
Abstract
Background:
Although Constraint-Induced Movement therapy (CIMT) has been deemed efficacious for adults with persistent, mild-to-moderate, post-stroke upper-extremity hemiparesis, CIMT is not available on a widespread clinical basis. Impediments include its cost and travel to multiple therapy appointments. To overcome these barriers, we developed an automated, tele-health form of CIMT.
Objective:
Determine whether in-home, tele-health CIMT has outcomes as good as in-clinic, face-to-face CIMT in adults ≥1-year post-stroke with mild-to-moderate upper-extremity hemiparesis.
Methods:
Twenty-four stroke patients with chronic upper-arm extremity hemiparesis were randomly assigned to tele-health CIMT (Tele-AutoCITE) or in-lab CIMT. All received 35 hours of treatment. In the tele-health group, an automated, upper-extremity workstation with built-in sensors and video cameras was set-up in participants’ homes. Internet-based audio-visual and data links permitted supervision of treatment by a trainer in the lab.
Results:
Ten patients in each group completed treatment. All twenty, on average, showed very large improvements immediately afterwards in everyday use of the more-affected arm (mean change on Motor Activity Log Arm Use scale = 2.5 points, p < 0.001, d′ = 3.1). After one-year, a large improvement from baseline was still present (mean change = 1.8, p < 0.001, d′ = 2). Post-treatment outcomes in the tele-health group were not inferior to those in the in-lab group. Neither were participants’ perceptions of satisfaction with and difficulty of the interventions. Although everyday arm use was similar in the two groups after one-year (mean difference = –0.1, 95% CI = –1.3–1.0), reductions in the precision of the estimates of this parameter due to drop-out over follow-up did not permit ruling out that the tele-health group had an inferior long-term outcome.
Conclusions:
This proof-of-concept study suggests that Tele-AutoCITE produces immediate benefits that are equivalent to those after in-lab CIMT in stroke survivors with chronic upper-arm extremity hemiparesis. Cost savings possible with this tele-health approach remain to be evaluated.
Keywords
Introduction
Chronic, upper-extremity hemiparesis affects between 55–75% of stroke survivors (Lai, Studenski, Duncan, & Perera, 2002). Deficits in more-affected arm function are associated with poor quality of life (Nichols-Larsen, Clark, Zeringue, Greenspan, & Blanton, 2005). Nonuse of the more-affected arm is associated with a reduction in its representation in the brain (Gauthier, Taub, Mark, Barghi, & Uswatte, 2012; Liepert et al., 2000). Notably, Constraint-Induced Movement therapy (CIMT) has been shown to produce both large improvements in use of the more-affected arm (Taub et al., 1993; Taub, Uswatte, King, et al., 2006) and corresponding increases in its representation in the brain (Gauthier et al., 2008; Liepert et al., 2000).
Although multiple randomized controlled trials (RCTs) support the efficacy of CIMT for rehabilitating use of the more-affected arm after stroke (Hatem et al., 2016) and several prominent national organizations recommend CIMT as a standard of care (Heart and Stroke Foundation of Canada, 2019; Rudd, Bowen, Young, & James, 2017; Winstein et al., 2016), CIMT is not offered on a widespread clinical basis in many countries (Gauthier et al., 2017; Pedlow, Lennon, & Wilson, 2014; Viana & Teasell, 2012). Among barriers to its dissemination on a more widespread basis than now are its cost (Lum, Uswatte, Taub, Hardin, & Mark, 2006; Viana & Teasell, 2012), scarcity of personnel trained in its administration (Morris & Taub, 2014; Takebayashi et al., 2018; Viana & Teasell, 2012), and requirement for patients to visit the treatment facility on multiple days (Pedlow et al., 2014). CIMT, in its signature form, demands 35 hours of one-on-one, face-to-face therapy that is typically administered by a skilled physical or occupational therapist (PT or OT), whose services are costly (Taub, Lum, Hardin, Mark, & Uswatte, 2005). The number of PTs and OTs with specialized training in administering CIMT is still modest (Morris & Taub, 2014; Pedlow et al., 2014; Viana & Teasell, 2012); moreover, they are clustered at major medical centers (D. Morris, personal communication, April 15, 2020). The original form of CIMT requires 10 visits to a treatment facility (Taub et al., 1993; Taub, Uswatte, King, et al., 2006); later, distributed forms of CIMT require that number or more (Dettmers et al., 2005; Shi, Tian, Yang, & Zhao, 2001). These features of CIMT mean patients with modest incomes, who live far from medical centers, or who have mobility limitations have to clear high hurdles to gain access to this efficacious therapy. Given that these hurdles are not unique to CIMT (Chae, Kim, Lee, & Park, 2020; Johnson, Rai, Barathi, Mendonca, & Bustamante-Valles, 2017), methods for surmounting them may have implications for increasing access to other efficacious physical rehabilitation interventions.
To address these needs, authors E.T., G.U., and P.L. initiated a program of research with the aims of automating the delivery of CIMT, which lowers labor costs, and making CIMT available on a remote basis, which permits patients to receive treatment in their own homes. Lum, Taub, and colleagues first developed a workstation that automated the delivery of CI therapy, named Automated CI Therapy Extension (AutoCITE)(Lum et al., 2004). AutoCITE consisted of a circuit of 8 upper-extremity task stations with built-in sensors that fed forward information about a patient’s interactions with the stations to a personal computer (PC) running custom-made software. The software displayed visual feedback about the patient’s performance on a monitor and controlled the flow of the training tasks. Taub, Uswatte, and colleagues then showed that treatment outcomes even when the therapist was in contact with a patient for only a quarter of the total treatment time were equivalent to the outcomes observed in previous studies of one-on-one, face-to-face CIMT (Taub et al., 2005). Next, Lum, Uswatte, and colleagues showed in a case series that when tele-rehabilitation was simulated by placing the therapist in a different room in the laboratory from the patient and workstation, treatment outcomes were similar to outcomes in previous CIMT studies (Lum et al., 2006). Other approaches to delivering CIMT in the home with reduced therapist effort include using a gamified virtual-reality platform to implement motor training (Gauthier et al., 2017) and teaching patients to carry out training tasks at home on their own with a family caregiver playing the role of a coach (Barzel et al., 2015). In another in-home variant of CIMT (Lima et al., 2014), no attempt was made to reduce the amount of therapist effort; training was delivered via home visits by a therapist.
