
Abstract
Background:
Physical exercise can improve cognitive dysfunction. Its specific mechanism remains unknown. Recent studies have indicated that elevating or peripherally overexpressing brain-derived neurotrophic factors (BDNF) improve cognitive impairment.
Objective:
This meta-analysis aimed to investigate whether physical exercise improves cognitive performance in patients with cognitive dysfunction, such as mild cognitive impairment (MCI) or Alzheimer’s disease (AD), by increasing peripheral BDNF.
Methods:
PubMed, Embase, Cochrane Library, and Web of Science were searched up to June 2020 for studies that assayed the changes in peripheral BDNF levels in MCI and AD patients after exercise training.
Results:
Peripheral BDNF levels were significantly elevated after a single exercise session (SMD = 0.469, 95% CI: 0.150–0.787, P = 0.004) or regular exercise interventions (SMD = 0.418, 95% CI: 0.105–0.731, P = 0.009). Subgroup analysis showed that only regular aerobic exercise interventions (SMD = 0.543, 95% CI: 0.038–1.049, P = 0.035) and intervention duration of 16 weeks or greater (SMD = 0.443, 95% CI: 0.154 –0.733, P = 0.003) significantly increased peripheral BDNF levels. Only plasma BDNF levels (SMD = 0.365, 95% CI:0.066–0.664, P = 0.017) were significantly increased after exercise interventions.
Conclusions:
Acute and chronic physical exercises may improve cognitive impairment by increasing peripheral BDNF levels. Aerobic exercises and a longer duration of exercising increased BDNF levels. These findings also suggest that BDNF may be a suitable biomarker for evaluating the effect of exercise in patients with cognitive impairment, such as AD or MCI.
Keywords
Introduction
Alzheimer’s disease (AD), characterized by progressive cognitive deterioration and memory loss, is the most prevalent form of dementia worldwide, with more than 131.5 million individuals expected to be influenced by 2050. Mild cognitive impairment (MCI) is the preclinical phase of dementia, approximately 13% of which is estimated to evolve into AD every year (Farias et al., 2009). The main pathophysiological changes in AD are aggregation of amyloid-β, formation of neurofibrillary tangles, astrogliosis and microglial cell activation, progressive reduction of cholinergic function, and impaired ability to secrete neurotrophic factors.
Brain-derived neurotrophic factor (BDNF) plays a prominent role in cognition and memory by modulating short- and long-lasting synaptic interactions and controlling neuronal and glial development. It can induce hippocampal long-term potentiation through activation of its high-affinity tyrosine kinase receptor B receptor. This receptor is important for memory formation and consolidation. However, amyloid-β peptide promotes the cleavage of the tyrosine kinase receptor B receptor and attenuates the regulation of synaptic plasticity by BDNF (Jerónimo-Santos et al., 2015). Some post-mortem studies indicated that the transcription and expression of BDNF declined in the cerebral cortex and hippocampus of adults with AD or MCI. Meta-analyses showed a significant decrease in peripheral BDNF levels in patients with AD and a downward tendency in those with MCI (Ng et al., 2019; Qin et al., 2017). In patients with AD, the level of BDNF significantly increased after donepezil or lithium administration. Moreover, ten-year follow-up study indicated that the risk of AD and dementia decreased by more than half in individuals with BDNF levels in the top quintile (Weinstein et al., 2014). These results suggest that high levels of BDNF may prevent the AD and dementia.
