
Abstract
Background:
Continued long-term rehabilitation programs with acquired brain injury are important for their participation in meaningful daily activities.
Objective:
This paper investigated the participation-based interventions on outcomes in patients with acquired brain injury.
Methods:
A systematic review and meta-analysis search for randomized control trials published between 1998 and 2019 using PubMed, CINAHL, and MEDLINE was performed. Nine studies were selected and analyzed for systematic review. Five studies analyzed the effectiveness of participation-based intervention using meta-analysis and assessed the level of evidence of qualitative studies.
Results:
A total of 843 publications were searched. Nine studies met the inclusion criteria and were of high quality. The effective score for improving participation following participation-based interventions in persons with acquired brain injury was 0.32 and significant in this study (p < 0.05).
Conclusions:
The findings of this systematic review and meta-analysis suggest that, in persons with acquired brain injury, participation-based interventions are essential for community living.
Introduction
Acquired brain injury is defined as brain injury that occurs after birth. It is a major health issue and a leading cause of disability worldwide (Jolliffe et al., 2018). Acquired brain injury (ABI) affects both normal development and new learning when young and the brain is still developing. Recovery can take years and may not be complete (Rees and Skidmore, 2008). There are two types of acquired brain injury, traumatic and non-traumatic. Acquired brain injury can cause a variety of impairments depending on the affected brain area and the severity of the damage. It may lead to obvious sensory, motor, cognitive, behavioral, and emotional impairments and long-term functional limitations in daily life and participation limitations in the community (Lannoo et al., 2004; Mahar & Fraser, 2011; Woodson, 2014).
Currently, most studies continue to emphasize measurement and intervention in terms of motor function and mobility. In addition, there is evidence supporting the use of occupation-based interventions to improve daily activity performance (Wolf et al., 2015). However, many people with acquired brain injury continue to live in their community while only having a limited participation in meaningful daily activities (Corrigan et al., 2014; Vogler et al., 2014). Therefore, further research focusing on ach-ieving meaningful participation and quality of life improvement is still needed (Engel-Yeger et al., 2018; Eriksson et al., 2013).
The concept of participation in the International Classification of Functioning, Disability and Health (ICF) has become a meaningful concern for rehabilitation. Participation is defined as engagement in life situations or people’s living experiences in actual situations in their occupations (Cicerone, 2004; World Health Organization, 2001). The conc-ept of ICF participation is described along with the concept of an occupation, which is defined as an individual’s activity or function. An individual’s activity and participation is the result of a dynamic interaction between an individual’s ability and performance, and between environmental and situational factors (World Health Organization, 2001).
Acquired brain injury is a significant cause of long-term disability and research has shown that people with Acquired brain injury perceive that they are re-stricted in all domains of participation. People with acquired brain injury may face a variety of challenges related to engagement from a short and long term perspective. It was considered particularly important to explore the experiences of engaging in everyday life in this population (Häggström and Lund, 2008).
Previous studies have shown that acquired brain injury is one of the most common causes of long-term disability. It is associated with loss of quality of life and substantial economic costs (Grill et al., 2007). When discharged from the inpatient neurological rehabilitation, patients with acquired brain injuries continue to suffer from limited independence, lack of meaningful participation, and poor quality of life. For meaningful participation, the most effective rehabilitation possible is needed to prevent or reduce long-term limitations in participation. Therefore, participation is a key outcome in rehabilitation of persons with acquired brain injuries.
The purpose of this study was to determine the effectiveness of participation-based interventions on outcomes in persons with acquired brain injury by conducting a systematic review and meta-analysis. This study provided evidence to support participa-tion-based interventions for persons with acquired brain injury and to identify target outcomes when applying participation-based interventions. The pri-mary purpose of this study was to determine, via a meta-analysis, participation-based intervention met-hods that are effective in persons with acquired brain injury. The secondary purpose was to assess methods and targeted outcomes of participation-based interventions by conducting a systematic review and to compare the participants, interventions, and outcome measurements used. Through a systematic review, it is aimed at explaining and improving understanding of methods for participation-based intervention which persons with acquired brain injury participate in daily life. Thus, this study provided evidence to support the participation of persons with acquired brain injury.
