
Abstract
Background:
The integration of therapeutic approaches is increasingly recommended for children with cerebral palsy, to enhance outcomes. Nevertheless, clinicians still opt for separate or combined therapies based on little credible knowledge.
Objective:
This study endeavored to evaluate the effect of botulinum neurotoxin-A (BoNT-A) injection and reciprocal neuromuscular electrical stimulation (rNMES) and their combination on the upper extremity function in children with spastic hemiplegia.
Methods:
Sixty-four children with spastic hemiplegia (aged 6– 10 years) were randomly assigned to four treatment-based groups [group I (BoNT-A), group II (rNMES), group III (combined BoNT-A and rNMES), and group IV (Control)]. All children received a physical rehabilitation program, thrice/week over three months. Unilateral upper-limb function, bimanual hand function, and real-time arm-hand function were assessed using Melbourne Assessment (MA), Assisting Hand Assessment (AHA), and Pediatric Motor Activity Log (PMAL) scales respectively pre-treatment, post-treatment, and at 6 months follow-up.
Results:
Post-treatment, group III achieved greater improvement in MA, AHA, and PMAL compared to other groups (all P < 0.05), and the difference remained in favor of group III at the follow-up (all P < 0.05).
Conclusions:
This study suggests that BoNT-A and rNMES combined are more effective than either of them alone to enhance upper-extremity function in children with spastic hemiplegia.
Keywords
Introduction
Cerebral palsy (CP) is the most frequent cause of motor disability during childhood (Jones, Morgan, Shelton, & Thorogood, 2007). Hemiplegia is a type of CP refers to the unilateral involvement of the body and accounts for about 25% of all CP diagnosis (Koman, Smith, & Shilt, 2004). Children with hemiplegic CP have trouble with the motor function of the involved upper limb (UL) attributable to a combination of; spasticity, reduced muscle strength, increased muscle co-activation, lack of selectivity, and other motor deficits (Elnaggar, 2016; Elnaggar, 2020a; Gordon, Lewis, Eliasson, & Duff, 2003; Elnaggar, 2020b, Elnaggar, 2020c). The focus of treatment, particularly in children with hemiplegic CP, is to enhance the functional use of paretic limbs. In physical rehabilitation of the UL, therapists emphasize the repeated practice of uni-manual and bi-manual motor skills in diverse contexts (Elshafey & Elnaggar, 2015; Novak et al., 2013; Sakzewski, Ziviani, & Boyd, 2009; Sakzewski, Ziviani, & Boyd, 2014). But, owing to the perception of movement limitation, children are usually resistant to participate actively in the repeated practice of motor activities (Elnaggar, 2016).
Blocking of the nerve impulse by injection of a powerful neurotoxin such as botulinum toxin-A (BoNT-A) to the spastic muscle can facilitate movement. The BoNT-A exerts its effect by impeding the release of acetylcholine (a facilitatory chemical neurotransmitter) from the presynaptic cholinergic nerve terminals into the myoneural junction leading to reduction of muscle activity (Hallett, 2018). BoNT-A displays local diminution of dominating-spasticity and thereby providing the recipient with an opportunity for 3 – 4 months to effectively employ their treated arm in daily activities. Further effects of BoNT-A injection are increasing range of motion, preventing contractures, and thus delaying the need for surgery. The existing literature on the BoNT-A injection in children with CP revealed that there was sufficient evidence that these injections are effective in relieving spasticity (Wasiak, Hoare, & Wallen, 2004), promoting inter-limb muscle coordination (Degelaen et al., 2013), improving balance and gait (Elnaggar, 2014; Elnaggar & Elbanna, 2019), enhancing UL function (Lowe, Novak, & Cusick, 2006), and optimizing the overall motor potential (Heinen et al., 2010).