The next step in the program of research described above is to test whether the results from the case series, in which tele-rehabilitation was simulated, can be confirmed in a study with a RCT design in which the participants in the tele-rehabilitation group actually train at home with therapy monitored remotely by a trainer in the laboratory. This small, proof-of-concept study, which is the first RCT to directly compare automated, tele-rehabilitation delivery to standard delivery of CIMT, answers that question. Participants were randomized in equal numbers to automated CIMT in the home on a tele-rehabilitation basis with one-on-one, remote supervision from a trainer or to standard CIMT in the laboratory with one-on-one, face-to-face supervision from a trainer. Answers to questions about cost savings, including those that might be achieved by reducing the amount of therapist support, will await future studies.
Methods
Participants
Participants were recruited from individuals who contacted our laboratory in response to news reports about CIMT, as well as referrals from the inpatient consultation liason service and outpatient clinic of the physiatry department at our University medical center. Potential participants were screened using structured telephone interviews and then structured examinations by a physical or occupational therapist and a neurologist. To be enrolled, candidates had to be adults ≥1-year after stroke and display mild-to-moderate motor impairment of the more-affected arm along with substantial nonuse of that arm. The methods for determining the degree of arm motor impairment and nonuse are described in Supplementary Table 1, as are the other inclusion and exclusion criteria that were taken directly from previous CIMT studies from our laboratory in stroke patients with a similar degree of more-affected motor impairment (Taub et al., 1993, 2013, Taub, Uswatte, King et al., 2006). Three additional inclusion criteria were specific to this study. To permit the tele-rehabilitation workstation to be installed by project staff, all participants had to live in a neighborhood in which Hi-speed Internet was available and that was within a two-hour driving distance of the laboratory. In addition, participants had to have adequate vision and audition and technological knowhow to perform the training tasks on the workstation with coaching from project staff, if needed, after a brief instruction session. Participant characteristics are described in Section 3: Results.
Apparatus
The design of AutoCITE was modified to create an upper-extremity rehabilitation workstation suitable for placement in a stroke patient’s home (Brennan et al., 2011). This version, named Tele-AutoCITE, had a smaller footprint than AutoCITE (approximately 107×107 vs. 120×240 cm), was portable, and had Internet-based audio-visual and data links that enabled a therapist at a treatment center to monitor the progress of a patient at home. The workstation featured seven task stations, which were mounted on a table, that permitted the performance of 10 tasks (see Supplementary Figure 1 and Supplementary Table 2). The task stations had built-in sensors that fed forward information about a patient’s interactions with the stations to a PC mounted beneath the table. The PC ran custom-made software that controlled the flow of the training tasks and displayed instructions for the patient and visual feedback about the patient’s performance on a touchscreen monitor mounted on the table (see Supplementary Figure 2 and 3). The patient sat in a chair with a stable, lockable base facing the task devices and monitor, which were arrayed along a semicircular cutout in the table to permit easy access by simply swiveling the chair (Supplementary Figure 1). Counterpart software installed on the PC of the therapist in the treatment center permitted the therapist to remotely control the training activities and monitor the progress of the participant via a Hi-speed Internet connection (see Supplementary Figure 4). Set-up and connection to the Internet of the workstation in a participant’s home required an approximately 4 hour home visit by the project engineer. If a Hi-speed Internet connection was not already present, installation of a Hi-speed connection by an Internet service provider was arranged by the engineer beforehand. The design and operation of Tele-AutoCITE is described in detail in Brennan et al., 2011.
Interventions
Participants were randomly assigned, using a computer-generated random numbers table, to in-lab or tele-health delivery of CIMT. Participants in both groups received 3.5 hours of treatment per day for 10 consecutive weekdays with one-on-one supervision from a trainer for the entirety of each treatment session. The amount, intensity, and organization of the motor training in the two group was the same. Three hours of each treatment session were committed to motor training following shaping principles (see Section 2.3.1); 30 minutes were committed to a package of procedures designed to promote changes in motor behavior outside the treatment setting (see same section). During the period committed to motor training, participants were trained to perform upper-extremity tasks exclusively with the more-affected arm in sets of ten 30 s trials with one minute rest intervals between trials and ten minute rest intervals between tasks. This schedule resulted in the completion of 7.5 tasks per session, with 37.5 minutes spent performing the tasks and 142.5 minutes spent resting. Participants in both groups were asked to place a physical restraint on the less-affected arm to discourage use of that arm both in and outside of the treatment sessions for a target of 90% of waking hours over the two-week treatment period. During the first month after treatment, participants received four telephone calls; they were part of the package of behavior change procedures. During these calls, which took place one week apart, trainers interviewed participants about use of their more-affected arm at home and guided problem-solving about any perceived or actual barriers to use of that arm. The face-to-face, in-lab CIMT protocol is described in detail in Morris & Taub, 2014. The principles that underlie CIMT are given briefly below, followed by (a) synopsis of the face-to-face, in-lab CIMT protocol and (b) description of the in-home, tele-health protocol, which employed Tele-AutoCITE. Cardiovascular safety procedures implemented in both groups are summarized in Supplementary Table 3.
CIMT principles
CIMT has four major components. First is intensive training of the more-affected arm on functional tasks. Second is organization of this training following shaping principles, which are measuring patients’ performance, providing frequent positive feedback, and incrementally increasing the requirements for the task as patients gain mastery (Skinner, 1938; Taub et al., 1994). Third is a group of behavior change procedures designed to transfer gains from the treatment setting to the real world, termed the “Transfer Package”(Taub et al., 2013). Fourth is discouraging use of the less-affected arm by requiring that participants wear a physical restraint on it for the portion of waking hours of the treatment period that it is safe to do so. The overall purposes of the four components are to (a) countercondition learned nonuse (Taub, 1980; Taub, Uswatte, Mark, & Morris, 2006), i.e., a learned tendency to avoid using the more-affected arm, (b) improve the quality, speed, and ease of more-affected arm movement, (c) promote transfer of the therapeutic gains to everyday life, and (d) drive neuroplastic brain changes that support use of the more-affected arm (Taub, Uswatte, & Mark, 2014).
Face-to-face, in-lab CIMT protocol
Participants in the in-lab CIMT group received treatment face-to-face on an outpatient basis in our clinical research facility. Supplementary Table 4 outlines the schedule of activities on a typical treatment day. In this group, training tasks were selected from a bank of 120 assembled by our laboratory based on the individual needs of a participant. Examples of tasks are lifting a stacking cones, spooning beans from a bowl to a plate, and picking up coins.
In-home, tele-health CIMT protocol
Participants in the tele-health CIMT group, as noted, received the same type, amount, and intensity of training except that treatment was carried out in the home using Tele-AutoCITE with remote supervision provided by the trainer in our clinical research facility.
