
Abstract
Background:
Both 1 Hz repetitive transcranial magnetic stimulation (rTMS) and intermittent theta-burst stimulation (iTBS) are reported to benefit upper limb motor function rehabilitation in patients with stroke. However, the efficacy of combining 1 Hz rTMS and iTBS has not been adequately explored.
Objective:
We aimed to compare the effects of 1 Hz rTMS and the combination of 1 Hz rTMS and iTBS on the upper limb motor function in the subacute phase post-stroke.
Methods:
Twenty-eight participants were randomly assigned to three groups: Group A (1 Hz rTMS over the contralesional primary motor cortex (M1) and iTBS over the ipsilesional M1), Group B (contralesional 1 Hz rTMS and ipsilesional sham iTBS), and Group C (contralesional sham 1 Hz rTMS and ipsilesional sham iTBS). The participants received the same conventional rehabilitation accompanied by sessions of transcranial magnetic stimulation for two weeks (5 days one week). Motor-evoked potential (MEP), upper extremity Fugl-Meyer Assessment (UE-FMA), and Barthel Index (BI) were performed before and after the sessions.
Results:
Group A showed greater UE-FMA, BI, and MEP amplitude improvement and more significant decrement in MEP latency compared to Group B and Group C in testable patients. Correlation analyses in Group A revealed a close relation between ipsilesional MEP amplitude increment and UE-FMA gain.
Conclusions:
The combining of 1 Hz rTMS and iTBS protocol in the present study is tolerable and more beneficial for motor improvement than the single use of 1 Hz rTMS in patients with subacute stroke.
Introduction
Stroke is the leading cause of adult disability worldwide, particularly for the domain of the motor system. According to the recent global burden of disease study, there are 10.3 million new strokes each year (Thrift et al., 2017). Up to 75% of stroke survivors are not able to perform activities of daily living with the affected upper limb (Feigin, Norrving, & Mensah, 2017). At present, rehabilitation therapy is the best approach for treating neurological deficits after stroke.3 However, it is not ideal because quite a part of stroke survivors remain neurologically impaired after rehabilitation. Based upon the concept of interhemispheric rivalry, where the intact hemisphere (IH) loses the interhemispheric inhibition from the stroke hemisphere (SH), it has been proposed that either stimulation of SH or inhibition of the IH can increase the motor excitability of SH. It can potentially translate to improved motor functions (Dionisio, Duarte, Patricio, & Castelo-Branco, 2018; Zhang, Xing, Shuai, et al., 2017). Recent studies have shown that the repetitive transcranial magnetic stimulation (rTMS) can modulate cortical excitability and harness neuroplasticity in stroke patients to promote their motor recovery (Dionisio et al., 2018; Graef, Dadalt, Rodrigues, Stein, & Pagnussat, 2016; Zhang, Xing, Shuai, et al., 2017).
Inhibitory rTMS administered in the contralesional motor cortex at a frequency of ≤1 Hz is a strategy that has shown potential to disrupt this possible maladaptive transcallosal pathway (Sebastianelli et al., 2017). Under the mechanism of long-term depression (LTD), 1 Hz rTMS has been found, primarily, to reduce contralesional cortical excitability and, secondarily, to increase ipsilesional activity (Dionisio et al., 2018; Graef et al., 2016; Sebastianelli et al., 2017; Zhang, Xing, Shuai, et al., 2017). A meta-analysis presented that low-frequency rTMS to the unaffected hemisphere induced more functional recovery than high-frequency rTMS to the affected hemisphere (Zhang, Xing, Fan, et al., 2017).
Theta-burst stimulation (TBS) is a varied form of rTMS and has more rapid and robust effects than rTMS (Li et al., 2019). Compared with the classic rTMS, TBS has many advantages such as fewer number of pulses (600–1200 pulse versus 1200 pulse above) and lower stimulus intensity (40–80% rest motor threshold versus 90–130% rest motor threshold), which can avoid the coil overheating and produce longer-lasting cortical excitability (30–60 minutes versus 20–30 minutes) (Diekhoff-Krebs et al., 2017; Long et al., 2018; Sebastianelli et al., 2017). Long-term stimulation of the classic rTMS quickly makes the cerebral cortex resistant and affects the therapeutic effect, while TBS effectively avoids tolerance problems by changing the stimulation pattern (intracluster frequency 50 Hz, inter-cluster frequency 5 Hz). Applying intermittent TBS (iTBS) to ipsilesional M1 significantly increased ipsilesional M1 excitability and motor function and decreased contralesional M1 excitability as compared to control stimulation (Diekhoff-Krebs et al., 2017). But continuous TBS (cTBS) over the intact hemisphere did not change motor behavior of the paretic hands in stroke patients (Talelli et al., 2007).