Reciprocal neuromuscular electrical stimulation (rNMES) is the type of electrical stimulation in which the opposed muscle groups are activated cyclically in an alternating pattern (Elnaggar & Elbanna, 2019). The rNMES imitates the normal agonist/antagonist firing sequences. It has been shown to aid in minimizing the cortical excitability of the spastic muscles and in augmenting the strength of the anti-spastic muscle as well (Tinazzi et al., 2005). Therefore, rNMES has the potential to treat motor deficits that clearly affect a child’s ability to change the direction of movement. Previous experimental studies have found that the use of rNMES was effective in treating spasticity, improving calf/anterior tibial muscle sequencing, enhancing motor function and postural stability, and improving spatiotemporal and kinematic gait parameters in children with CP (Badawy & Ibrahim, 2015; Elnaggar, 2014; Elnaggar & Elbanna, 2019).
Clinical reasoning and expert perspective suggest that the application of rNMES in the post-injection period enhances the BoNT-A effect and improves outcomes (Elnaggar & Elbanna, 2019). The rationale for this combination therapy is that the post-injection period of denervation provides an opportunity for the dominating-spasticity to be controlled and spastic muscle to be stretched. In the meantime, rNMES alongside physical exercises can be used to direct the children’s response to a more organized activation pattern of the spastic and anti-spastic muscles and to help them to learn new and more functional motor patterns. To our knowledge, no previous studies evaluated the effect of rNMES as an adjunctive to BoNT-A injection of the UL, and thereby no evidence that this combination will enhance the functional performance. Rather, the available studies evaluated the add-on effect of BoNT-A to the standard physical rehabilitation (Fehlings, Rang, Glazier, & Steele, 2000; Lowe et al., 2006; Speth, Leffers, Janssen-Potten, & Vles, 2005). Therefore, this is the first study known to evaluate the effect of rNMES as an adjunctive to BoNT-A injection on the UL function in children with hemiplegic CP.
The main objectives of this study were to identify 1) if either the BoNT-A or rNMES alone is effective in improving the upper-limb function in children with hemiplegic CP, 2) if BoNT-A and rNMES in conjunction are more effective than either of them alone.
Methods
Study design
This was a single-blinded, randomized clinical trial performed between August 2018 and October 2019. The study was registered in the Iranian Registry of Clinical Trials and assigned the following number: IRCT20200215046504N1. The research protocol was approved by the Institutional Research Ethics Committee (RHPT/0018/0064) at the College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia. The study procedures followed the ethical principles regarding human experimentation adopted in the sixth revision of the Declaration of Helsinki 2008. Parents/Guardians signed a consent form to authorize their children to participate.
Participants
Sixty-four children with CP were recruited from a large tertiary referring hospital. Children were included if they had a confirmed diagnosis of spastic hemiplegia, aged between 6 and 10 years, had spasticity of grade II or III according to Modified Ashworth Scale (Ansari, Naghdi, Arab, & Jalaie, 2008), were mentally able to comply with verbal instructions during evaluation and treatment, and had a normal or corrected visual and auditory function. Children were excluded if they; had contractures limiting the arm and hand function, received a BoNT-A injection in the involved UL in the past six months, were advised against stopping of spasticity-relieving medications during the study period by their neuro-pediatrician, had any prior casting, or underwent orthopedic or neuromuscular surgery of the involved UL within the past year or planned for during the study, and if they had uncontrolled seizures.
Sample size estimation
To avoid type I error, a power analysis was conducted before data collection using PASS software version 15.0.5 (NCSS, Kaysville, UT, USA). In a one-way ANOVA study, a group-sample of 14 subjects was obtained from the 4 groups whose means are to be compared. The total sample of 56 subjects achieves 80% power to detect differences among the means versus the alternative of equal means using an F test with a.05 significance level. The size of the variation in the means was represented by effect size (η²) equal to 0.46, which was estimated from the results of a small pilot study. We recruited up to 64 subjects to account for the possible dropout.