A day or two before the first treatment session, the trainer accompanied the project engineer on the home visit necessary to set-up the Tele-AutoCITE workstation (see Section 2.2). While the engineer was doing so, the trainer oriented the participant to the study procedures (Supplementary Table 4). In addition, the trainer (a) negotiated a behavioral contract with the participant and a family caregiver, if available, about what activities the participant would attempt with more-affected arm and when the participant would wear a padded safety mitt on the less-affected arm outside of the treatment setting (b) showed the participant how to keep the daily diary on use of the more-affected arm at home and compliance with wearing the padded safety mitt, (c) identified tasks to assign the participant as homework, and (d) demonstrated how to put on the padded-safety mitt. After setup of Tele-AutoCITE was complete, the trainer helped the engineer to properly position the Tele-AutoCITE chair and showed the participant how to use Tele-AutoCITE. Instruction was carried out until the participant was able to reliably demonstrate independent operation of Tele-AutoCITE.
A typical training session (Supplementary Table 4) was similar to that for participants in the CIMT group except that training was done at home with Tele-AutoCITE and supervision was remote. The trainer made a phone call to the participant 30 minutes ahead of time to alert the participant to the upcoming session. The trainer selected the training tasks based on the individual needs of the participant and set the shaping parameters (e.g., distance to target) based on the participant’s training records from previous sessions. To initiate the session, the trainer “unlocked” the Tele-AutoCITE workstation, activated the audio-visual and data-stream links, and greeted the participant. (The workstation was locked in-between sessions to prevent participants from engaging in training outside of sessions, which would result in an unequal amount of training in the two arms of the study.) The trainer carried out the same elements of the Transfer Package that she did for participants in the CIMT group at the outset of a session (Supplementary Table 4). The Tele-AutoCITE permitted display of any forms necessary to carry out these procedures on the touch-screen monitor. Then, the trainer prompted the participant to start the first training task. Although the Tele-AutoCITE software automatically directed the participant, the trainer continuously monitored the progress of the participant using the audio-visual and data-stream feeds. She provided encouragement, answered questions, and altered the task and shaping parameter selections when needed.. The trainer completed the same Transfer Package elements as she did for participants in the CIMT group at the end of a session (Supplementary Table 3). Last, the trainer “locked” the Tele-AutoCITE workstation.
Measures
Pre- and post-treatment testing was conducted the first weekday before and after treatment in the laboratory with all participants. Long-term follow-up was collected after the one-year anniversary date for completing treatment. Follow-up data from the WMFT, which had to be done in the laboratory, were missing from five in the Tele-AutoCITE group and six in the CIMT group because several participants were not able to return to the laboratory for testing. Hence, long-term follow-up data are reported here only for the Motor Activity Log (MAL), which could be administered over the telephone. The primary endpoint is the change from pre- to post-treatment on the MAL.
The MAL is a scripted, structured interview that is reliable and valid (Uswatte, Taub, Morris, Vignolo, & McCulloch, 2005; Uswatte, Taub, Morris, Light, & Thompson, 2006). Among evidence for validity is a strong correlation (r, range = 0.71–0.91, p’s≤0.01) with an objective measure of amount of movement in the life situation, accelerometry (Uswatte, Foo, et al., 2005). Participants are asked to rate the quality of movement and amount of use of their more-affected arm in daily life on 30 upper-extremity activities over a specified period (e.g., last week, yesterday). Only the quality of movement rating, named the Arm Use scale, is reported typically because the two ratings are highly correlated and hence redundant (Taub, Uswatte, King, et al., 2006; Taub et al., 2013; Uswatte, Taub, et al., 2005; Uswatte et al., 2006). Scores on the 11-point Arm Use scale range from 0 (no use of the more-affected arm) to 5 (use of the more-affected arm that is good as pre-stroke). The test score is the mean of the item scores. A minimal clinically important difference (MCID) has been identified by Lang and colleagues as 1.0 points (Lang, Edwards, Birkenemeier, & Dromerick, 2008).
The Wolf Motor Function Test (WMFT) is a valid and reliable measure of in-laboratory motor capacity, (i.e., maximum ability) when a participant is asked to complete a task with the more-affected arm (Morris, Uswatte, Crago, Cook, & Taub, 2001; Wolf et al., 2001). Time is recorded to complete each of 15 upper-extremity actions or tasks, which range from raising the more-affected arm from lap to tabletop to picking up a pencil with the more-affected hand. The test score is the mean of the item Performance Time scores after transforming them into a rate (repetitions per minute; RPM)(Hodics et al., 2012). Items that cannot be completed in 120 s are assigned a score of 0. Performance Rate scores range from 0 to 60 repetitions per minute. A MCID has been identified by Lin and colleagues as 29% of the test score (Lin et al., 2009).
A Participant Opinion Survey (POS) assessed perceptions about the therapeutic value and difficulty of the interventions before and after treatment. Before treatment, participants rated the statement “I believe that CI therapy will benefit me.” Response options on the 7-point Likert scale ranged from 1 (Strongly disagree) to 7 (Strongly agree). After treatment, participants answered the question “How satisfied are you with your CI therapy program overall?” Response options on this Likert scale ranged from 1 (Not at all satisfied) to 7 (Extremely satisfied). In addition, before/after treatment, participants answered the question “How difficult do you think your CI therapy program will be/has been overall?” Response options on this Likert scale ranged from 1 (Not at all difficult) to 7 (Extremely difficult). Because MCID values for these items have not been established, we used a rule-of-thumb method, i.e., taking 30% of the score of interest, to determine these values.
Data analysis
One-tailed, repeated-measures t-tests were used to evaluate whether all participants, regardless of group assignment, showed improvement on the outcome measures from (a) pre- to post-treatment and (b) pre-treatment to long-term follow-up. One-tailed tests, along with 90% Confidence Intervals, were used because we hypothesized that both interventions would be of benefit to participants. As noted, multiple, prior studies have shown that in-lab CIMT produces large improvements on the MAL and WMFT (e.g., Taub et al, 1993 & 2006) and two have shown that similar improvements are observed when the AutoCITE workstation is used to provide CIMT in the lab with reduced therapist effort (Taub et al., 2005) and to simulate tele-rehabilitation (Lum et al., 2006).
The statistical test we used to compare outcomes in the two groups is illustrated in Fig. 1 and explained here. To evaluate if the outcome of tele-health delivery of CIMT was inferior to in-lab delivery, we constructed a two-tailed, 95% Confidence Interval (CI) around the difference between the mean post-treatment scores of the tele-health and in-lab groups on the outcome of interest. If the lower bound of the CI fell further below 0 than the MCID on the outcome of interest, we concluded that tele-health delivery produced an inferior outcome (Committee for Medicinal Products for Human Use, 2006). In other terms, we concluded that tele-health delivery was as good as in-lab delivery if the lower bound of our estimate of its benefit was not meaningfully worse than our estimate of the benefit of in-lab delivery. For the MAL and WMFT, post-treatment means were adjusted for any differences in pre-treatment values using an analysis of covariance model. For the POS items, observed rather adjusted means were used since the questions about satisfaction with and difficulty of the intervention were not administered before treatment and would not have been relevant then.