Methods
Data sources and searches
Studies to assess the methods and effectiveness of participation-based interventions on outcomes in persons with acquired brain injury were searched. Articles published from January 1, 1998 to December 31, 2019 were searched in three databases: PubMed, CINAHL, and MEDLINE. This review was identi-fied articles with the following the search keywords: “acquired brain injury” AND “participation”, “acq-uired brain injury” AND “daily living”, “acquired br-ain injury” AND “activity daily living”, “acquired brain injury” AND “self-care”, and “acquired brain injury” AND “occupation”.
Searching process
This literature search was conducted for original articles that met our inclusion and exclusion criteria. Using the searching keywords, a total of 843 articles were identified. Studies that could not be included solely by inclusion criteria or the content of the abstract were selected through a full-text review. Since we were unable to automatically exclude animal experiments from this search engine, we selected them manually. Abstracts from the rest of the articles have been scrutinized using the inclusion and exclusion criteria.
Thus, a total of 144 articles were included in the full-text review. The final list of systematic review consisted of 9 studies and the list of meta-analysis consisted of 5 studies except for insufficient statistical data (Fig. 1). The following data were extracted from the selected studies: diagnosis of participants, age of participants, study design, methods of assessment, methods of intervention, and operational definition.
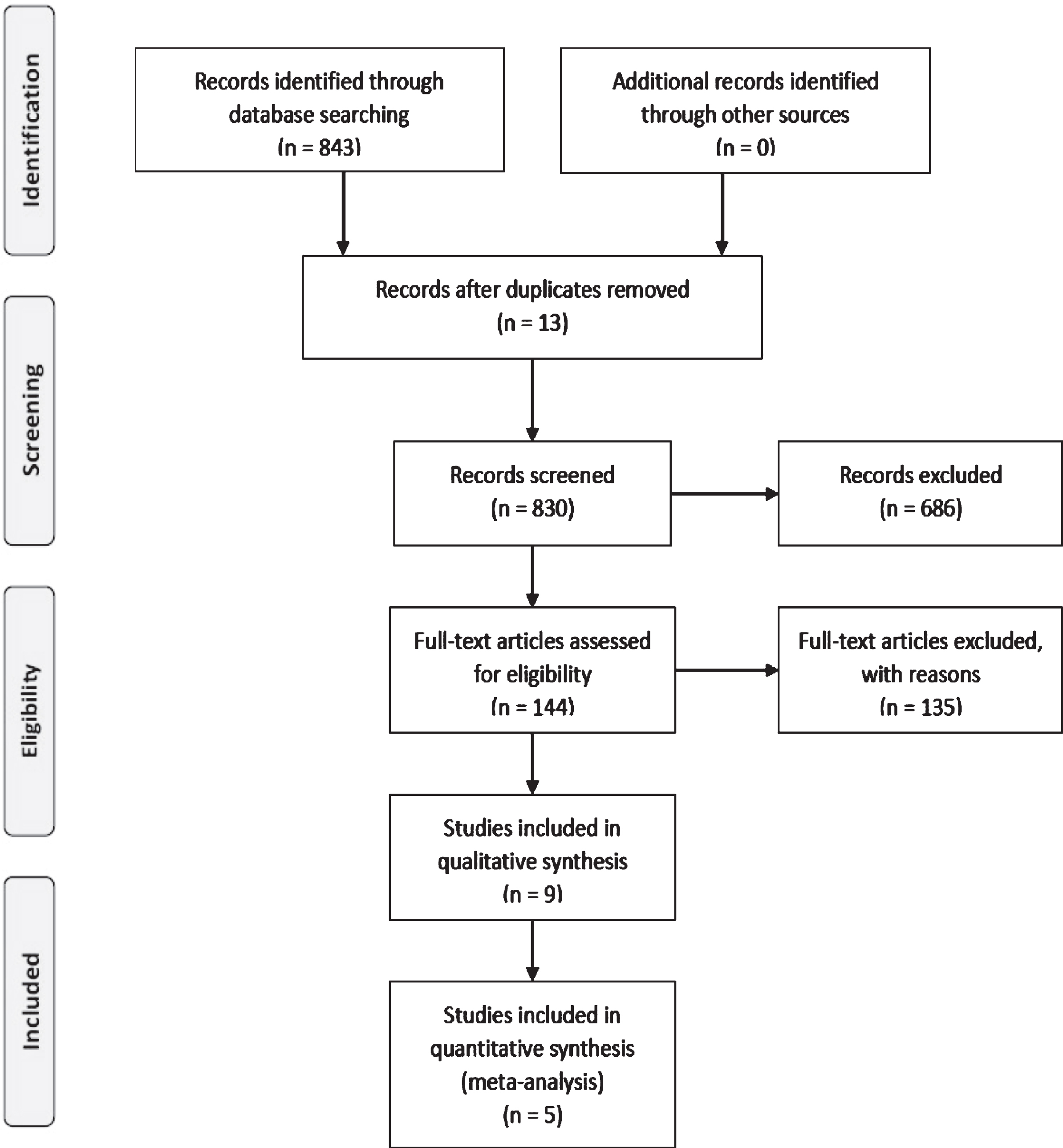
Flow diagram of search strategy.