While iTBS of the SH directly increases the excitability of ipsilateral corticospinal neurons, 1 Hz rTMS of IH produces a more indirect effect by suppressing the transcallosal inhibition (Diekhoff-Krebs et al., 2017; Zhang, Xing, Fan, et al., 2017). Based on the previous study that was combining high-frequency (10 Hz) and low-frequency (1 Hz) rTMS protocol was reported tolerable and more beneficial for motor improvement than the unilateral use of low-frequency (1 Hz) rTMS alone (Long et al., 2018). As the two approaches of 1 Hz rTMS and iTBS have different underlying neurophysiological mechanisms, they could have an additive effect on improving the excitability of the SH when used sequentially during the same setting, and thereby, improve the motor functions. With this hypothesis and the excellent efficacy of previously combined stimulation, the study aimed to find the combined effects of iTBS of SH and 1 Hz rTMS of IH on the motor function and activities of daily living as measured by the upper extremity Fugl-Meyer Assessment (UE-FMA) and Barthel Index (BI). Our study included the electrophysiological examination of motor-evoked potential (MEP) to test the cortical excitability.
Methods
Experimental design and subjects
Study participants were recruited from the patients who were hospitalized at the Rehabilitation Department of the First Hospital of China Medical University. The inclusion criteria included: (1) ischemic or hemorrhagic lesion within 1 hemisphere documented by computed tomography (CT) or magnetic resonance imaging (MRI); (2) 30 to 60 days after the first-ever stroke; (3) aged 30 to 70 years old; (4) an National Institute of Health Stroke Scale (NIHSS) of 1 to 15 points at enrollment (Vanacker et al., 2016). The exclusion criteria were as follows: (1) a large area of cerebral infarct or hemorrhage in the frontal and/or temporal lobe; (2) major circulatory, respiratory disease, neurological disease/deficit other than stroke; (3) severe limb orthopedic conditions; (4) recent use of drugs that alter cortical excitability (e.g. sedation, antidepressants); (5) aphasia, spatial neglect, visual field deficit, or