Randomization and allocation
Eligible children were allocated randomly into four treatment-based groups (I; BoNT-A, II; rNMES, III; combined BoNT-A and rNMES, IV; Control). We used a stratified random sampling technique to assign 16 subjects for each group. Four homogenous strata were created based on spasticity level on Modified Ashworth Scale and children’s age as follow: spasticity level 2 aged 6 - 8 years (n = 20); < 8 – 10 (n = 16) or spasticity level 3 aged 6 – 8 years (n = 24); < 8 – 10 (n = 4). A size-proportional sample was randomly taken from each stratum by an independent person. Afterward, these subsamples were combined to build a random sample for each group. Participants in the four groups were received a physical rehabilitation program. Moreover, participants in group I exposed to BoNT-A injection, participants in group II received rNMES, while the participants in group III submitted to BoNT-A and rNMES combined.
Assessment
All participants were assessed for the unilateral upper-limb function, bimanual hand function, and arm-hand, real-time function. The assessment took place at the baseline, post-treatment, and at 6 months follow-up. Where applicable, the rater was blinded to intervention assignments and was not part of this research at any stage of its implementation.
Primary outcomes
2.5.1.1. Unilateral upper-limb function. Melbourne Assessment (MA) was used to measure the quality of the unilateral upper-limb function. It is a clinician-based performance assessment tool that is applicable to children with neurological dysfunctions from 5 to 15 years and has been indicated as a reliable tool for measuring unilateral upper-limb function in children with CP, with a very high internal consistency of the test items (Cronbach’s α = 0.96) and high inter-rater (ICC = 0.95) and intra-rater reliability (ICC 0.97) for total test scores (Randall, Carlin, Chondros, & Reddihough, 2001).
The test battery consists of 16 criterion-referenced items that include reaching, grasp, release, and manipulation skills. Children were assessed while sitting at a table using a test kit including the items needed for test administration and was videotaped for later precise assessment. Each item was assessed from a videotape on the components that make up the assessment-criteria of that item, including the range of movement, accuracy, fluency, dexterity, and speed. Test items were assessed on 3-, 4-, or 5-point scales, which allocate scores on the items according to the success and movement quality, with a total of 37 sub-scores for all items. The sum of the sub-scores was recorded as the raw score. The raw scores were then converted to a percentage score and used for data analysis. The highest possible score for the complete test is 122 points. A higher percentage indicates a better quality of unilateral upper-limb function (Bourke-Taylor, 2003).
2.5.1.2 Bimanual hand function. The bimanual hand function was measured using the Assisting Hand Assessment (AHA) version 4.4. AHA is a standardized and criterion-referenced test used with children as young as 18 months and up to 12 years of age and had a unilateral disability, to quantify how effectively they use the affected hand interactively with the non-affected hand to complete bimanual tasks. Evidence of an excellent inter-rater and intra-rater reliability is reported in research (Holmefur, Krumlinde-Sundholm, & Eliasson, 2007). AHA comprises 22 test items, each item rated on a 4-point scale, resulting in a raw score range from 22 to 88 points, with the higher scores indicating higher ability. AHA outcomes were presented in two score levels: 1) ordinal level data (raw scores and percentage scores that indicate the age-percent of the score attained), 2) interval level measures (unit logits ranging from 10.18 to 8.70 and logit-based 0– 100 AHA-unit). In this study, the outcomes are presented as interval level data (logit-based 0– 100 AHA-unit) (Krumlinde-Sundholm, 2012).
Secondary outcomes
2.5.2.1. Arm-hand, real-time function The pediatric motor activity log (PMAL) was used for the rating of the arm-hand, real-time functional activities. It is a parent-report measure, developed to capture the spontaneous use of the involved UL of children with hemiplegic CP who are aging from 7 months up to 8 years in real-life situations (Wallen, Bundy, Pont, & Ziviani, 2009). The PMAL comprises 22 activity items requiring the use of the hand and the arm. The PMAL tasks range from fine motor tasks (picking up or holding small objects) to gross motor tasks with arm involvement (reaching out). It also includes tasks that require unilateral hand use (turning a knob) and bilateral hand use (pulling and pushing a toy or holding a handle on a ride). Parents or guardians reported “how often” their children use the involved UL to perform the functional activities on a six-point scale from 0 (not used) to 5 (normal; used 90% – 100% of the time). They also rated “how well” their children completed these functional activities on a six-point scale from 0 (not used) to 5 (normal; the weaker arm did the activity normally). The total scores for the “how often” scale and the “how well” scale were derived from the mean of the items scores for each of them. A fair criterion-related validity of PMAL was reported by Lin et al. when compared with the 2nd edition of Peabody Developmental Motor Scale. It is markedly responsive to the functional changes after intervention with minimally detectable changes of 0.67 for the “how often” scale (i.e., PMAL amount of use) and 0.66 for the “how well” scale (i.e., PMAL quality of movement) (Lin et al., 2012).
