem et al., 2016). During MT, a task-oriented training via manipulation of objects is basically possible as well. However, this requires a coordinate transformation in addition to the body transformation already introduced by the mirror. Imaging results showed that body and coordinate transformation are accomplished by distinct and different neural structures (Dohle et al., 2011). Additional coordinate transformation does not only reduce activity in the precunei of either hemisphere, but also movement accuracy. Thus, coordinate transformations in a mirror can be performed and trained, but this might reduce neural activity and attention to the mirror illusion itself.
It might be argued that MT without objects might be too low demanding in order to keep sustained attention to the mirror image. However, the level of demand could be increased in other ways as well. For example, the Bonn and Berlin therapy protocols allowed the combination of proximal and distal body postures, thus varying task difficulty (Bieniok et al., 2011; Morkisch & Dohle, 2015). Additional shaping items such as instruction pace could further modify the level of demand (Morkisch et al., 2017a).
Limitations of the study
None of the differences in the three analyses was significant. This might also be due to the fact that the majority of studies was included in more than one of the analyses. Thus, possible differences between the clinical effects could not be unambiguously attributed to only one factor. Nevertheless, the direction of the differences provided strong suggestions on the “optimum” therapy protocol, which is in accordance with neurophysiological mechanisms (as detailed above).
Despite the application of a random effect model, the heterogeneity of the single subgroup analyses was very high, already in the original and other reviews on MT published previously (Cantero-Téllez et al., 2018; Hartman & Altschuler, 2016; Thieme et al., 2018). In the Cochrane review, subgroup analyses regarding the study population, e.g. stage of stroke, could not reduce this heterogeneity (Thieme et al., 2018).
Some of the trials only included stroke patients with sensory deficits or the presence of CRPS (Cacchio et al., 2009a, 2009b; Colomer et al., 2016). Notably, these trials provided especially outlier results (Fig. 3–5).
Implications for further research
In general, as already proposed by Hartman and Altschuler, further analyses regarding the MT effect should try to identify subgroups of patients who may derive benefit from MT (Hartman & Altschuler, 2016). In a pilot study, Brunetti and collaborators suggested to use the change of brain activation due to the mirror illusion as a predictor (Brunetti et al., 2015). Another approach using routine data, identified the sensory deficit, especially 2-point discrimination, as a potential predictor (Seifert et al., 2017). However, based on the present analysis, it cannot be excluded that different patients (e.g. hemiparesis, sensory deficit or pain) respond to different therapy protocols differently. To the best knowledge of the authors, this has not yet been investigated in detail.
Conclusion
The included trials showed a high variance in the actual execution of MT. The results of this meta-analysis indicate that improvement of both motor function and motor impairment of the affected upper limb after stroke depend on the therapy protocol. The use of a large mirror, a unilateral movement execution and exercises excluding the manipulation of objects were shown to result in greater effects. These are aspects of the therapy protocols proposed by the authors previously (Bieniok et al., 2011; Morkisch & Dohle, 2015). However, the results should be interpreted with caution, because the tests for subgroup differences did not reach statistical significance.
Due to the existing bulk of evidence, further studies aiming to demonstrate the efficacy of MT as an adjunct therapy or compared to a placebo therapy are no longer necessary (Thieme et al., 2018). Rather, new studies should consider specific questions regarding the optimal application of MT after stroke. Ultimately, this should result in the definition of an optimum therapy protocol and an optimum target population for applying MT after stroke.
Conflict of interest statement
HT and CD are each author of an included study. Both authors were neither involved in checking these trisals for eligibility, nor did they extract data from these trials.
Both HT and CD have received and will receive honorarium for presentations and seminars on mirror therapy and have received grants from the Federal Ministry of Education and Research for studies on conventional and technical-assisted mirror therapy.
CD and NM are authors of therapy manuals on mirror therapy, published at Schulz-Kirchner-Verlag (CD) and Hippocampus Verlag (CD and NM).
Footnotes
Acknowledgments
This study was not supported by any grant. Assistance provided by Katrin Jettkowski was greatly appreciated.