emotional problems; (6) history of seizure attack, dementia, cognitive impairment, or other neurodegenerative diseases; (7) TMS contraindications (e.g., pacemakers or metallic objects in the head). We used a power analysis to determine the necessary sample size, based on the previously reported study on the motor function (FMA-UE) changes induced by rTMS, considering 95% power and a 95% CI, we calculated that seven patients should be included in each group (Guan et al., 2017).
All patients gave their written informed consent before participating in this experiment with the approval of the Ethical Review Committee of the First Affiliated Hospital of China Medical University. For this participant-blinded study, one doctor generated the allocation sequence according to a software-based randomization scheme. Another two doctors of the team enrolled participants and assigned them to one of the three treatment arms according to the randomization scheme.
Each patient received ten daily sessions of stimulation (5 days per week for two weeks), each session consisting of 1-course of either real or sham 1-Hz rTMS over the contralesional M1 followed by one more session of either real or sham iTBS over the ipsilesional M1 (Fig. 2). Group A comprised ten subjects who underwent 1 Hz rTMS protocol followed by iTBS. Group B comprised ten subjects who underwent 1 Hz rTMS, followed by sham iTBS. Group C included eight subjects who underwent sham 1 Hz rTMS, followed by sham iTBS. The TMS protocols used in the current study were under the safety guidelines for rTMS applications (Taylor, Galvez, & Loo, 2018). According to the previous research, it is feasible to prime the contralesional M1 first with the inhibitory stimulus to reduce the excitability of the unaffected M1 and followed by the facilitatory ipsilesional stimulus to increase the cortical excitability on the affected M1 (Long et al., 2018).
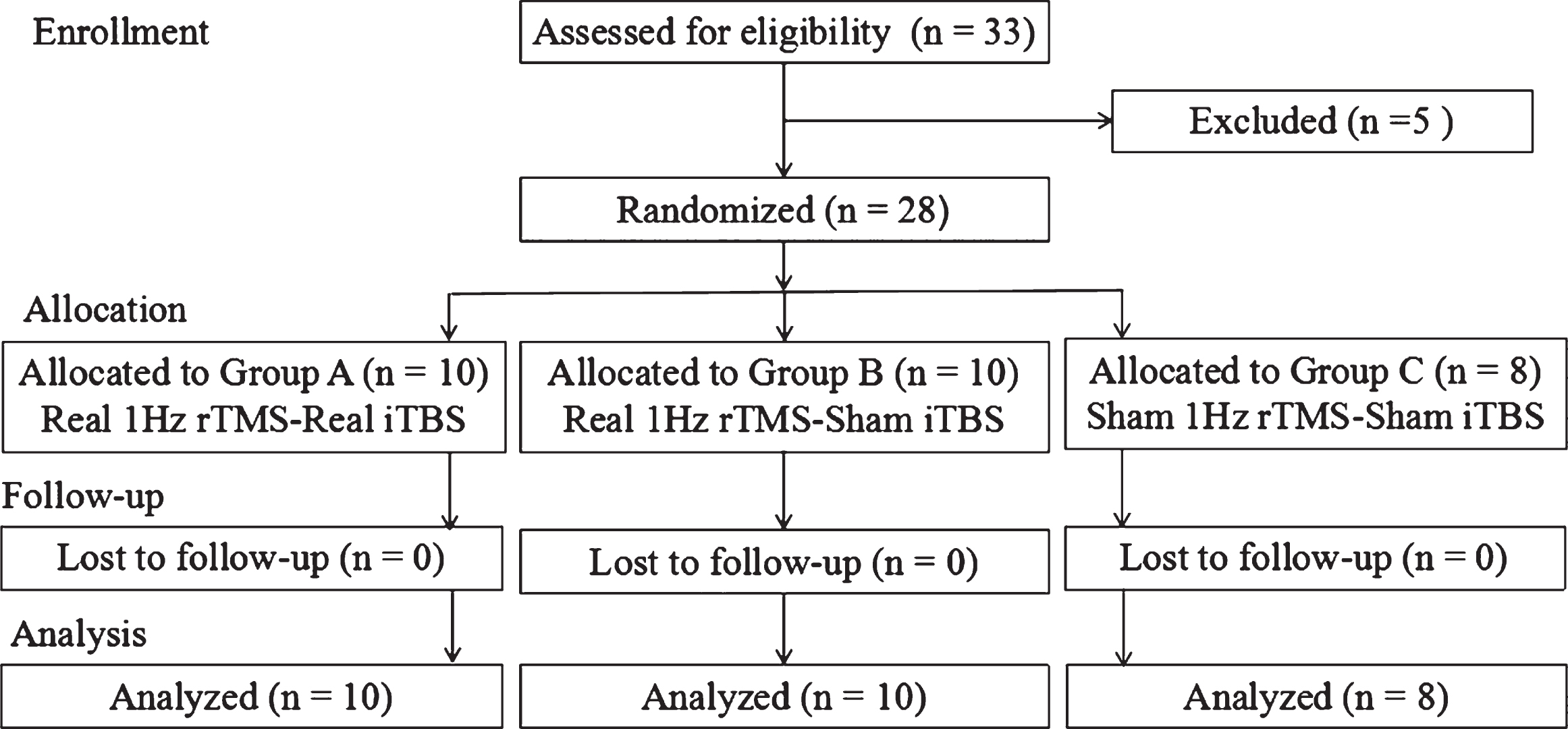
The flowchart illustrates recruitment, group allocation, allocation treatment, follow-up and analysis.
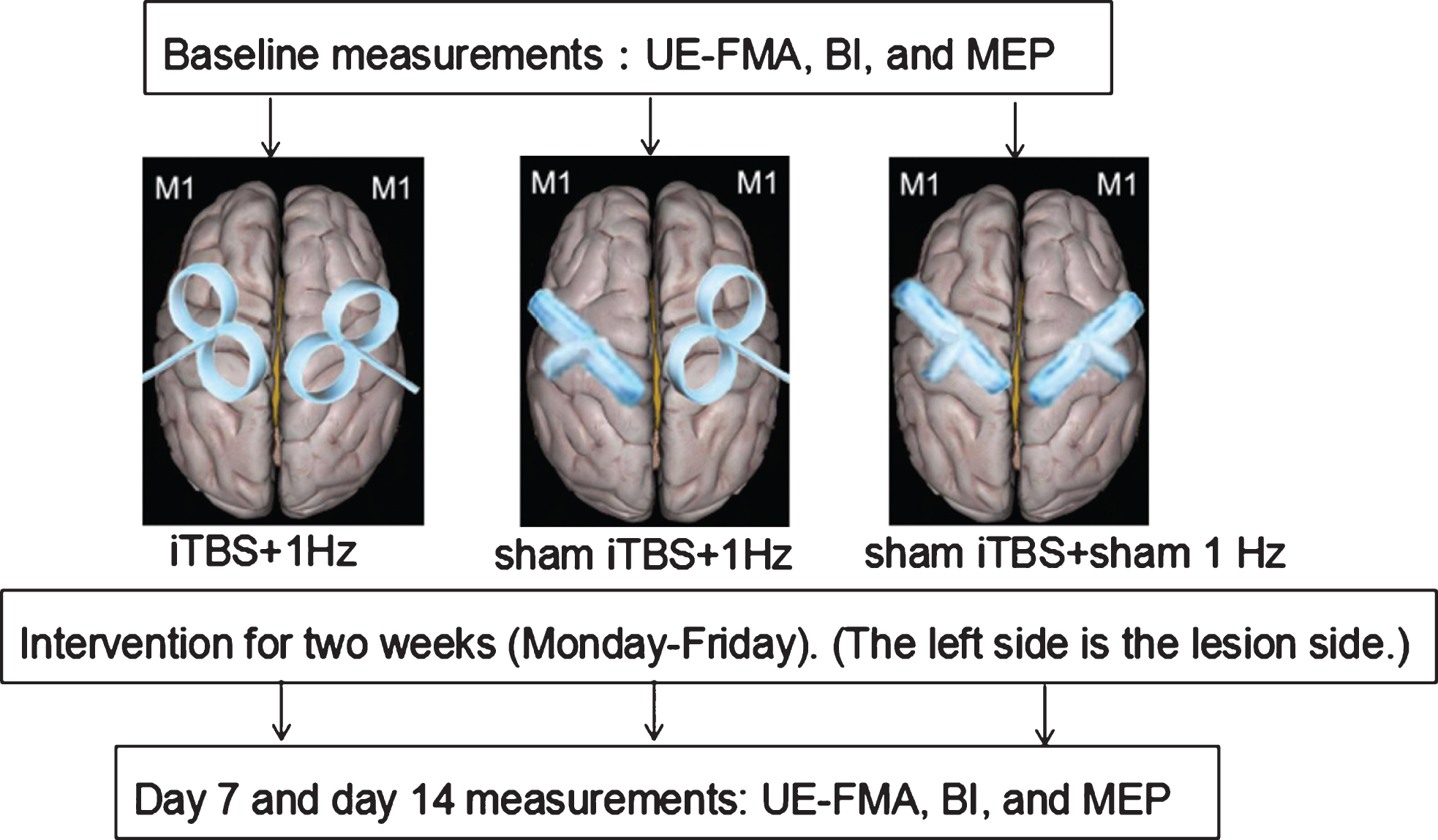
Schematic presentation of the experimental design.