Interventions
Children were assigned randomly into four treatment groups (group I; BoNT-A, group II; rNMES, group III; combined BoNT-A and rNMES, and group IV; Control). The schedule of the individual and combined treatment is illustrated in Fig. 1.

Schedule of the individual/combined treatments.
In accordance with the updates of the European consensus on the use of BoNT-A for children with CP (Heinen et al., 2010), participants of group I and III received a single set of intramuscular injection of BoNT-A (Botox®, Allergan PLC, Dublin, Ireland) after they were sedated using oral midazolam (0.5 mg/kg) to increase the injection tolerance. The dosage used was 0.5– 2 U kg–1/muscle group determined by the attending neuro-pediatrician, with a total dosage of 12 U kg–1 (and never exceeded a maximum total dose of 400 U). An ultrasound-guided injection procedure was used to determine the locations of injection. The principal investigator and the neuro-pediatrician decided together which muscle groups to inject during a comprehensive arm-hand function assessment. The flexor carpi ulnaris, pronator teres, and adductor pollicis were the most injected muscles, whereas the flexor carpi radialis, flexor pollicis brevis, brachioradialis, and biceps brachii were less often indicated for BoNT-A injection.
rNMES application
Children of groups II and III received three 15-minute rNMES per week for three successive months. The rNMES was applied before exercises when children attended for the exercise sessions. A computerized electrical stimulator (Vectra®2C; Chattanooga, TS, USA) with a dual-channel stimulating unit was used, each channel had two small-size, rectangular carbon rubber electrodes (3×5 cm) enclosed in two spongy covers. Children assumed a comfortable sitting position with the forearm kept in the neutral position, skin areas where the electrodes planned to be applied were carefully cleaned with alcohol swabs, then the electrodes were attached as follows: Channel 1 was applied to the wrist flexors (one electrode on the common flexor origin at the medial epicondyle of the elbow the other electrode on the lower third of the palmar aspect of the forearm proximal to the wrist joint) and channel 2 was applied to wrist and finger extensors (one electrode on the common extensor origin at the lateral epicondyle of the elbow and the other electrode on the lower third of the dorsal aspect of the forearm proximal to the wrist joint) (Fig. 2) The system was set to the reciprocal mode to produce alternating stimulation of the wrist flexor and extensor muscles. Simulation parameters were: symmetrical biphasic square waveform, frequency of 30 Hz, a pulse width of 300μs, the up- and down-ramp times were set on an individual basis to avoid the stretch-reflex from becoming elicited, alternating cyclic time (wrist 5 seconds for flexors and 10 seconds for extensors), the intensity was adjusted to the sensory threshold to acclimate the children to the stimulation and was then increased until the visible contraction was achieved.

Reciprocal neuromuscular electrical stimulation of wrist flexor and extensor muscles.
An exercise program based on the standard practice for physical rehabilitation of children with spastic hemiplegia was applied to the children of the four groups. The program incorporated uni-manual and bi-manual functional activities with a general goal of improving arm-and-hand use in the activities of daily living (ADL). It was a neurodevelopmentally-based, task-oriented, and was tailored for each participant depending on the functional status. The motor activities included reaching out, grasping, releasing, transferring, carrying, in-hand manipulation, and bilateral hand use skills. The program also emphasized the functional strength training, hand weight-bearing exercises, stretching exercises, and bilateral-arm and inter-arm coordination exercises. The program was administered in three 60-minute sessions per week over three consecutive months by three pediatric rehabilitation specialists. For the children in groups I and III, the program commenced one week after BoNT-A injection.