The inclusion criteria were as follows: studies with the original text written in English; studies involving participants with acquired brain injuries after youth; studies that contained an intervention; and studies with randomized controlled trial designs. The exclusion criteria were as follows: studies based on animals; studies that did not contain an intervention (e.g. review articles, qualitative studies, and cross-sectional studies); and studies using drugs, injections, and acupuncture as the intervention.
Data extraction and quality assessments
The following data were extracted from the sel-ected studies: diagnosis of the participants, age, study design, assessment, interventions, and operational definition. Finally, nine studies were included (Appendix 1). A total of five studies were included in the meta-analysis. In particular, the following identifiable data were obtained from the studies: the means and standard deviations, t-tests results, and p values.
For the meta-analysis, the methodological quality of each study was assessed by two independent reviewers using the Jadad scale. The Jadad score is required in validating the quality of clinical trials, and blind raters assess the quality to limit the risk of introducing bias into the meta-analyses, and peer-review process. In addition, the nine articles were classified according to intervention and the analysis of type of interventions.
Data synthesis and analysis
The following information was extracted: year of publication, first author, period, number of persons with acquired brain injury in each group, age of participants enrolled, types of intervention, and assessment tools. We analyzed nine studies using the PICO concept for systematic reviews and extracted the following from the selected studies: patient, intervention, comparison, and outcome. Five studies analyzed the effectiveness of participation-based interventions using meta-analysis and assessed the level of evidence of qualitative studies using the PE-Dro scale. The level of evidence was evaluated using the PEDro scale for assessing the quality of criteria used in the studies. The PEDro scale is used to assess the amount and quality of evidence for interventions. The maximum PEDro score is 10. Two points are attributed for “blinding” of the subjects receiving interventions and therapists delivering interventions. Because such blinding is often not possible in many trials involving interventions in sports, the maximum score can only be 8 (Maher et al., 2008; Maher et al., 2003).
To conduct a quantitative meta-analysis, this study performed calculations by computing the standardized difference of mean scores. This study completed all analyses using the Comprehensive Meta-Analysis program (Borenstein et al., 2005). The effect size was calculated by the mean difference, standard deviation, and sample size in each group between the experimental and control groups. The effect size for participation-based interventions in persons with acquired brain injury was determined using a standardized mean difference and a 95% confidence interval (CI) in a fixed-effect mode. To estimate the effect size in this meta-analysis, we calculated the means and standard deviations, and the exact p-values. The effect size of the participation-based interventions in persons with acquired brain injury was interpreted as large if the effect size was greater than 0.8, moderate if it was greater than 0.5, and small if it was greater than 0.2 (Cohen, 1988). In addition to estimating the effect size in numerical order, a forest plot was used to visually depict the estimated value of the studies handling the effect and the confidence interval of the effect size.
Results
General characteristics of the studies
The data from the nine articles were presented in accordance with the principle of PICO (Patients, Intervention, Comparison, and Outcome), a method used to systematically sort out the results of all studies (Appendix 1). Among the nine studies that reported on the effects of participation-based interventions, the average number of participants was 46.44±19.00 (range: 16– 67) and the average period of the intervention was 8.22±5.58 (range: 2– 3) weeks.