All of the subjects continued the routine of conventional physical rehabilitation and occupational therapy regardless of the group they were assigned. Daily programs included 1 hour of task-oriented training and activities of regular daily exercise, which was conducted by a therapist blinded to group allocation. Before (baseline) and after two weeks of treatment (post), all the subjects participated in motor task evaluations and TMS examinations for corticomotor excitability. This procedure ensured the blindness of patients and examiners.
Electrophysiological measures included corticomotor excitability conducted by TMS (CCY-I rTMS, YIRUIDE, Wuhan, China) through a figure-of-eight coil (diameter: 125 mm), probing resting motor threshold (rMT), maximal amplitude, and latency of motor-evoked potential (MEP) (Du et al., 2018). Electromyography (EMG) instrument (Haishen, Shanghai, China) was connected to the stimulator to record the MEP signals. The amplified (100μV-1 mV/div) and bandpass-filtered (10–500 Hz) signals were digitized at a 20-kHz sampling rate. Motor responses were recorded from the abductor brevis pollicis (thumb abductor) contralateral to the stimulated hemisphere with a pair of Ag-AgCl electrodes. Muscle activity was carefully monitored by real-time EMG to ensure a relaxed state before stimulation. The rMT for MEP was defined as the minimal intensity at which MEPs of at least 50-μV amplitudes could be elicited in half of 10 consecutive stimuli. The MEP amplitude and latency were measured as peak to peak (mV) and the period (ms) between stimulus onset and the start of the largest MEP, respectively (Du et al., 2018). For subjects who showed no MEP response to ipsilesional stimulation, the hot spot and rMT were used by the mirror image of the contralesional hemisphere.
We performed transcranial magnetic stimulation using rTMS with a 125-mm figure-of-eight coil; 1 Hz rTMS trains consisting of 1200 pulses at 100% of rMT were applied over the motor representation of the abductor brevis pollicis in the contralesional M1. iTBS was performed at 60–80% of rMT over the ipsilesional M1, consisting of bursts containing three pulses at 50 Hz repeated at 200-ms intervals for 2 seconds (i.e., at 5 Hz). A 2-second train of iTBS was repeated every 10 seconds for 1200 pulses together (Lin et al., 2019). The initial intensity of iTBS was 60% rMT and increased 5% rMT daily until 80% rMT unless the patient had discomforts like headache or nausea. Once there were uncomfortable symptoms, the intensity would not change until the patient could tolerate. Because many patients had a low motor function and could not complete active motor threshold (AMT) measurement, we chose not to measure AMT and instead used rMT as a reference for stimulation intensity (Pedapati et al., 2015). For sham rTMS, the coil was held at 45°, touching the skull not with the center but with the rim opposite the handle. In this position, the coil–cortex distance is considerably larger such that the electromagnetic field, if at all reaching the cortex, is substantially weaker and far outside the target (Diekhoff-Krebs et al., 2017). Because all the patients had no experience with rTMS, they did not know whether they were receiving real or sham rTMS.
Assessments
All the subjects underwent a blinded evaluation of the upper extremity Fugl-Meyer Assessment (UE-FMA) and Barthel Index (BI) by an independent assessor at two visits before and after rTMS sessions (Kim, 2018; Rezola-Pardo et al., 2019). Electrophysiological measures included corticomotor excitability, probing maximal amplitude, and latency of MEP from paretic abductor brevis pollicis (ABP), extensor digitorum communis (EDC) and biceps brachii (Du et al., 2018). The primary endpoint was defined as the percentage of patients (responders) with a clinically meaningful improvement in the UE-FMA score of 5-point compared with the baseline assessed after a 2-week treatment (Harvey et al., 2018). Secondary measures included the absolute change on the BI, as well as change on the amplitude and latency of MEP after treatment.