Statistical analysis
Data were analyzed using statistical software Stata version 15.1 (Stata Corp, College Station, TX). The level of statistical significance was set at α= 0.05 for all analyses. A preliminary analysis including a check for data normality, a plot for each variable, and a descriptive summary was performed. One-way ANOVA and Fisher’s exact tests were used to check the comparability of the study groups at the entry for the baseline characteristics. A one-way ANOVA test was computed to detect the between-group differences with respect to the dependent outcome measures. When a statistical significance was demonstrated on the ANOVA test, post-hoc analysis with Bonferroni correction was applied to compare the study groups in pairs. A repeated measure ANOVA test was used to detect the within-group differences.
Results
Participants’ allocation and follow-up are illustrated in Fig. 3. The potential participants were 92 children. Of them, 64 children fulfilled the inclusion criteria and were randomized. Four children discontinued (three children did not complete the assigned intervention, one child lost during the follow-up for unknown causes). Therefore, data of the remaining 60 children were included in the analysis. Participants’ baseline characteristics are displayed in Table 1. The study groups were not significantly different in the age, gender distribution, anthropometric variables, involved side, or the baseline spasticity level (P > 0.05).
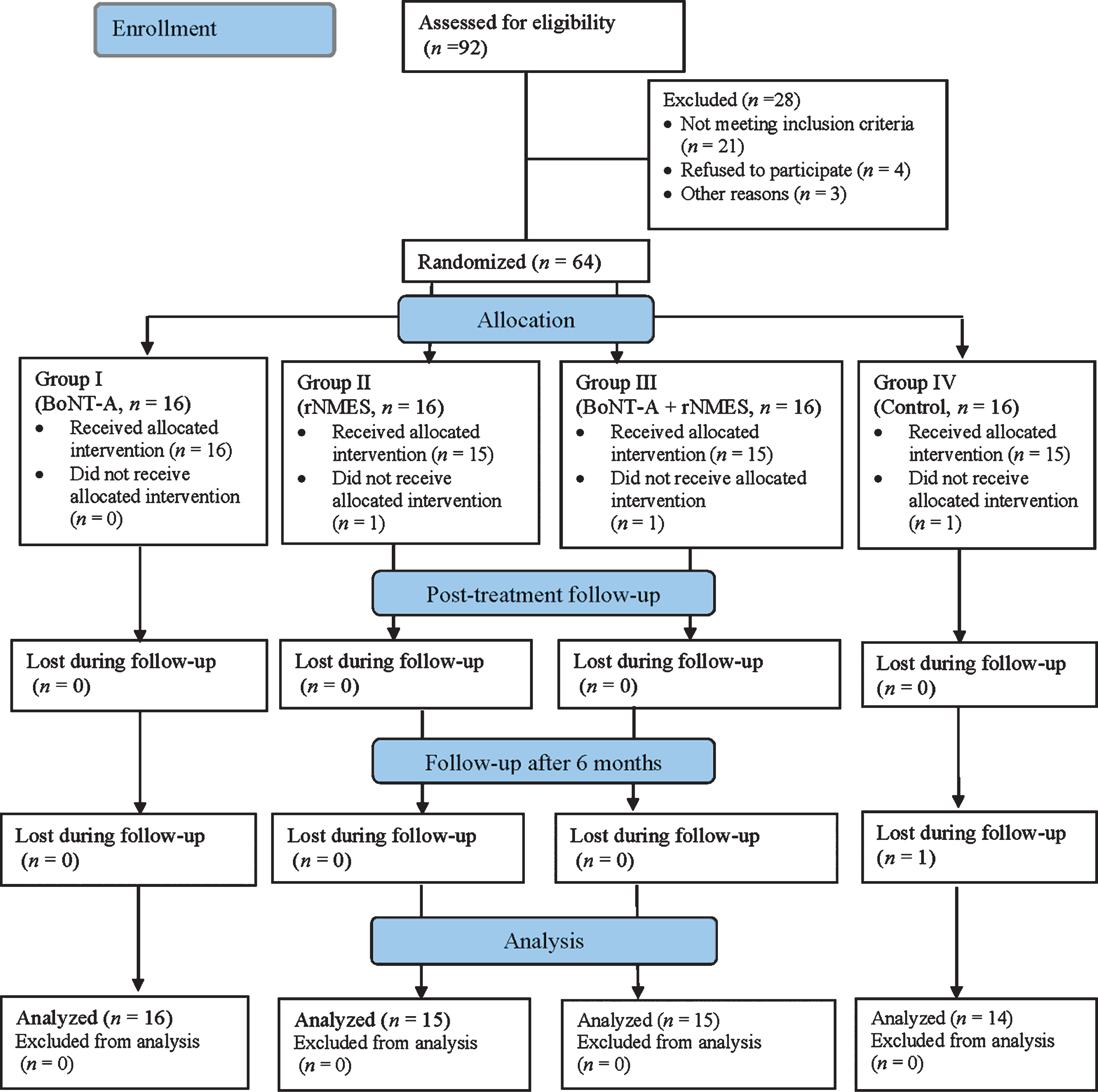
Schematic illustration of the study design.
Participants’ baseline characteristics
Data expressed as mean±SD except gender involved side, and spasticity level distribution expressed as n(percentage), BMI: body mass index, Dt: dominant, Non-Dt: non-dominant, asignificance (ANOVA test), bexact significance (Fishers’ exact test).
Change scores for the primary outcome measures are outlined in Table 2. No significant between-group differences were observed concerning the pre-treatment MA or AHA scores (P > 0.05). From the pre- to the Post-treatment, the MA and AHA scores demonstrated a statistically significant improvement in groups I, II, and III (P > 0.05) and that improvement was maintained at the