Both single episode of exercise and long-term interventions have been shown to elevate BDNF levels in healthy individuals (Dinoff et al., 2016 & 2017). Some studies have demonstrated that physical exercises improved cognitive ability and brain functions (Stillman et al., 2017). Furthermore, the risk of AD and dementia decreased by 45% and 28%, respectively, in a population with a high level of physical exercise (Hamer & Chida, 2009). Meta-analyses have also confirmed that physical exercise interventions promoted cognitive function in older adults, and patients with AD or MCI (Northey et al., 2018; Ströhle et al., 2015). A study has also shown that twelve months of exercise training increased hippocampal volume by 2% and reversed aging-related reduction of hippocampal volume by 1-2 years (Erickson et al., 2011). These effects were associated with an increase in BDNF. Furthermore, animal studies have shown that exercise remarkably upregulates cerebral BDNF expression and increases hippocampal neurogenesis in healthy mice and dementia models (da Costa Daniele et al., 2020; Venezia et al., 2017). These results suggest that physical exercises may improve cognitive impairment by increasing BDNF. In contrast, some studies have shown that cognitive function and BDNF levels in patients with AD or MCI were not ameliorated by exercise interventions (Damirchi et al., 2018; Enette et al., 2020). These conflicting outcomes can be explained in terms of variable discrepancies, such as sex, age, diagnostic criteria, disease severity, and intervention characteristics. Hence, this meta-analysis aimed at investigating whether physical exercise ameliorates cognitive performance in patients with cognitive dysfunction, such as MCI or AD, by increasing peripheral BDNF levels.
Materials and methods
Literature search
This meta-analysis was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses. PubMed, Embase, Cochrane Library, and Web of Science were searched independently by two of the investigators (Hong Huang and Wenyang Li), up to June 2020, for articles that focused on the effect of exercise interventions on peripheral BDNF levels in adults with cognitive dysfunction such as AD or MCI. The searched terms included “Alzheimer’s disease”, “mild cognitive impairment”, “exercise”, “physical exercise,” “exercise therapy”, “physical therapy”, “physical fitness”, “physical activity”, “physical exertion”, and “brain derived neurotrophic factor”. Details of the search strategy are presented in the Supplementary Material section. The search was limited to English publications.
Selection criteria
We included the studies that satisfied the following criteria: (i) subjects with AD or MCI, (ii) BDNF levels were observed before and after exercise, and (iii) single exercise session or regular exercise training. Reviews, meta-analyses, and conference abstracts were excluded. Two reviewers independently screened and included (or excluded) studies, and any differences in opinions were resolved by discussion.
Data collection
Hong Huang and Wenyang Li independently examined the articles for eligibility. Wei Wang was consulted to settle any disagreements. Data on population characteristics, study design, diagnostic criteria, Mini-Mental State Examination (MMSE) score, BDNF level, origin of BDNF, exercise intervention characteristics, and other research details were extracted and organized using a templated word document. We contacted the corresponding authors for missing data as necessary.
Quality assessment
Quality assessment was independently performed by Huang and Li. Inconsistencies were discussed with Wei Wang, who made the final decision. Quality assessment of the randomized controlled trials (RCTs) was performed using the Cochrane risk of bias tool. It included seven items, and each was characterized as “low,” “high,” or “unclear” based on the bias level. Non-randomized studies were evaluated according to the Methodological Index for Non-Randomized Studies (MINORS). It included 12 items, with a maximum score of 24.
Statistical analysis
Effect sizes were presented as standardized mean differences (SMDs) using random-effects models (Borenstein et al., 2010). The suggested formulas were used to calculate the standard deviation by the median and range, or by the standard error and mean, if necessary (Wan et al., 2014). Chi-square test (Chi2) and inconsistency test (I2) were applied to evaluate the statistical heterogeneity between the articles. P < 0.1, or I2 > 50% indicated the presence of significant heterogeneity. The inconsistency explanation followed the prescription in the Cochrane Handbook. Subgroup analyses were conducted based on the type of exercise training, duration of exercise intervention, and origin of BDNF (serum or plasma). Egger’s regression tests and the funnel regression method were used to examine publication bias. Data were analyzed using Stata version 15.0. The figure showing the risk of bias of the RCTs was created using RevMan 5.3.5. Differences were considered statistically significant at P < 0.05.