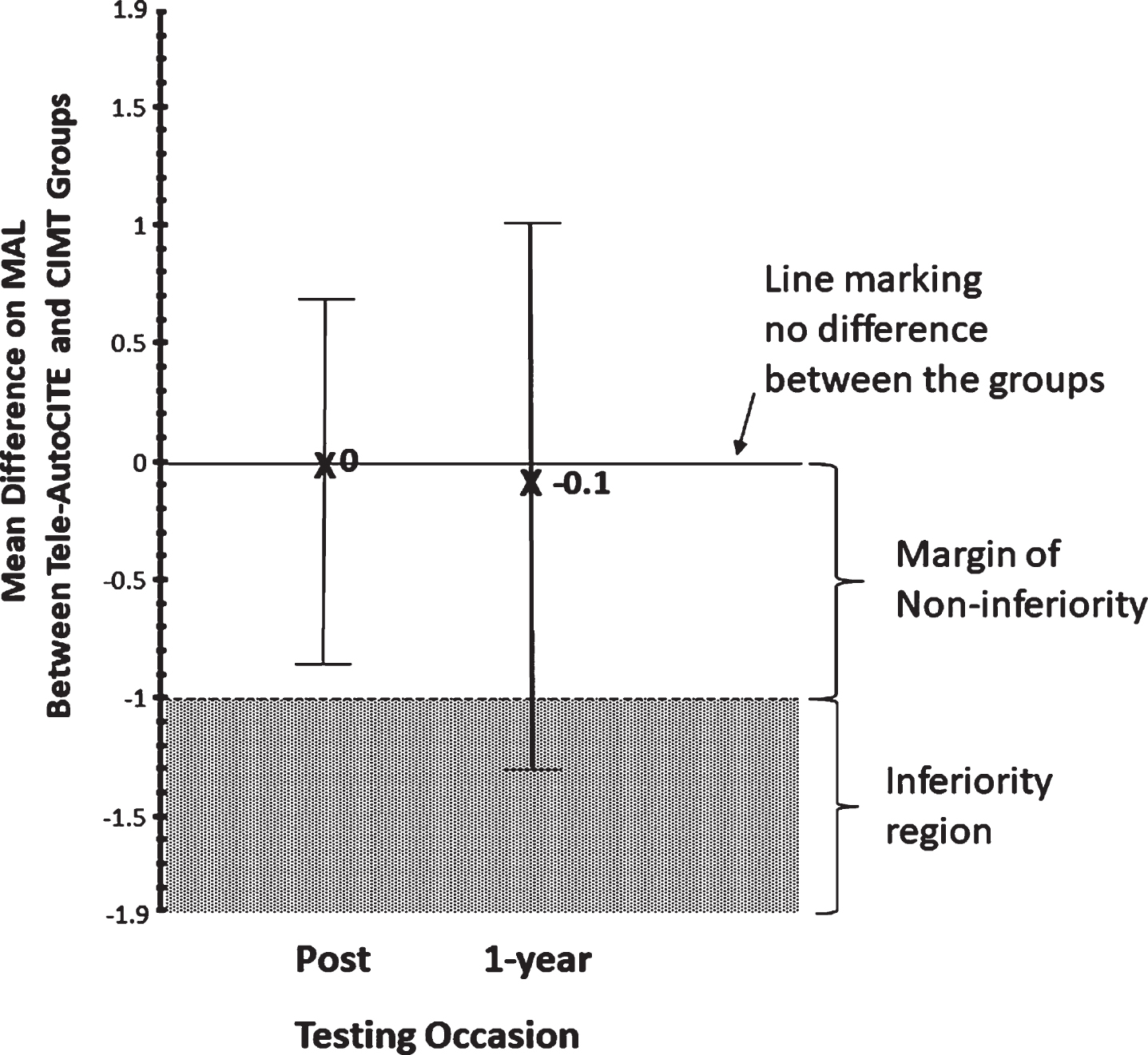
Test of non-inferiority. To compare everyday arm use after treatment in the two study groups, a two-tailed, 95% CI was constructed around the difference between the mean post-treatment MAL scores of the tele-health and in-lab groups. The same was done for the long-term follow-up scores. A MCID on the MAL is 1 point. The lower bound of the margin of non-inferiority was set to –1, i.e., one MCID below the value that marks no difference between the groups, i.e., 0. At post-treatment, the hypothesis that the MAL gains in the Tele-AutoCITE group were not worse than those in the CIMT group was supported: the lower bound of the CI (–0.8) fell within the margin of non-inferiority. In other words, the range of likely values of the difference in outcome between the two groups fell above the range of values marking an inferior outcome. At long-term follow-up, inferiority could not be ruled out. The mean difference between the two groups at follow-up was small and very similar to that at post-treatment: –0.1 vs. 0. However, because the precision of the estimate of the difference of the between the two groups fell at follow-up due to drop-out (cell size at post-treatment = 20, cell size at follow-up = 7), the CI expanded, with the result that the lower bound of the CI fell in the inferiority region. Note that least square means were used for this analysis; the post-treatment group means were adjusted for differences between the group means at pre-treatment using an ANCOVA model.
The primary analysis only included participants who completed both pre- and post-treatment testing (Per Protocol). We also completed sensitivity analyses with (a) the baseline observation carried forward (BOCF) for missing data and substitution of the group average (AVG) for any missing outcome values (Rubin & Sheiner, 1995). The BOCF analysis represented, in effect, a worst-case scenario, in which participants with missing data were assumed not to show any improvement, while the AVG analysis represented a “middle-of-the-road” scenario in which data were assumed to be missing-at-random or, in other words, in which participants with missing data were assumed to show as much improvement as those without missing data. A single outlying WMFT value in the TeleAutoCITE group was excluded from the primary analysis and treated as missing in the BOCF and AVG analyses. Values were considered outliers if they lay outside of bounds that were the interquartile range boundaries multiplied by 1.5 (Sun & Genton, 2011). The results of the primary analysis only are described below, except for the two tests for which the results of the three analyses differed. Results from all three analyses are reported in detail in Tables 2 3 along with a description of missing data in the footnotes.