Statistics
Statistical analysis was performed using the SPSS software (version 19.0, Inc. Chicago.) The mean values among the groups were compared by either a one-way ANOVA for continuous data or a chi-squared test for categorical data. We compared the absolute change in baseline UE-FMA, BI, and MEP values after treatment using the Student’s t-test. A one-way ANOVA was used to compare the three groups at pre- and post-intervention. In cases in which significant differences were observed, the Bonferroni procedure was used for post hoc pairwise comparisons between the groups. We used the Spearman test to perform correlation analyses of changes to cortex excitability and motor performance. P < 0.05 was considered significant.
Results
Patient characteristics, safety, and tolerance
From June 2018 to March 2019, we screened 33 patients for the study. There were five who either did not meet inclusion or exclusion criteria or declined to participate. The demographic characteristics of the 28 stroke patients are summarized in Table 1. There were no significant differences between the two groups at baseline regarding age, gender, scores of NIHSS, time of intervention after stroke onset, and lesion location. Because not all patients had recordable rMT from the affected APB, we also compared the changes in corticospinal excitability from the affected EDC and biceps brachii.
Demographic Data and Clinical Characteristics of All Patients
Demographic Data and Clinical Characteristics of All Patients
Values are presented as the number of cases or mean±standard deviation. Abbreviations: NIHSS, National Institutes of Health Stroke Scale. All three groups shared the same overall characteristics as listed without a significant difference among groups (P > 0.05).
Following 1 Hz rTMS, iTBS, or sham stimulation, we did not observe seizure induction in our patients. The self-reports of adverse effects following stimulation included light nausea (Group A: 1 case; Group B: 1 case) and mild headache (Group A: 2 cases, Group B:1 case), which disappeared within 5 minutes after stimulation. And they gradually developed tolerance within the fourth treatment. No other adverse effects like a mild tingling sensation, syncope, paresthesia, dizziness, hearing changes, or fatigue appeared, suggesting that iTBS 1200 was well tolerated throughout the intervention period.
The groups were comparable in their baseline motor scales and tasks for the affected upper extremity and activity of daily living (P > 0.05). Three groups had a progressive improvement in the UE-FMA and BI scores over time (Group A: P < 0.01, Group B: P < 0.01, Group C: P < 005, post-intervention compared with baseline, Fig. 3). After two weeks of treatment, there were six responders or 60% in Group A achieving a clinically meaningful improvement on the UE-FMA from baseline, three responders or 30% in Group B, and none responders in Group C. Notably, Group A presented significant post hoc differences (improvements) in the UE-FMA (score increased from baseline to post-intervention: Group A 8.7±6.2 vs. Group B 4±2.2, P = 0.04; Group A 8.7±6.2 vs. Group C 3±1.9, P = 0.004, Fig. 3) and the BI (score change from baseline to post-intervention: Group A 13.5±2.4 vs. Group B 9.5±3.7, P = 0.037; Group A 13.5±2.4 vs. Group C 5±3.8, P < 0.001, Fig. 3). For UE-FMA, Group A presented a much higher improvement of 41.7% in comparison with Group B (17.4% improvement) and Group C (9.4% improvement). For BI, Group A displayed a much more significant increase of 24.1% in comparison with Group B (16.4% improvement) and Group C (9.6% improvement).