Results
Study identification and quality assessment
The literature search revealed 702 studies. Among them, 137 were from PubMed, 285 from Embase, 234 from Web of Science, and 46 from Cochrane Library (see Fig. 1). A total of 460 studies were excluded by screening the title and abstract. Another 31 studies were excluded by screening the full text. Two articles (Fungwe et al., 2019; Nascimento et al., 2014;) were excluded because they were from the same study as other reports (Allard et al., 2017; Nascimento et al., 2015). The study by Suzuki et al. was excluded because there was no assay of BDNF levels after exercise (Suzuki et al., 2013). The study focused on the effect of the cybercycle was also excluded (Anderson-Hanley et al., 2012). A final 12 articles were included in the systematic review, and nine articles provided data for the meta-analysis.
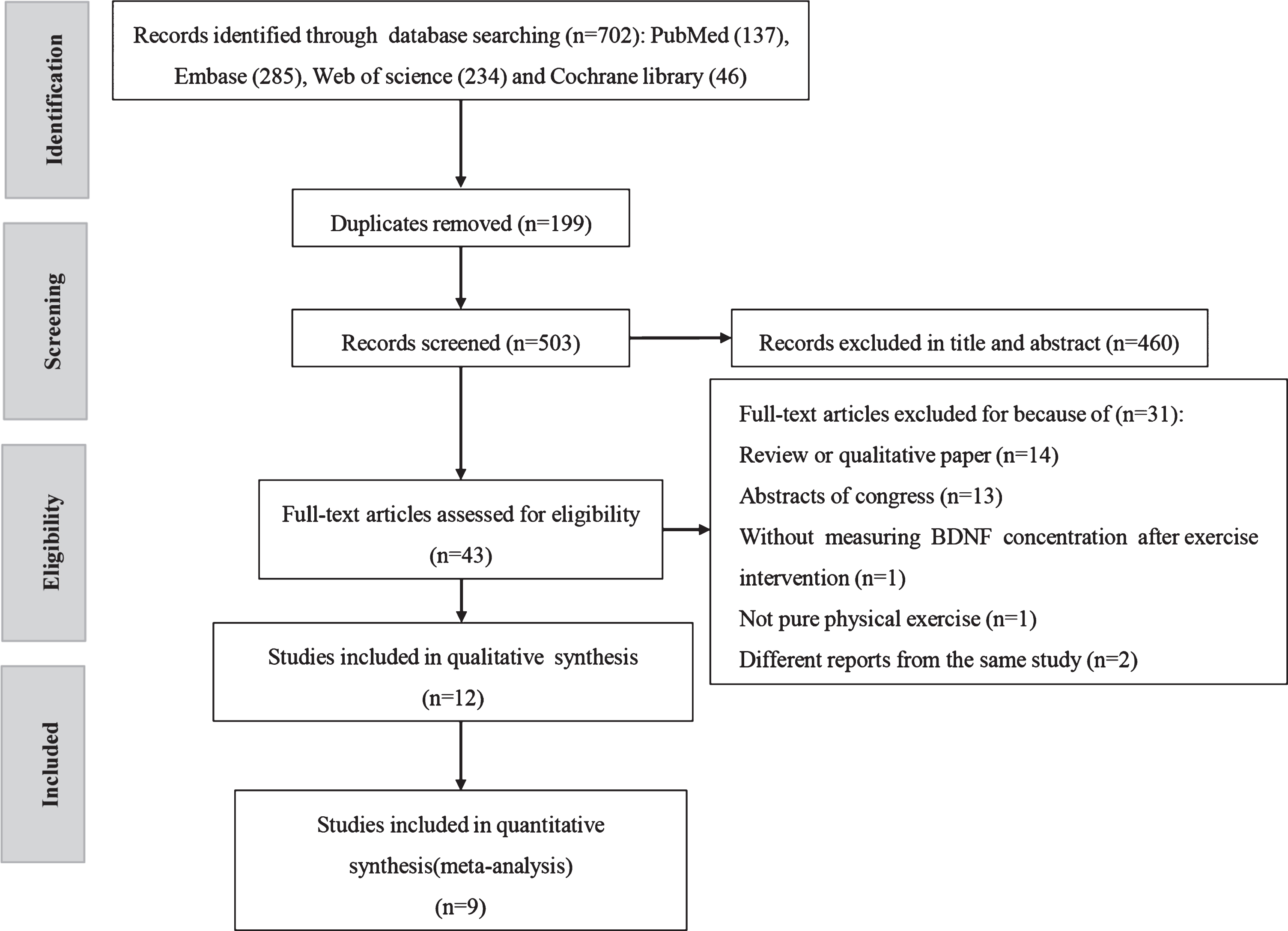
The protocol for searching and selecting studies.