follow-up after 6 months as compared to the pre-treatment scores in these groups. A statistical difference was found between the study groups in the post-treatment and follow-up mean values of MA (P = 0.0001, and P = 0.001 respectively) and AHA (P > 0.0001) scores. The post-hoc analysis demonstrated that group III had the highest improvement in post-treatment MA scores compared to group I (P = 0.034), II (P = 0.01), or IV (P < 0.0001). At the follow-up, the improvement difference remained in favor of group III compared to group II (P = 0.035) and IV (P = 0.001), but the difference lost compared to group I (P = 0.071). Also, group III achieved greater improvement in the post-treatment AHA scores than group I (P = 0.013), II (P = 0.001), or IV (P < 0.0001), and that differences continued in favor of group III at the follow-up when compared to group I (P = 0.006), II (P = .001) or IV (P < 0.0001).
Changes in MA (unilateral upper-limb function) and AHA (bimanual hand function) within and between the study groups
Data expressed as mean±SD, *significant at P < 0.05.
Changes in the PMAL are listed in Table 3. No significant differences were found between the study groups pre-treatment, regarding the amount and quality of arm-hand use (P > 0.05). From pre- to post-treatment, there were significant improvements in the amount and quality of arm-hand use in groups I, II, and III (P > 0.05), and these improvements were sustained at the follow-up. A statistical difference was found between the study groups in the post-treatment and follow-up amount and quality of arm-hand use (P > 0.0001). The post-hoc analysis demonstrated that group III had the highest improvement in the post-treatment and follow-up amount of arm-hand use compared to group 1, II, or IV (P > 0.0001). Furthermore, group III achieved greater improvement in the post-treatment quality of arm-hand use than group I (P = 0.023), II (P = 0.0003), or IV (P > 0.0001), and that differences continued in favor of group III at the follow-up when compared to group I (P = 0.028), II (P = 0.0002) or IV (P > 0.0001).
Changes in PMAL (arm-hand, real-time function) within and between the study groups
Data expressed as mean±SD, *significant at P < 0.05.