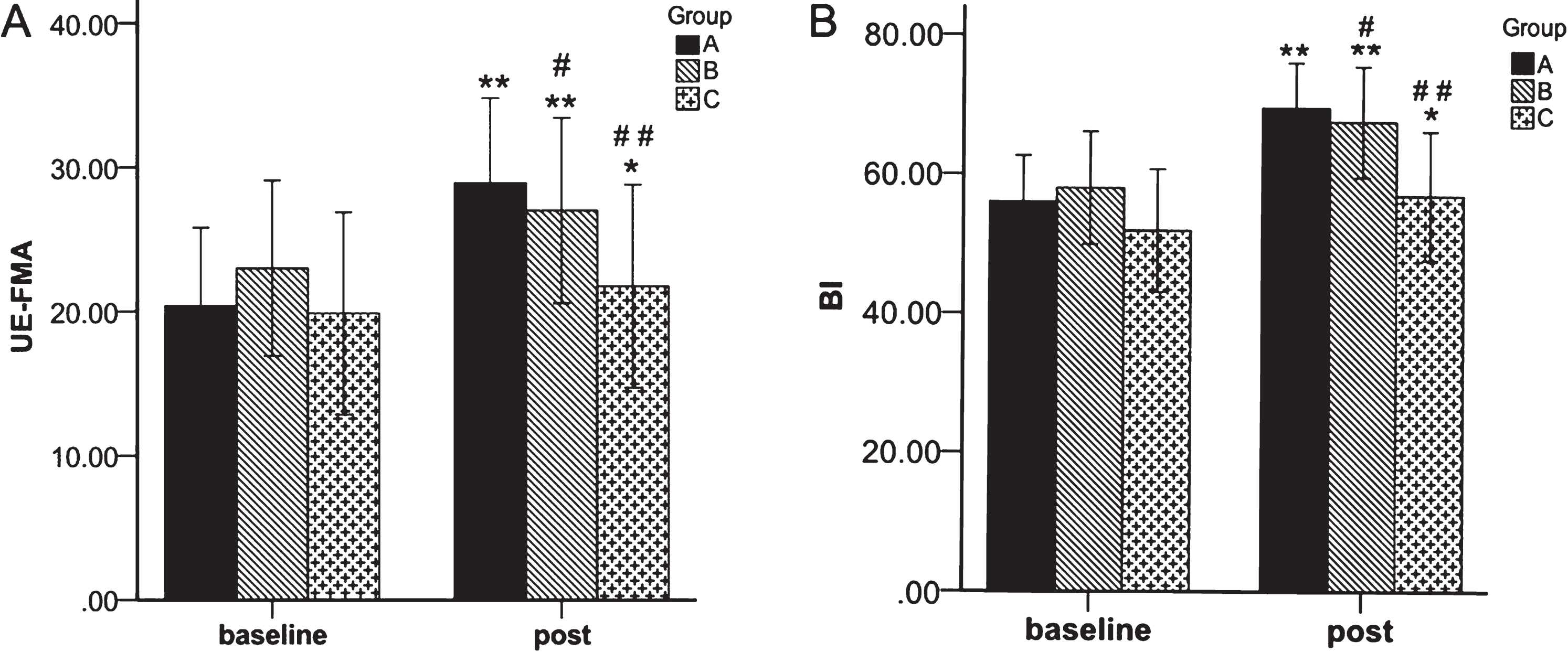
A, B: The mean group values of the UE-FMA and BI before and after the intervention. Values are mean±SD; *p < 0.05, **p < 0.01 versus baseline; and #p < 0.05, # #p < 0.01 versus Group A.
APB MEPs following TMS of the lesioned M1 were absent in eight participants at pre- and post-intervention (three in Group A, three in Group B, and two in Group C). EDC MEPs were absent in eleven participants at pre- and ten post-intervention (four pre- and three post-intervention in Group A, four in Group B, and three in Group C). Biceps brachii MEPs following TMS of the lesioned M1 were absent in four participants at pre- and one post-intervention (two pre- and 0 post-intervention in Group A, one pre- and 0 post-intervention in Group B, and one in Group C). Table 2 summarizes the mean group data for cortical excitability. The groups were comparable in their baseline MEP parameters. We detected that the amplitude increased and the latency shortened in the three groups. Group A showed significant change in MEP amplitude (Group A vs. Group B, P = 0.011 in EDC, P = 0.008 in biceps brachii; Group A vs. Group C, P = 0.001 in APB and EDC, P = 0.008 in biceps brachii) and latency (Group A vs. Group B, P = 0.038 in EDC, P = 0.009 in biceps brachii; Group A vs. Group C, P = 0.001 in APB and biceps brachii, P = 0.004 in EDC) at post in comparison with Group B and Group C. There was a trend of increased corticomotor excitability in the ipsilesional hemisphere. This tendency was particularly apparent in those who showed more considerable UE-FMA improvement (Fig. 4).
Results in motor-evoked potential in the studied groups
Results in motor-evoked potential in the studied groups
All values are presented as mean±standard deviation. MEP, Motor evoked potential. P1, P2: P values determined using the paired t-test and represent changes in data from the baseline to post-treatment. P Avs . B, P Avs . C, P Bvs . C: P values determined using ANCOVA and describe differences in the stimulation effects between the A, B, and C groups and post hoc analyses with Bonferroni correction.
To examine the relation between rTMS-induced cortical excitability changes and functional gain, we performed a correlation analysis for each group. For Group A, the increase of ipsilesional MEP amplitude was positively correlated with the increment of UE-FMA (P = 0.002; r = 0.90; Fig. 4), and the decrement of MEP latency was negatively associated with the increase of UE-FMA (P = 0.003; r = –0.89). However, these associations did not reach significance for Group B (MEP amplitude and UE-FMA: P = 0.79; MEP latency and UE-FMA: P = 0.81, respectively) or Group C (MEP amplitude and UE-FMA: P = 0.28; MEP latency and UE-FMA: P = 0.94 respectively).