The summary of bias risk of the ten RCTs was performed using the Cochrane Collaboration’s tool as shown in Supplementary Figure S1. All studies were regarded as having a high risk of performance bias because it is unrealistic to expect participants to be blinded to the exercise program. The MINORS scores of the two controlled trials were 14 (Kim et al., 2018) and 15 (Coelho et al., 2014), respectively. Neither of them expounded blinded assessment of the outcomes, and one of them did not calculate the study size prospectively (Coelho et al., 2014).
The characteristics of the included articles are shown in Tables 1–3 according to the type of exercise. Overall, 52 patients with AD (mean age 76.71±4.85, mean BMI 24.84±2.96, mean MMSE 19.30±3.62) and 243 patients with MCI (mean age 67.03±8.24, 63.1% female, mean BMI 25.26±3.99, mean MMSE 26.21±2.16) were included. Four studies (33%) explored changes in BDNF levels after acute exercise (Coelho et al., 2014; Devenney et al., 2019; Kim et al., 2018; Tsai et al., 2018). Another eight studies (67%) examined the changes with regular exercise intervention (Allard et al., 2017; Baker et al., 2010; Damirchi et al., 2018; Enette et al., 2020; Kohanpour et al., 2017; Nascimento et al., 2015; Sungkarat et al., 2018; Tsai et al., 2019). For the regular programmed exercise, exercise intervention characteristics were 42.19±10.86 (30–60) minutes per session, and 3±0.5(2–4) sessions per week for 16.63±6.30 (8–24) weeks. The training intensity of aerobic exercises ranged from 50% to 70% of the maximum oxygen uptake (VO2max), 50% to 85% heart rate reserve (HRR), or 60% –85% of maximal heart rate (HRmax). The training intensity of resistance exercises ranged from 65% to 75% of one repetition maximum (1 RM) or within the desired range (13–15) of ratings of perceived exertion (RPE). No participants in the included studies were taking antidepressant drugs or medications for cognitive impairment during the exercise interventions, except for some those in the study by Enette et al. (Enette et al., 2020).
Overview of aerobic exercise programs
Overview of aerobic exercise programs
AD: Alzheimer’s disease, aMCI: amnestic mild cognitive impairment, BDNF: brain-derived neurotrophic factor, BMI: body mass index, CDR: Clinical Dementia Rating, CT: controlled trials, DSM: Diagnostic and Statistical Manual of Mental Disorders, HRmax: maximal heart rate, HRR: heart rate reserve, McoA: Montreal Cognitive Assessment, MMSE: Mini-Mental State Examination, NR, no reported; RCT: randomized controlled trials.
Overview of resistance exercise programs
aMCI: amnestic mild cognitive impairment, BDNF: brain-derived neurotrophic factor, BMI: body mass index, CDR: Clinical Dementia Rating, MMSE: Mini-Mental State Examination, NR, no reported; RCT: randomized controlled trials, 1 RM: One repetition maximum.
Overview of combined exercise programs
BDNF: brain-derived neurotrophic factor, BMI: body mass index, HRmax: maximal heart rate, HRR: heart rate reserve, KDSQ-C: Korean Dementia Screening Questionnaire Cognition; MCI: mild cognitive impairment, MMSE: Mini-Mental State Examination, MSROM: muscular strength, range of movement, RCT: randomized controlled trials, RPE ratings of perceived exertion.