Changes from pre-treatment to post-treatment and 1-year follow-up in the study groups
aFor the intention-to-treat, BOCF analysis, missing post-treatment or follow-up data were replaced with corresponding baseline values. For the intention-to-treat, AVG analysis, missing data were replaced with the group average for that testing occasion. For both the BOCF and AVG analyses, outliers were treated as missing data points. bCohen’s d′ is a repeated-measures effect size index; calculating this statistic involves dividing the mean of a set of changes scores by their standard deviation. Values ≥0.57 are considered large (Cohen, 1988). cAn outlier with respect to treatment change (29.1) was excluded from WMFT scores for the Tele-AutoCITE group. The results did not change meaningfully for the Tele-AutoCITE group when none were excluded: 6.9* (90% CI = 1.3–12.4), d′ = 0.7 (Per Protocol); 5.7 (90% CI = 1.0–10.4), d′ = 0.6 (BOCF); 6.9* (90% CI = 2.4–11.4), d′ = 0.8 (AVG). Nor did the results for all participants, i.e., those from both groups combined: 5.2* (90% CI = 2.3–8.2), d′ = 0.7 (Per Protocol); 4.4* (90% CI = 1.8–6.9), d′ = 0.6 (BOCF); 5.2* (90% CI = 2.8–7.7), d′ = 0.7 (AVG). Abbreviations: AVG = average; CI = confidence interval, CIMT = in-lab Constraint-Induced Movement therapy, BOCF = baseline observation carried forward, M = mean, MAL = Motor Activity Log, Tele-AutoCITE = in-home Telerehab Automated CI Therapy Extension, WMFT = Wolf Motor Function Test. *p < 0.05. Note that in the table statistical tests were only conducted on change scores for All, i.e., on data from both groups combined.
Differences between the study groups after treatment
aFor the BOCF sensitivity analysis, missing post-treatment or follow-up data were replaced with corresponding baseline values. For the AVG sensitivity analysis, missing data were replaced with the group average for that testing occasion. For both the BOCF and AVG analyses, outliers were treated as missing data points. bValues are least-square means from analysis of covariance models with pre-treatment scores entered as the covariate and group as the independent variable. Post-treatment scores for the POS items are not adjusted because corresponding pre-treatment scores do not exist for these items. cAn outlier was excluded from WMFT scores for the Tele-AutoCITE group. Mean post-treatment score values did not change meaningfully for the Tele-AutoCITE group when none were excluded: 36 (95% CI = 31–41) (Per Protocol); 35 (95% CI = 31–40) (BOCF); 36 (95% CI = 32–41) (AVG). Nor did the values for the difference at post-treatment between the means of the Tele-AutoCITE and CIMT group: 4 (95% CI = –4–11) (Per Protocol); 3 (95% CI = –3–9) (BOCF); 4 (95% CI = –3–10) (AVG). dOne participant who completed the protocol in the Tele-AutoCITE group did not provide a response to the POS Satisfaction and Difficulty items. eBOCF calculations were not conducted because there was no corresponding POS item at pre-treatment from which to carry forward an observation. fOn the POS Difficulty item, a seven indicates that a participant found the intervention to be extremely difficult. Hence, a negative difference score indicates that the TeleAutoCITE group found their intervention to be less difficult than the CIMT group. That is the opposite of all the other variables tabled, for which a negative difference score signifies a disadvantage for the TeleAutoCITE group. *Marks comparisons for which the outcome of the Tele-AutoCITE group was not inferior to that for the CIMT group. The values of the lower bound of the margin of inferiority for the MAL, WMFT, POS Satisfaction item, and POS Difficulty item were was –1, –10, –1.9, and 1.2. Footnote f to this table explains why the last number, unlike the others, is a positive value. Figure 1 explains the construction of the test of non-inferiority. Abbreviations: AVG = average; CI = confidence interval, CIMT = in-lab Constraint-Induced Movement therapy, BOCF = baseline observation carried forward, M = mean, MAL = Motor Activity Log, n/a = not applicable, Tele-AutoCITE = in-home Telerehab Automated CI Therapy Extension, WMFT = Wolf Motor Function Test.
The d′ statistic (Cohen, 1988) was used to quantify the effect size of the pre- to post-treatment changes observed. Calculation of this statistic requires dividing the mean of a set of changes scores by their standard deviation. Values ≥0.57 are considered large. Power was more than adequate (≥0.85) to test whether the outcome of the Tele-AutoCITE group was meaningfully worse than that of the CIMT group on the primary endpoint, i.e., pre- to post-treatment improvement on the MAL Arm Use scale.
Trial profile and initial participant characteristics
Out of 89 referrals, 24 were enrolled. Twelve were randomized to each group. Ten in each group completed treatment and post-treatment testing. Seven in each group completed testing after one-year. Figure 2 shows the flow of candidates through the study, and provides a breakdown of the reasons individuals were excluded or dropped-out at each stage. Table 1 enumerates several demographic, stroke, and attitudinal characteristics of the participants. There were no significant differences between the Tele-AutoCITE and CIMT groups for the characteristics tabled, including, notably, expectations about the benefit and difficulty of the interventions.

Trial profile. The Institutional Review Board at our University approved the study procedures. All participants gave written informed consent. The trial was registered with ClinicalTrials.gov (unique identifier: 01157195). The participant who was discontinued for being noncompliant went through the motions during the treatment sessions and did not carry out the homework assignments. We discovered partway through treatment that her only reason for taking part in the study was that her boyfriend thought it would benefit her. The participant for whom oxygen saturation levels could not be reliably detected by the pulse oximeter connected to the Tele-AutoCITE workstation was discontinued because monitoring oxygen saturation was part of the treatment session safety protocol. There were no adverse events related to participation in the study. In addition to the participant who developed pneumonia in the Tele-AutoCITE group, one participant in that group had a stomach virus and another had low blood pressure on one occasion and developed an infected toe on another. These two participants were able to continue with treatment after receiving appropriate care.
Initial characteristics of participants in the study groups
Note. Values are M (95% CI) for continuous data and number in class as a percentage of the total number in the group for categorical data. There were no significant differences between the Tele-AutoCITE and CIMT groups for the variables tabled. Two-tailed, independent samples t-tests with an α of 0.05 were used to test whether participants in the two groups differed before treatment in age, time since stroke, use of the more-affected arm in daily life (MAL), and more-affected arm motor capacity (WMFT). Fisher’s exact tests were used to examine differences in the distribution of sex, ethnicity, side of paresis, and side of dominance before stroke. Mann-Whitney U tests were used to examine differences in expectations about the benefit (POS Item 3) and difficulty (POS Item 1) of the interventions. Variable values for participants who completed the study (Per Protocol) were similar to those for all enrolled (All). aAn outlier (94.1) was excluded. Mean age in the Tele-AutoCITE group was higher when including these values: COMPLETERS, 63.1 years (95% CI = 52.5–73.7); ALL, 66.3 years (95% CI = 56.5–76.1). Note that the presence of the 94 year old in the Tele-AutoCITE group stacks the deck against experimental hypothesis, i.e., that tele-health delivery of CIMT is as good as in-clinic delivery. bNone of the participants were Hispanic. cTwo outliers (60.6, 30.0) were excluded. Mean time since stroke in the Tele-AutoCITE group was longer when including these values: COMPLETERS, 11.1 years (95% CI = –2.8–25.0); ALL, 9.6 years (95% CI = –1.7–21.0). As for the outlier with respect to age, the presence of the outliers with respect to time since stroke in the Tele-AutoCITE group stack the deck against experimental hypothesis. (The outlier with respect to age was also an outlier with respect to time since stroke.) dOne COMPLETER in the Tele-AutoCITE group did not provide responses to the POS survey. eBecause participants who did not complete the protocol did not provide responses to the POS survey, the values for ALL would be the same as for COMPLETERS. Abbreviations: CI = confidence interval, CIMT = in-lab Constraint-Induced Movement therapy, M = mean, MAL = Motor Activity Log, POS = Participant Opinion Survey, Tele-AutoCITE = in-home Telerehab Automated CI Therapy Extension, WMFT = Wolf Motor Function Test.