Increased spastic/anti-spastic muscles’ co-contra-ction in the UL is not just a disordered motor-control problem but also detrimental to the arm-hand function in children with spastic hemiplegia. It has been suggested that excessive coactivation of the spastic UL flexors opposes the moment of the force created by the weak anti-spastic extensors and thereby restraining movement (Pontén, Fridén, Thornell, & Lieber, 2005; Smits-Engelsman, Rameckers, & Duysens, 2004). Investigating UL function after therapeutic approaches to improve opposing muscles’ synergism can help to optimize the rehabilitation process.
This study provided empirical evidence on the BoNT-A and rNMES influence on the upper-limb function measured by MA, AHA, and PMAL in children with spastic hemiplegia. The findings demonstrated that the use of BoNT-A and rNMES combined was more advantageous than either of them alone in improving unilateral upper-limb function, bi-manual hand function, and optimizing the amount and quality of use of the involved UL in the real-time functional activities in the post-treatment and follow-up occasions. The clinical implication of these findings is that the enhancement of the post-injection effects on some of the important factors that contribute to the upper-limb function by application of rNMES can reduce the frequency of BoNT-A injection, and would further help the clinician to choose between the mono- and combined applications based on empirical evidence.
Previous investigations that have considered the combination of BoNT-A and rNMES in the treatment of children with CP were limited to three studies that considered the application of the treatment to the lower limbs. In the first study, children with spastic diplegia achieved remarkable improvement in static and functional balance measures when the rNMES was applied to the ankle dorsi/plantar flexor muscles after they were exposed to BoNT-A injection into the calf muscles (Elnaggar, 2014). In the identical fashion of BoNT-A and rNMES application, the second study assessed ankle kinematics and dynamic limits of postural stability in a sample of children with diplegic CP (Elnaggar & Elbanna, 2019). As opposed to the independent application, coupling of BoNT-A and rNMES produced notable correction of ankle displacement angles during gait, and enhancement of postural control. The third study was a single-subject design that included five children with CP. Three of them received a single set of BoNT-A injection followed by 4-weeks of rNMES applied during walking to the tibialis anterior from the push-off until the initial contact phase to prevent foot slapping, and to the gastrocnemius starting from the initial contact phase to allow weight transfer. The results of that study showed a trend toward an increase in the isometric strength of the plantar flexor muscles after rNMES, although children did not demonstrate changes in the walking speed (Seifart, Unger, & Burger, 2010). Despite the methodological differences, the results of this study support in part the significant role of the integration of BoNT-A and rNMES in the treatment of children with spastic CP. Further, a pilot study adopted the single-subject design with repeated measures investigated the coupling effect of BoNT-A and another mode of electrical stimulation (i.e., functional electrical stimulation) in a heterogeneous sample of eight children with spastic CP (Galen, Wiggins, McWilliam, & Granat, 2012). The BoNT-A administered to the gastrocnemius of the affected side and the electrical stimulation was delivered to the tibialis anterior muscle during gait, in two consecutive phases. In general, results indicated notable improvement in the ankle dorsiflexion angle during the gait swing phase and the foot contact pattern. Despite the earlier research uncovered the promising effect of the BoNT-A and rNMES combined on many aspects of activity limitations in children with spastic CP, they have focused on the lower extremity only and no or very little checks have been made to the UL functionality. This may highlight the importance of the results of this study which provided evidence on the effect of BoNT-A and rNMES combined on the motor function of the involved UL in children with spastic hemiplegia.