The pooled results, with a random effect model, indicated that BDNF levels significantly increased after a single exercise session based on the data of three studies (Coelho et al., 2014; Kim et al., 2018; Tsai et al., 2018) (SMD = 0.469, 95% CI: 0.150–0.787, P = 0.004) (see Fig. 2a). Regarding the effect of acute aerobic exercise, all articles reached a consensus that it could significantly increase peripheral BDNF levels (Coelho et al., 2014; Devenney et al., 2019; Tsai et al., 2018). The level of BDNF showed an increasing trend after resistance or combined exercises, but this was not statistically significant (Kim et al., 2018; Tsai et al., 2018).
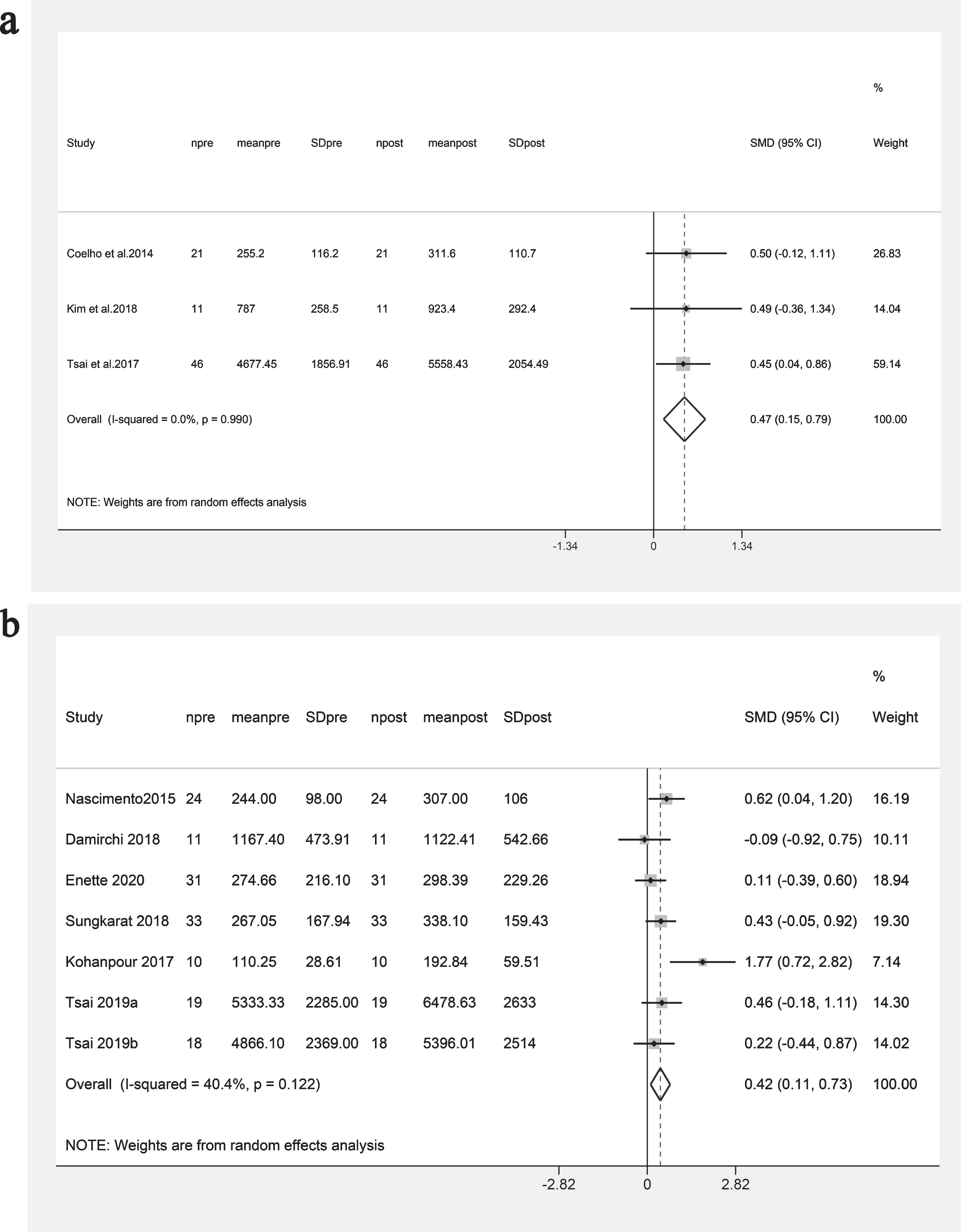
(a). Impact of a single exercise session on peripheral BDNF levels (pg/ml). (b). Impact of regular exercise training on peripheral BDNF levels (pg/ml).