Regardless of the group to which participants were assigned, all, on average, showed very large improvements immediately after treatment in everyday use of the more-affected arm. Unless otherwise specified, results are reported for the primary, i.e., per protocol, analysis. The mean pre- to post-treatment improvement on the MAL Arm Use scale for participants who completed testing at both occasions was 2.6 points, 90% CI = 2.3—2.9, t(19) = 15, p < .001, d′ = 3.4. All participants, on average, showed large improvements over the same period in motor capacity of the more-affected arm. The mean improvement in WMFT Performance Rate was 4 repetitions per minute, 90% CI = 2—6, t(18) = 3.2, p = 0.007, d′ = 0.7. As noted, this analysis excluded an outlier. An alternate analysis, with similar results, that included the outlier is presented in a footnote to Table 2, which presents the results of the sensitivity analyses in addition to the primary analysis. Notably, the sensitivity analyses (BOCF, AVG) did not produce results that were substantially different from the primary analysis. Table 2, in addition, breaks out the results by study group. Only results of the omnibus analysis, i.e., for all participants combined, are described here because the findings in the two groups were similar. The same applies to the long-term follow-up results.
Satisfaction with the intervention received was high for all at post-treatment; the mean score on this POS item was 6.5 out of 7, 95% CI = 6.2—6.9. The estimate of the mean in the AVG analysis was similar: 6.5, 95% CI = 6.3—6.8. Perceived difficulty of the intervention received was moderate at post-treatment; the mean score on this POS item was 3.7 out of 7, 90% CI = 3.0—4.4. The estimate of the mean in the AVG analysis was similar: 3.7, 95% CI = 3.0—4.3. POS scores for each group are described in the next section and enumerated in Table 3. BOCF analyses were not performed because these post-treatment measures had no pre-treatment counterparts, i.e., baseline values were not available to carry forward.
After one-year, all still showed very large improvements from baseline in everyday use of the more-affected arm: mean MAL change = 1.9 points, 90% CI = 1.5—2.3, t(13) = 8.7, p < .001, d′ = 2.3. For participants who completed long-term follow-up (n = 14), the mean MAL score at pre-treatment was 1.1, 90% CI = 0.8—1.4, while the mean at post-treatment was 3.6, 90% CI = 3.2—4.0, and the mean at follow-up was 3.0, 90% CI = 2.5—3.5. In other terms, a 15%reduction in everyday use of the more-affected arm was observed from post-treatment to follow-up: mean change = –0.5, 90% CI = –0.8—–0.2, d′ = –0.8. Follow-up could not be collected from three in each group because these participants could not be contacted or declined to complete additional testing (Fig. 2). Similar gains at post-treatment for participants with and without long-term follow-up suggested that these missing data did not bias the long-term follow-up results; participants who completed follow-up reported a gain of 2.4, 90% CI = 2.0—2.8, while subjects who did not reported a gain of 2.8, 90% CI = 2.4—3.2. However, it was still possible that subjects who completed follow-up showed smaller decrements in arm use over the follow-up than subjects who did not. The pattern of results for the sensitivity analyses were similar to those for the primary analysis (see Table 2).
Comparison of outcomes in Tele-AutoCITE and CIMT groups
The pre- to post-treatment improvements on the MAL and WMFT in the Tele-AutoCITE group were not inferior to those shown by the CIMT group (Fig. 1). The mean, covariate-adjusted, post-treatment MAL score in the Tele-AutoCITE group was 3.7 points, 95% CI = 3.1—4.2; the corresponding value in the CIMT group was the same: 3.7, 95% CI =3.2—4.2. The lower-bound of the 95% CI around the difference in these scores was less than a MCID from 0: mean difference score = 0, 95% CI = –0.8—0.7; MCID = 1. The mean, covariate-adjusted, post-treatment WMFT score in the Tele-AutoCITE group was 34 repetitions per minute, 95% CI = 30—38; the corresponding value in the CIMT group was very similar: 33, 95% CI = 29—37. The lower-bound of the 95% CI around the difference in these scores was less than a MCID from 0: mean difference score = 1, 95% CI = –5—6; MCID = 10. Table 3 presents the results for the sensitivity analyses in addition to the primary analysis. For the MAL, the result of the AVG analysis was similar to that for the primary analysis, but the BOCF analysis did permit ruling out chance as responsible for the identical mean improvements in the two groups. Although there was no difference in post-treatment MAL scores between the groups on average, the lower bound of the CI around the mean (–1.1) fell just below the lower bound of the margin of non-inferiority (–1). Entering post-treatment MAL values that reflected no improvement from baseline for the two dropouts in each group (Fig. 2), as required by the BOCF analysis, resulted in an increase in variability and hence wider CI values. For the WMFT, the results of the sensitivity analyses were very similar to those for the primary analysis.
Satisfaction with and perceived difficulty of the intervention at post-treatment in the Tele-AutoCITE group were also not inferior to that reported in the CIMT group. The mean, post-treatment, POS Satisfaction score in the Tele-AutoCITE group was 6.7 points, 95% CI = 6.3—7.1; the corresponding value in the CIMT group was 6.4, 95% CI = 5.8—7.0. The lower-bound of the 95% CI around the difference in these scores did fall further than a MCID from 0: mean difference score = 0.3, 95% CI = –0.4—1.0; MCID = 1.8. The mean, post-treatment, POS Difficulty score in the Tele-AutoCITE group was 3.3 points, 95% CI = 2.3—4.4; the corresponding value in the CIMT group was 4.0, 95% CI = 3.0—5.0. The upper-bound of the 95% CI around the difference in these scores was less than a MCID from 0: mean difference score = –0.7, 95% CI = –2.1—0.7; MCID = 1.1. (The upper bound of the CI is the relevant consideration here because for the Difficulty score a between-group difference with a positive value indicates that participants who received TeleAutoCITE group found their intervention to be more difficult than those who received CIMT.) The sensitivity analyses produced results that were very similar to those for the primary analysis (see Table 3).