However, the stand-alone effect of either the BoNT-A or rNMES cannot be disregarded. Results from this study suggested that each of these interventions had the potential to improve the unilateral upper-limb function, bi-manual hand function, and the real-time arm-hand function. The scientific evidence on the use of BoNT-A to improve the activity capacity of the involved UL in children with spastic CP has been demonstrated in the literature. An earlier trial tested the hypotheses that BoNT-A into the UL muscles of children with spastic hemiplegia (aged between 2.5 to 10 years) would improve the UL-related function (Fehlings et al., 2000). BoNT-A was administered to the biceps muscle, volar forearm muscles, or the adductor pollicis muscles at a dosage of 2 to 6 U/kg. Many functional tests, specifically regarding the quality of the UL skills test and parent-proxy self-care domain of pediatric evaluation of disability inventory were blindly conducted. Both measures showed significant improvement favoring the BoNT-A group. Also, a randomized trial investigated the influence of UL BoNT-A against placebo injection alongside an intensive physical therapy program on the UL function and the competence in ADL in 27 children with spastic hemiplegia (Ferrari et al., 2014). The BoNT-A group achieved a significant increase in UL function (measured by the assisting hand assessment scale) and the competence in ADL (as quantified by the goal attainment scale). Further, a recent analysis of the outcomes of BoNT-A injection (mean dosage was 0.8 to 7.26 U/kg) previous to an individualized physical and occupational therapy program in cases of CP with UL involvement was executed ((Karaca, Ünlü, Köse, Gönen, & Çakcı, 2016). The analysis revealed remarkable progress of the UL function as reflected by the pediatric functional independence measure, UL physician’s rating scale, and the 9-holes peg test. It is quite interesting to speculate on how the BoNT-A contributed to the improvement of UL motor-related functions. This may be attributed to the neuromuscular blockade effect of BoNT-A on the spastic muscles, as it helps to lengthen the shortened muscles, enhance the peak torque generated by the anti-spastic muscles, and to affect the main mechanism that impairs the active function around the joint through neutralization of the spastic/ant-spastic muscle action (Gracies, 2004). This could, in fact, help the children to learn and build up new motor patterns and stimulate the central neuroplastic changes in the brain, especially in 3– 6 months post-injection.
Also, there is some evidence in the published literature on the individual contribution of rNMES in the treatment of children with CP. A previous study evaluated the adjunctive effect of rNMES applied to the quadriceps and hamstring muscles in children with spastic diplegia (Badawy & Ibrahim, 2015). The children allocated to the rNMES intervention arm exhibited significant improvement in standing and walking function and in the potential to adjust the knee joint alignment. A further investigation explored the consequences of rNMES application to the ankle dorsi/plantar flexor muscles in children with spastic diplegia. The findings of that investigation showed a considerable gain in the mediolateral and anteroposterior postural stability and ankle dorsiflexion in the gait-swing phase (Elnaggar & Elbanna, 2019). An explanatory trial on adult patients with stroke examined the effect of alternating electrical stimulation of the extensor and flexor muscles of the hand (de Kroon, IJzerman, Lankhorst, & Zilvold, 2004). The results demonstrated a significant increase in the arm function on the action research arm test. The mechanism whereby the rNMES works could be explained by the reduced cortical excitability of spastic wrist flexors and improved strength of the weak wrist extensors by virtue of the alternating stimulation since the rNMES enables graded agonist-antagonist action through activation of the reciprocal inhibition mechanism. Furthermore, repetitive cyclic stimulation of the wrist flexor and extensor muscles help to modify the co-activation to a near-normal pattern, which the child can learn and build up in the brain (Elnaggar & Elbanna, 2019; Tinazzi et al., 2005).
Worthy of note that, this study has some limitations. First, the single-blind design, where the children and their families were knowledgeable about the treatment groups. This might have implications on the parents-reports on the PMAL measure. Second, despite parents were instructed to refer to the same items in the environment each day when answering questions on the PMAL to ensure consistency, many factors may have influenced parental rating and were difficult to be controlled by the researcher. These factors may include fatigue, sickness, potential changes in the home environment, and/or any other factors that may impose different levels of difficulty and/or requires different motor behaviors. The upcoming studies should think about the double-blind design and the more robust study of the real-time upper-limb function.
Conclusion
The findings of the current study provide evidence on the effectiveness of the individual application of BoNT-A and rNMES in combination with physical rehabilitation in improving the upper-limb function in children with spastic hemiplegia. However, BoNT and rNMES combined had the potential to produce significantly favorable effects.
Declaration of interest
The authors of this work claim no conflicts of interest
Footnotes
Acknowledgments
This project was supported by the Deanship of Scientific Research at Prince Sattam Bin Abdulaziz University under the research project # 2020/03/16921