Figure 2b shows that the BDNF levels after regular exercise training were significantly higher than those at baseline (SMD = 0.418, 95% CI: 0.105–0.731, P = 0.009). No significant heterogeneity was detected among the included articles (P = 0.122, I2 = 40.4%). Egger’s test (P = 0.281) and funnel plot (see Fig. 3) did not reveal a significant risk of publication bias. Four of the eight studies indicated a significant increase in BDNF levels (Kohanpour et al., 2017; Nascimento et al., 2015; Sungkarat et al., 2018; Tsai et al., 2019), two studies showed a mild decrease (Baker et al., 2010; Damirchi et al., 2018), while the others reported no significant change (Allard et al., 2017; Enette et al., 2020). Sensitivity analysis showed that none of the included studies had a remarkable impact on the results.

Funnel plot of the studies for regular exercise training.
Subgroup analyses in terms of the type of exercise indicated a significant increase in BDNF levels after aerobic exercise interventions (SMD = 0.543, 95% CI:0.038–1.049, P = 0.035), but not after combined exercise training (SMD = 0.331, 95% CI: –0.347–1.010, P = 0.339) (see Fig. 4). Of note, we did not set up a resistance exercise training group in this analysis because this involved only one study.

Subgroup analysis of the changes in BDNF level based on type of exercise intervention.
Given that the median exercise intervention duration was 16 weeks, we divided these studies into two groups: intervention duration of less than 16 weeks for one group (three studies) and more than 16 weeks for the other group. The comparison showed that the more than 16 weeks group had increased BDNF levels (SMD = 0.443, 95% CI: 0.154 –0.733, P = 0.003) (see Fig. 5).

Subgroup analysis of the changes in BDNF level based on exercise intervention duration.
In terms of the origin of BDNF, Fig. 6 showed a significant increase in plasma BDNF levels (SMD = 0.365, 95% CI: 0.066–0.664, P = 0.017) and only an increasing trend for serum BDNF levels (SMD = 0.514, 95% CI: –0.124–1.153, P = 0.114) after exercise interventions.

Subgroup analysis of the changes in BDNF level based on the origin of the samples.
This meta-analysis indicated that both acute and chronic exercise interventions could elevate the peripheral BDNF level by up to 45% in patients with cognitive dysfunction such as AD or MCI. Longer duration and aerobic exercises led to a higher increase in BDNF levels. These findings suggest that physical exercises may improve cognition and psychiatric symptoms by increasing BDNF levels and may be an effective non-pharmacological treatment strategy for neurodegenerative diseases (Brown et al., 2013). This is the first meta-analysis to focus on the impact of physical exercise on peripheral BDNF levels in patients with cognitive impairment.