After 1 year, the mean improvement from pre-treatment on the MAL in the Tele-AutoCITE group was very similar to that in the CIMT group but chance could not be ruled out as responsible this outcome (Fig. 1). The mean, covariate-adjusted, long-term follow-up MAL score in the Tele-AutoCITE group was 3.0 points, 95% CI = 2.2—3.8; the corresponding value in the CIMT group was similar: 3.1, 95% CI = 2.3—3.9. However, the lower bound of the CI around the mean difference between the two groups (–1.3) fell below the lower bound of the margin of non-inferiority (–1). The results of the BOCF analysis paralleled those of the primary analysis (see Table 3). The AVG analysis results, however, permitted ruling out of inferiority: the lower bound of the CI around the mean difference between the two groups (–0.7) fell inside the margin of non-inferiority (–1). Because missing values at long-term follow-up were replaced for the AVG analysis with values that assumed the same improvement from pre-treatment that participants without missing data showed, variability of the post-treatment scores fell at the same time that the sample size increased, resulting in a narrowing of the confidence interval.
Discussion
For stroke survivors with chronic, mild to moderate, upper extremity hemiparesis, in-home delivery of CIMT with remote supervision yielded results immediately after treatment that were as good as those from in-lab, face-to-face delivery. Regardless of delivery method, participants showed very large improvements in everyday use of the more affected arm and large improvements in motor capacity of that arm. In addition, all participants reported high satisfaction with the intervention that they received and considered completing the intervention of just moderate difficulty. One year after treatment, mean improvements in everyday use of the more affected arm were similar in the telehealth and in-lab groups. However, reductions in the precision of the estimates of this parameter due to drop-out in each group over follow-up did not permit ruling out that the similar long-term outcomes in the two groups were due to chance.
These findings indicate that Tele-AutoCITE has promise as a method for overcoming several barriers to widespread dissemination of CIMT, namely, the need to travel to a clinic on multiple occasions, the concentration in urban centers of clinics with personnel with appropriate expertise, and cost. Tele-health delivery eliminates the need to travel to a clinic and permits therapists with specialty training in urban centers to treat patients in rural areas. Although the trainers in both arms of this study spent the same amount of time supervising treatment, a previous RCT using the first edition of Tele-AutoCITE showed that outcomes were not adversely affected by reducing therapist effort by 75%, i.e., by providing 8.75 instead of 35 hours of therapist support. Since labor is the largest part of the cost of providing CIMT, a reduction in therapist effort of this magnitude would result in significant savings. As noted, widespread dissemination of CIMT is of interest because it has robust evidence of efficacy and chronic, upper-extremity hemiparesis is a common problem after stroke. Even if the real-world gains after Tele-AutoCITE are modestly smaller than for CIMT, the increase in access to the intervention and reduction in cost of delivery make Tele-AutoCITE worthwhile considering as a treatment option.
An advantage of Tele-AutoCITE over alternate methods of delivering CIMT in the home is the magnitude of the improvement it produces in everyday use of the more-affected arm: mean pre- to post-treatment MAL change = 2.5, 90% CI = 2.0–2.9, d′ = 3.1. In a well-known study, Barzel and colleagues (2015) tested an in-home version of CIMT (HOMECIMT), in which a therapist, over 5 one-hour home visits, trains and supervises the patient to self-administer CIMT with the assistance of a family caregiver. Although less expensive than Tele-AutoCITE, MAL gains after HOMECIMT are much smaller (mean change = 0.6, 95% CI = 0.4–0.7, d′ = 0.8, n = 85) (Barzel et al., 2015). Gauthier and colleagues (2017) recently completed a large RCT testing an in-home, virtual-reality, gaming-based form of CIMT (Recovery Rapids; Games That Move You, PBC, Columbus, OH) that makes use of off-the-shelf hardware and has custom-built software that dynamically tailors the difficulty of training tasks to match patient needs. This approach, which eliminates the need for custom-built task stations and a table and requires less therapist effort, is also less costly than Tele-AutoCITE (Gauthier et al., 2017). However, data from a preliminary study suggest that MAL gains after this in-home form of CIMT may be smaller: mean change = 0.7, 95% CI = 0.4–1.1, d′ = 1.1, n = 16 (Borstad et al., 2018). The data from the RCT have yet to be published.
Available data do not permit conclusions about the factors that are responsible for the differences in outcome among Tele-AutoCITE, HOMECIMT, and Recovery Rapids. Three candidates are (a) implementation of task training, (b) amount of supervision provided by the therapist, and (c) implementation of the Transfer Package. Task training is implemented using task stations in Tele-AutoCITE, whereas household objects are used in HOMECIMT and virtual tasks are used in Recovery Rapids. The amount of therapist supervision is much higher in Tele-AutoCITE, as implemented in this study (35 hours), than in HOMECIMT or Recovery Rapids, as implemented in the preliminary study (5 hours). One advantage of this is allocation of a substantial amount of time to the Transfer Package, which has the critical function of promoting transfer of therapeutic gains from the treatment setting to everyday life. The Recovery Rapids RCT features an arm in which participants receive additional therapist contact with a focus on the Transfer Package, which will provide a direct test of whether doing so enhances everyday arm use in the context of an in-home, tele-health intervention.