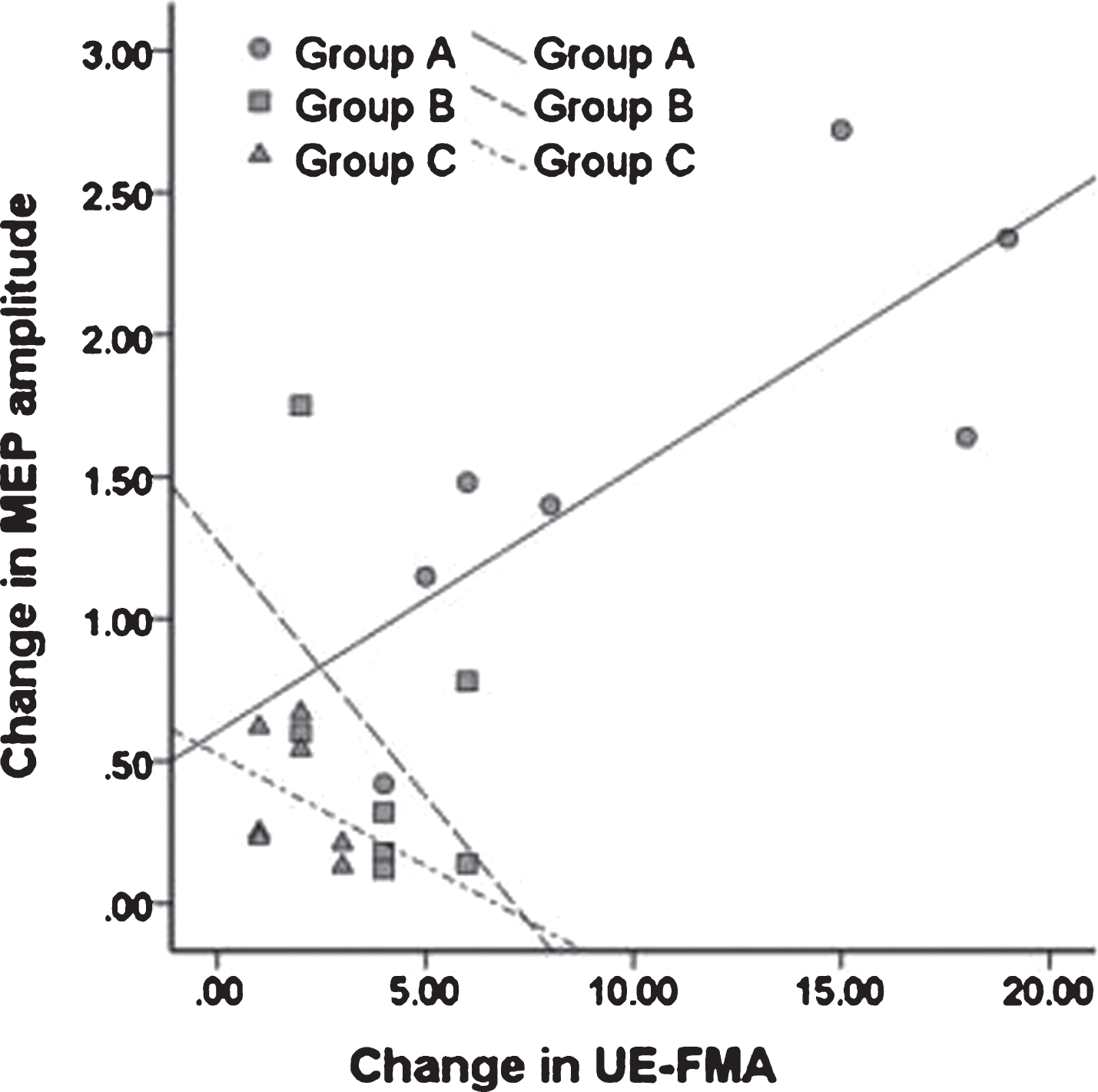
Relationship of change in UE-FMA and change of ipsilesional MEP amplitude among each group after 10-session rTMS. The scatter plot showed the positive correlation between changes in these parameters for group A, and negative relationship for groups B and C, with greater responsibility for group A (P = 0.002; r = 0.90).
The primary result of the present study was that 1 Hz and the combination of 1 Hz rTMS and iTBS improved the motor function of the affected upper limb in post-stroke hemiplegic patients in the subacute phase. Besides, the improvement was more significant in the combination group than in the 1 Hz rTMS group. With the substantial correlation of motor gain and upregulation of ipsilesional cortical excitability, this novel coupling protocol showed bipartite advantages for the amelioration of interhemispheric imbalance and motor restoration in subacute hemiplegic patients.