The mechanism underlying the increased peripheral BDNF levels is still unknown. It is likely that physical activities not only increase cerebral blood flow, but also enhance synaptic plasticity and hippocampal neurogenesis by inducing BDNF expression. These changes lead to cognitive improvement. Plasma irisin levels of eight healthy subjects significantly increased after ten weeks of endurance training, consisting of 20–35 min cycling per session and 4-5 sessions per week (Boström et al., 2012). Irisin can cross the blood–cerebral barrier to upregulate the level of BDNF and then increase synaptogenesis and synaptic plasticity (Pedersen, 2019). Five weeks of swimming increased the levels of hippocampal FNDC5/irisin and BDNF in one study (Lourenco et al., 2019). Studies using AD models have shown that synaptic plasticity and memory impairment can be improved by peripheral overexpression of FNDC5/irisin. Conversely, it has been shown in AD mice that blocking the FNDC5/irisin/BDNF signaling pathway may attenuate the improvement in memory function from exercise training. On the other hand, seven-day running may also increase the level of BDNF in the hippocampus by activating the DNA demethylation of the BDNF VI promoter (Gomez-Pinilla et al., 2011). Single nucleotide polymorphisms, such as the ɛ4 allele of the apolipoprotein E gene (APOEɛ4) and BDNF val66met, may have an impact on the increase in BDNF resulting from exercise training. It has been reported that BDNF val66met result in decreased activity-dependent secretion of BDNF (Egan et al., 2003) and greater AD-related cognitive impairment (Franzmeier et al., 2021). Nascimento et al. also confirmed that only the subjects with BDNF–Met genotypes presented a significant elevation of BDNF after physical exercises (Nascimento et al., 2015). A pilot study in elderly African Americans showed that non-ApoEɛ4 carriers prominently elevate BDNF levels after six-month aerobic training when compared to ApoEɛ4 carriers (Allard et al., 2017). Future studies are needed to explore the impact of these polymorphisms on increased BDNF levels induced by physical activities in patients with cognitive dysfunction.
Interestingly, aerobic training, rather than resistance exercises, significantly elevated BDNF levels. This outcome was in accordance with the report of Cassilhas et al., who found that aerobic exercises and resistance exercises exerted effects on cognition and neuroplasticity by divergent mechanisms (Cassilhas et al., 2012). Aerobic exercises preferentially upregulated BDNF expression in the hippocampus of rats, while resistance exercises predominantly increased insulin-like growth factor 1. The subgroup analysis showed that exercise interventions of 16 weeks or more may lead to a higher increase in BDNF levels than shorter interventions. Berchtold et al. reported that increased BDNF gradually returned to its baseline level after exercising is stopped, and the reduction rate of BDNF levels depended on the absolute duration of the preceding exercise program (Berchtold et al., 2005). From the origin of the sample, plasma BDNF levels, but not serum BDNF levels, significantly increased after exercise. Similarly, Dinoff et al. also found that the increased BDNF level of plasma was greater than that of serum after physical exercise training (Dinoff et al., 2016 & 2017). The circulating BDNF protein was released from the brain (70% –80%) and absorbed and stored in circulating platelets. It was then released into the serum when the platelets were activated. Hence, the inconsistent change in serum BDNF levels between different studies might be due to the differential release of BDNF from activated platelets during serum extraction.
This study has some limitations. First, the number of enrolled studies was not as high as expected. Only one study was concerned with the impact of resistance exercises. This suggests that the conclusion about resistance exercises should be cautiously explained. Second, the bias risk of the included studies was relatively high. The generation of random sequences was only described in three studies, two of which further clarified allocation concealment. However, inappropriate allocation concealment may exaggerate the therapeutic effects of physical therapy (Armijo-Olivo et al., 2015).
In brief, both acute and chronic physical exercises may improve cognitive impairment by increasing peripheral BDNF levels. Aerobic exercises and a long duration of exercise may increase BDNF levels. These findings also suggest that BDNF level might be a suitable biomarker for evaluating the effect of exercising in patients with cognitive impairment, such as AD or MCI.
Footnotes
Acknowledgments
This study was funded by The National Key Research and Development Program of China (NO. 2016YFC1304502).
Author contributions statement
All the authors conceived and designed the study. H.H. and W. Y. L. collected and analyzed the data. H.H. drafted the manuscript. All authors critically reviewed and revised the manuscript. W.W. supervised the study.
Conflicts of interest
The authors declare no competing interests.