Results of systematic review
This study reviewed nine studies to provide evidence to support participation-based interventions for persons with acquired brain injury and to identify a target outcome when applying participation-based interventions.
Regarding type of intervention, errorless goal management training was most applied for participation based intervention (Bertens et al., 2016; Bertens et al., 2016), similar to treatment program was goal management training + Lifelog (Cuberos-Urbano et al., 2018) and goal management training combined with problem solving (Spikman et al., 2010). In the re-maining five articles, there were in group based combined with individual occupation based support program (Ownsworth et al., 2008), immediate Mitii program (Sakzewski et al., 2016), resource facilitation program (Trexler et al., 2016), Instrumental activity daily of living self-awareness training (e.g. IADL self-awareness training) (Goverover et al., 2007), and participation focused outpatient treatment (Bender et al., 2016) (Table 1).
Type of interventions
Type of interventions
GMT (Goal management training), IADL (Instrumental activity daily of living).
This study reviewed nine studies to provide evidence to support participation-based interventions for persons with acquired brain injury and to identify a target outcome when applying participation-based interventions.
Regarding type of intervention, errorless goal management training was most applied for participation based intervention (Bertens et al., 2016; Bertens et al., 2016), similar to treatment program was goal management training + Lifelog (Cuberos-Urbano et al., 2018) and goal management training combined with problem solving (Spikman et al., 2010). In the re-maining five articles, there were in group based combined with individual occupation based support program (Ownsworth et al., 2008), immediate Mitii program (Sakzewski et al., 2016), resource facilitation program (Trexler et al., 2016), Instrumental activity daily of living self-awareness training (IADL self-awareness training) (Goverover et al., 2007), and participation focused outpatient treatment (Bender et al., 2016) (Table 1).
Five studies analyzed the effectiveness of parti-cipation-based interventions using meta-analysis and assessed the level of evidence of qualitative studies using PEDro scale. All five studies were of high quality (PEDro scale > 5) (Table 2).
Methodological quality of meta-analysis studies
Methodological quality of meta-analysis studies
In this meta-analysis, the effect sizes of studies investigating the efficacy of participation-based interventions in improving participation ranged from 0.08 to 0.57. The overall effect size of 0.32 can be interpreted as moderate with a 95% CI [0.08, 0.57 (p < 0.05) (Fig. 2).
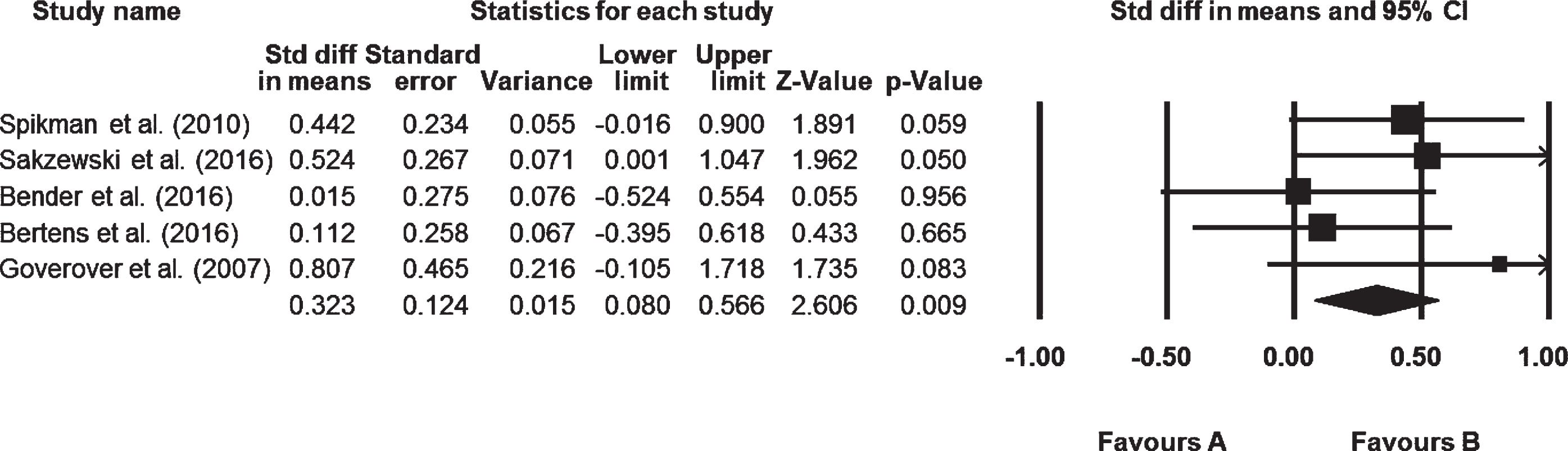
Forest plot showing individual effect sizes.