The theoretical basis of targeting the ipsilesional motor cortex with facilitatory iTBS and the contralesional motor cortex with inhibitory rTMS (1 Hz rTMS) is that the increase in the cortical excitability of stroke hemisphere has been shown to correlate with improvement in motor functions of paretic hand (Birchenall et al., 2018; Rezola-Pardo et al., 2019), and the inhibitory connectivity from the contralesional to the ipsilesional M1 was associated with the degree of motor impairment (Du et al., 2018). Two meta-analyses reported that the existing literature on unilateral rTMS had documented modest improvements from 10% to 30% across a variety of stroke patient assessments, including FMA (Sebastianelli et al., 2017; Zhang, Xing, Fan, et al., 2017). Our study revealed that the UE-FMA performance of Group B benefited from real 1 Hz rTMS conditioning, achieving 17.4% improvement, relative to its baseline level. And the combination approach resulted in an outranged behavior gain of 41.7% for UE-FMA. This result concord with Long and colleagues who found that combined HF- and LF-rTMS protocol (1 Hz rTMS to the contralesional hemisphere followed by 10 Hz rTMS to the lesional hemisphere) for 15 consecutive days resulted in 27% behavioral gain regarding the UE-FMA scores (Long et al., 2018). These findings may prompt the use of multiple courses of coupled rTMS protocol in the treatment of patients with motor dysfunction after stroke.
We observed that the coupling protocol undertaken had a significant additive effect on motor function, as reflected in the FMA and BI results, in comparison with that found in the 1 Hz rTMS group, as shown in Fig. 3. Moreover, the upregulation of ipsilesional cortical excitability as reflected in an increase in MEP amplitude and a decrease in MEP latency were strongly associated with motor performance improvement (as measured in UE-FMA) for Group A, not for Group B or Group C. These findings indicate that derived cortical excitability change in Group A had a more positive impact than in Group B and C regarding clinical consequences. This fact reinforces our contention that, through the priming inhibition of the intact hemisphere and subsequent activation of the perilesional motor network, the combined modulation consolidated the harmonization of abnormal interhemispheric competition, which plays a vital role in the functional recovery of stroke patients. Previous researchers have pointed out that the increase in MEP amplitude and MEP sizes have already been associated with motor recovery (Birchenall et al., 2018; Kuo, Zewdie, Ciechanski, Damji, & Kirton, 2018; Wang, Tsai, Yang, Yang, & Wang, 2014). These earlier observations are comparable to our findings in MEP amplitude with UE-FMA improvement under compound rTMS. This significant behavior-electrophysiological correlation reflects greater neuromodulatory effect of a bihemispheric approach. Besides, researches have shown that iTBS can promote motor re-learning (Butts, Kolar, & Newman-Norlund, 2014; Platz, Adler-Wiebe, Roschka, & Lotze, 2018). It can be inferred that the combined stimulation effect is related to the ameliorating interhemispheric imbalance and the further promotion of motor re-learning.
Several studies have shown that the presence of an MEP was associated with better upper limb functional restoration in acute and chronic stroke (Bembenek, Kurczych, Karli Nski, & Czlonkowska, 2012). Most studies have selected the APB or the first interosseous muscle to record MEP (Li et al., 2016; Zhang, Xing, Shuai, et al., 2017). However, it is difficult for patients with low muscle strength to induce MEP of the distal extensor muscle (Du et al., 2018; Koch et al., 2018). During the rehabilitation process after stroke, the upper limbs usually first appear flexor muscle synergistic movement, then the extensor muscle movement. Therefore, this study measured the MEP of the proximal flexor (biceps brachii) of the affected side, which may detect the subtle changes in the early recovery of function. In patients without MEP of APB before treatment, it still did not appear after the process. For the patients without MEP of EDC before the intervention, the MEP appeared in one after the procedure (Group A). Among the patients without MEP of biceps brachii before the therapy, the MEP appeared in three after treatment (Group A: 2 cases, Group B: 1 case). The innovative measurement of biceps MEP matches more closely the motor recovery from the proximal end to the remote end.
Some patients have mild nausea or headache during treatment, which would relieve after the end of treatment. Generally, they will adapt within four times, and the symptoms will disappear. No other adverse reactions were found in this study. The safety of repetitive sessions of iTBS 1200 over ipsilesional M1 of subacute stroke patients has long been confirmed (Hsu et al., 2013). iTBS of the affected motor cortex during the acute phase in patients with hemiparesis due to capsular infarction also appeared to enhance motor recovery without side effects (Watanabe et al., 2018). This study included in patients with the subacute phase of stroke and excluded those with a large area of cerebral infarct or hemorrhage in the frontal or temporal lobe, and demonstrated the safety of combined low-frequency rTMS and iTBS.
Heterogeneity within our hemiplegic sample may be a confounding factor influencing the study result. Factors such as pathological type, lesion location, time poststroke, and age must all be taken into consideration. Although there was no significant difference for these characteristics across the three study groups, further large-scale investigations with factor stratification are critical for expanding the evidence base. Meanwhile, it is warranted to investigate the long-term effect of this protocol in further study.
Conclusion
In conclusion, our use in this study of a combination of different strategies is a significant step toward securing an optimal motor facilitation process to disabled stroke patients. This randomized, controlled study has contributed critical explicit information to the existing literature that can serve as a sound basis for progressively fine-tuning more effective strategies. Treatment with a compound coupling rTMS protocol opens a promising era of research to underpin widespread clinical practice with greater certainty of achieving motor recovery.
Footnotes
Acknowledgments
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.