The Cochran’s Q-value of 3.83 (p = 0.42) in our test of statistical heterogeneity indicates no significant heterogeneity. Both the fixed-effects and random-effects models showed an effect size of 0.21, providing further evidence of the lack of statistical heterogeneity among the studies included in the present meta-analysis (Table 3).
Heterogeneity
Analysis of the funnel plot showed five values distributed in every section, acquiring an asymmetric funnel shape, with more values falling on the right-hand side of the mean effect size plot. Thus, the results were considered reliable, as no significant publication bias was found (Fig. 3).

Funnel plot of publication bias.
The purpose of this study was to provide evidence to support participation-based interventions for persons with acquired brain injury and to identify a target outcome when applying participation-based interventions. In addition, it was aimed at explaining and enhancing understanding of participation-based intervention methods in which people with acquired brain injury participate in daily life through a systematic review. Thus, this study provided evidence supporting the participation of people with acquired brain injury.
The intervention program mostly used for par-ticipation-based interventions was goal management training. A variant method of goal management training was the errorless goal management training, goal management training combined with problem solving, and goal management training+Lifelog. In goal management training, patients are taught a strategy to keep the selected everyday goal and the corresponding task steps active in their working memory. Patients are trained to monitor their performance during the execution of the task steps and to check if they are still aware of all further steps that lead to the goal. In errorless goal management training, the acquisition and execution of task steps are trained using errorless learning techniques, such as the use of visual and verbal (feed-forward) instructions and cue cards (Bertens et al., 2016). In addition, the goal management training combined with Lifelog involved recoding with the sense cam/ActiHeart (Cuberos-Urbano et al., 2018). The goal management training combined with problem solving was a multifaceted treatment aimed at improving the eight executive functional aspects of the Ylvisaker’s conceptual fra-mework: self-awareness, goalsetting, planning, self-initiation, self-monitoring, self-inhibition, flexibility, and strategic behaviour (Spikman et al., 2010).
Moreover, various interventions described below were applied to participation-based interventions for persons with acquired brain injury. Group-based support interventions were also combined with ind-ividualized occupation-based support interventions. Group-based support interventions targeted the dev-elopment of metacognitive skills (self-awareness and use of compensatory strategies) through group-based psycho-education, peer and facilitator feedback, and goal setting. Individualized occupation-based intervention focused on client-cantered goals and associated occupational activities considered important and meaningful to the individual (Ownsworth et al., 2008). In the immediate Mitii program, Mitii was a multi-modal web-based rehabilitation pro-gram, comprising cognitive, visual perceptual, upper limb, and gross motor training. Mitii was accessed via the internet and uses Microsoft Kinect (2nd generation; Microsoft Research, Redmond, WA, USA) to track body movements (Sakzewski et al., 2016). The resource facilitation program was provided according to the model described in “Resource Facilitation: Indiana Best Practices Manual for Return-to-Work or Return-to-School”. The major roles and functi-ons of the resource facilitation team members were resource facilitator, local support network leader, and clinical management (Trexler et al., 2016). In the IADL self-awareness training, participants were asked to predict their performance before completing each task. They were also asked to assess their performance immediately following the completion of each task. If a participant identified a specific problem while performing the task, he/she was asked to think of a strategy to help make task performance better and easier (Goverover et al., 2007). The par-ticipation-focused outpatient treatment (in German: teilhabeorientierte ambulante Maßnahme; TEAM) was for patients and their relatives to learn to deal with specific everyday challenges in the ICF domains of self-care, home life, and mobility using a partici-pation-focused outpatient program known as TEAM in line with its initials in German. The TEAM intervention also closely integrated relatives and evaluated patients in their real home environments (Bender et al., 2016).
This study analyzed five studies to identify applications for effective participation-based interventions in acquired brain injury. The overall effect size of ap-plying participation-based interventions for persons with acquired brain injury was found to be 0.32, a statistically significant result indicating that cognitive therapy has a small effect. No significant heterogeneity or publication bias was identified. It may also have affected the results of small effect size because few studies have utilized meta-analysis. Based on the results of this research, it is proposed that an effective method of conducting participation-based interventions for persons with acquired brain injury be developed. This meta-analysis is the first attempt to examine the empirical evidence regarding the eff-ectiveness of participation-based interventions for persons with acquired brain injury. The effect size of participation-based interventions for persons with acquired brain injury found in the present investigation was smaller than expected. Therefore, there is insufficient evidence to support the clinical benefit of participation-based interventions to improve outcomes in acquired brain injury.
According to Linden and collegue, they reviewed interventions to facilitate participation with rehabilitation interventions among adults with acquired brain injury. Regarding the rehabilitation setting, most of the behavioral interventions took place in an inpatient setting, and rehabilitation compliance/compliance was evaluated. In addition, metacognitive interventions were primarily established in an outpatient or home setting and were evaluated for goal achievement or participation (Linden, Glang, & McKinlay, 2018). This review suggested that interventions may be successful in increasing participation, but ideally should be tailored to the individual’s abilities and circumstances.
Persons with acquired brain injury cannot adapt to various stimuli from the community due to a variety of problems. Acquired brain injury, which req-uires long-term rehabilitation, requires intervention to participate in any way in their environment. How-ever, it is difficult to apply participation-based interventions clinically because the severity and disease progression are different for each patient. In this study provided evidence to support participation-based int-erventions for persons with acquired brain injury and to identify targeted outcomes when applying participation-based interventions for systematic re-view and meta-analysis.
However, in this study, only randomized controlled trials were reviewed in the search process, which may be a limitation since quasi-experimental design, single-subject design, qualitative research, review articles, and unpublished articles were excluded. For this reason, further research should be conducted through a broader search for studies on acquired brain injury.
Conclusions
Finally, the purpose of this study was to investigate participation-based intervention methods that are effective in persons with acquired brain injury via meta-analysis and to assess methods and targeted outcomes of participation-based interventions by conducting a systematic review. At this study, there was insufficient evidence to support the clinical benefit of participation-based interventions to improve outcomes in acquired brain injury and provided evidence to support participation-based interventions for persons with acquired brain injury. Therefore, this study provided evidence to support participation-based interventions in communities of persons with acquired brain injury. Based on the result of this study, it will be helpful to incorporate in communities the application of participation-based interventions to persons with acquired brain injury.
Footnotes
Table A1
Characteristic of included studies (N = 9) GMT (Goal management training), TEAM (in German: teilhabeorientierte ambulante Maßnahme), IADL (Instrumental activity daily of living).
Study
Participants
Intervention
Outcome measurements
Outcome
Intervention / groups
Session/time
Bender et al., 2016
Fifty-three patients
•Participation focused
6 hours every
•Goal Attainment Scale
There was difference between participation focused
who had sustained
outpatient treatment
weekday for
•Functional Independence
outpatient treatment (TEAM) and standard treatment
an acquired
group (n = 26)
4 weeks
Measure
on the Functional Independence Measure scale.
brain injury
•Control group
•EuroQol -5D
Moreover, improvements were seen at 12 months.
(n = 27)
•Short-Form 36
•WHO Disability Assessment
Schedule
•German New Appraisal
Assessment: Nursing
Care Caregiver Strain Index
Bertens,
Sixty-seven patients
•Errorless GMT
1-hour individual
•Dysexecutive Questionnaire
No significant interaction effects between these three
Kessels,
with executive
group (n = 33)
sessions,
•Cognitive Failures Questionnaire
types of outcome measures and the two forms of GMT
Boelen, &
impairments after
•Conventional GMT
administered
•Executive Function Index
were found. Performance on two executive tests improved
Fasotti,
acquired brain
group (n = 34)
twice a week
•Executive Observation Scale
and daily executive function problems as reported by
2016
injury
for 4 weeks
•RAND-36
the participants and proxies diminished.
Bertens,
Sixty with
•Errorless GMT
1 hour 8 sessions
•Dysexecutive Questionnaire
Higher age was associated with better everyday task
Fasotti,
acquired
group (n = 30)
given twice a week
•Cognitive Failures Questionnaire
performance after conventional goal management training,
Boelen, &
brain injury
•Conventional GMT
for 4 weeks
•Executive Function Index
whereas higher IQ was associated with better performance
Kessels,
group (n = 30)
•National Adult Reading Test
after errorless goal management training.
2016
•RAND 36
Cuberos-
Sixteen patients
•GMT + Lifelog (n = 8)
1 hour session per
•Dysexecutive Syndrome Questionnaire
GMT alone was associated with significant changes
Urbano et al., 2018
with acquired brain
•GMT only (n = 8)
week for 7 weeks
•Quality of Life after Brain Injury
of overall quality of life.
injury involving
executive dysfunction
Goverover,
Twenty participants
•IADL self-awareness
3 weeks, with one
•Assessment of awareness of disability
Compared to the control group, the intervention significantly
Johnston,
with a diagnosis of
training group (n = 10)
session per day on
•Self-Regulation Skills Interview
improved IADL performances and self-regulation.
Toglia, &
acquired brain
•Control group (n = 10)
2– 3 days of
•Assessment of Motor and Process Skills
DeLuca,
injury between the
each week.
•Satisfaction with quality of care
2007
ages of 18– 55
•Awareness Questionnaire
•Community Integration Questionnaire
Ownsworth,
Ownsworth Thirty-
•Group based
3 hours per week
•Brain Injury Community
The combined intervention was associated with maintained
Fleming,
five participants
support (n = 12)
for 8 weeks
Rehabilitation Outcome Scale;
gains in performance and satisfaction.
Shum,
with acquired
•Individual occupation
•Patient Competency Rating Scale;
Kuipers, &
brain injury
based support (n = 11)
•Canadian Occupational
Strong, 2008
•Combined group (n = 12)
Performance Measure
Spikman,
Seventy-five
•Management training
1 hour, twice a
•Behavioral Assessment of the
Multifaceted treatment program group has resulted
Boelen,
participants with
combined with program
week for 3 months
Dysexecutive Syndrome
in significant improvements of executive functioning
Lamberts,
acquired brain
group (n = 38)
•Dysexecutive Questionnaire
in daily life, lasting at least 6 months post-treatment.
Brouwer, &
injury
•Control group (n = 37)
•Executive Observation Scale
Fasotti, 2010
Sakzewski,
Fifty eight
•Immediate Mitii
30 minutes per day,
•Assessment of Motor and Process Skills
There were no differences between groups
Lewis,
with a minimum
group (n = 29)
6 days per week,
•Canadian Occupational Performance
on the primary outcome.
McKinlay,
of 12 months post
•Wait list
over 20 weeks
Measure
Ziviani, &
acquired brain
group (n = 29)
•Assisting Hand Assessment
Boyd, 2016
injury between the
•Test of Visual Perceptual Skills
ages of 8– 16
•Jebsen, Jebsen– Taylor Test of Hand Function
•Melbourne, Melbourne Assessment
of Unilateral Upper Limb Function
Trexler,
Forty four
•Resource facilitation
Every 3 month
•Vocational Independence Scale
Participants randomized to the resource facilitation
Parrott, &
outpatients with
group (n = 22)
monitoring of
•Mayo-Portland Adaptability Inventory-4
group demonstrated a significant advantage in terms
Malec, 2016
acquired brain
•Control group (n = 22)
employment
•Global Severity Index of the Brief
of rate and timing of return to productive
injury between the
status until
Symptom Inventory-18
community-based work relative to control participants.
ages of 18 – 60
15 months
•The Orientation Log and Cognitive Log
•Functional Independence Measure