Tele-AutoCITE departs from other tele-health approaches to outpatient rehabilitation of upper-extremity hemiparesis after stroke in three major ways. First, Tele-AutoCITE automates remote delivery of a therapy, i.e., CIMT, with robust evidence of efficacy (Hatem et al., 2016) and a basis in basic research in behavioral neuroscience and behavioral psychology (Taub, Uswatte, & Elbert, 2002). Apart from Recovery Rapids, which also is a translation of CIMT, no other form of upper-extremity tele-rehabilitation translates an intervention with similarly robust support (Sarfo, Ulasavets, Opare-Sem, & Ovbiagele, 2018). Evidence of efficacy for the original intervention is important because it makes very likely that successful translation of an in-clinic intervention will result in meaningful benefit for patients. Basic research is important because it identifies key therapy components and principles, and can therefore help guide translation of an in-clinic intervention to a remote format. Second, as noted, Tele-AutoCITE produces a very large improvement in everyday use of the more-affected arm. None of the upper-extremity tele-rehabilitation studies in adults after stroke in a systematic review by Sarfo, Ulasavets, Opare-Sem, and Obviagele (2018) assessed everyday more-affected arm function except one, which reported no change in this domain (Piron et al., 2009). A recent, large, multi-site RCT (N = 124), which was not part of this review, found that the tele-rehabilitation intervention it evaluated produced reductions in motor impairment that were equivalent to the comparison, in-clinic intervention. (Cramer et al., 2019). However, the changes in everyday more-affected arm function in the tele-rehabilitation group were inferior to those in the comparison, in-clinic intervention. (Gains in more-affected arm motor capacity in the tele-rehabilitation groups in two studies (Benvenuti et al., 2014; Wolf et al., 2015) that used the WMFT in the systematic review by Sarfo and colleagues were similar in size to those observed in the Tele-AutoCITE group here.) Third, Tele-AutoCITE implements task training using physical devices with built-in sensors that monitor patient interaction with the devices, which permits immediate, quantitative feedback on performance to be provided to the patient. Another noteworthy feature of the Tele-AutoCITE task stations is that they simulate everyday tasks, e.g., rotating a door lever (Turning Handle), turning over Dominoes (Flipping Blocks), and typing (Tapping Fingers). Other forms of upper-extremity tele-rehabilitation for adults with stroke typically use virtual tasks (e.g., Piron et al, 2009, Cramer et al., 2019) or a home kit with exercise equipment (e.g., resistive tubing, rubber handball, and putty; Cramer et al., 2019). Current evidence suggests that using actual tasks does not result in better motor outcomes than using virtual tasks (Karamians, Proffitt, Kline, & Gauthier, 2020). However, extant evidence indicates that motor training on everyday tasks or tasks that simulate them (Hubbard, Parsons, Neilson, & Carey, 2009) and with performance feedback (Subramanian, Massie, Malcolm, & Levin, 2010) produces better motor outcomes than motor training without these characteristics.
Study limitations
An important limitation of the study design is the small sample size (COMPLETERS, N = 20), which raises concerns about the precision of the effect size estimates. These concerns are reduced by the consistency of the findings from this study with previous trials from our laboratory, all of which found very large improvements after treatment on the primary outcome, i.e., the MAL, which assesses use of the more-affected arm outside of the treatment setting. The pre- to post-treatment effect size (d′) on the MAL in the CIMT group (n = 10) in this study was 3.5. In two RCTs that featured larger sample sizes, the corresponding effect size was 3.2 (n = 20; Taub et al., 2006) and 2.3 (n = 20; Taub et al., 2013). The pre-to post-treatment effect size on the MAL in the Tele-AutoCITE group (n = 10) in the study was 3.1. In two trials of the first edition of Tele-AutoCITE, the corresponding effect size was 3.7 (n = 27; Taub et al., 2005) and 3.0 (n = 7; Lum et al., 2006). Notably, in the last study, which simulated delivery on a tele-health basis, the effect size observed was very similar to that here (3.0 vs. 3.1). Gains on the MAL after CIMT were smaller in the HOMECIMT trial (d′ = 0.8), as noted, and EXCITE trial (d′ = 1.4)(Wolf et al., 2008) than here (d′ = 3.5). Likely sources of the difference in outcome between the HOMECIMT trial and this study were discussed above. In the EXCITE trial, two important components of the Transfer Package, which our laboratory has shown is key for maximizing gains in everyday arm use, were missing; homework was not assigned during treatment and participants were not systematically queried about use of the more-affected arm at home since the last treatment session at the outset of each treatment day. The latter procedure serves as an occasion to reinforce use of that arm with verbal praise and to conduct problem solving about actual and perceived barriers to use that arm.
Another limitation with respect to the sample is the modest range of motor and cognitive impairment, age, and technological knowhow present. Participants with greater than moderate motor or cognitive impairment and without adequate technological knowhow to independently operate the Tele-AutoCITE workstation were excluded. Although there was no upper limit with respect to the inclusion criterion for age, the recruitment and screening procedures in total resulted in a sample that was relatively young (median age = 60, interquartile range = 51–65, range = 32–94). These factors limit the generalizability of our findings.
Two limitations with regard to data collection are the missing observations on the MAL and WMFT at one-year follow-up and the lack of kinematic measures. Six MAL scores are missing because the participants could not be contacted. As a result, the estimate of long-term outcome is less precise than otherwise. However, the mean reduction in MAL scores from post-treatment to long-term follow-up present here (15%) is similar to that from comparable CIMT studies from our laboratory (sample-size weighted mean = 11%, range = 0 to 23%, N = 64; Taub et al., 1993, 2005, 2006, 2013). Eleven WMFT scores are missing because the participants in question were not able travel to the laboratory for testing at one-year follow-up. This number of missing observations preclude reliable reporting of long-term WMFT results. As a consequence, no objective, one-year follow-up data are present. Future studies might consider including a test of motor capacity that could be administered reliably in the home to avoid this shortcoming. Collection of kinematic data would permit examination of whether the changes in everyday arm use in this report are supported by restoration of normal movements, evolution of alternate movement of patterns, or some combination thereof.
Three limitations of the design of the Tele-AutoCITE workstation were the requirement of a Hi-speed Internet connection in the home of the participant, the need for a technician to visit the home of the participant to set up and tear down the workstation, and the size of the workstation. The requirement for a Hi-speed Internet connection to be present for remote supervision to take place excludes patients who live in areas where Hi-speed Internet is not available, such as poor rural communities, and patients who cannot afford Hi-speed Internet service. The need for technician visits raises the cost of providing treatment. The size of the workstation makes its transport somewhat cumbersome and expensive and requires that a patient has adequate room in their house to place the workstation. These design flaws, which limit the viability of the current workstation design for widespread use by clinical facilities, can be addressed by designing a workstation that (a) relies on cellular access, which is widely available, for remote supervision; (b) has a plug-and-play design, which eliminates the need for technician visits, and (c) features task stations that can be placed on a regular table or desk and be connected via a hub to the USB port of a personal computer, laptop, or tablet. Such a design would reduce the cost of production, shorten the set-up time, and take advantage of devices that many patients already have in their home. An alternate approach that has similar advantages is the use of virtual tasks, such as done in the Recovery Rapids system.
An ostensible limitation of the Tele-AutoCITE design is the small number of training tasks (10) relative to the number of training tasks from which a selection can be made when CIMT is conducted face-to-face (> 120). Surprisingly, this large difference does not appear to affect the benefit that patients can obtain from Tele-AutoCITE. As noted, participants in this study, as well as in previous studies testing the first edition of Tele-AutoCITE, had outcomes similar to those obtained by participants in the in-lab CIMT arm of this trial and previous in-lab CIMT trials. This finding suggests that when a sufficiently diverse array of tasks is present to address the types of upper-extremity impairment commonly prevalent after stroke, a large bank from which to make a selection is not necessary for obtaining optimal treatment outcomes.
Conclusions
Notwithstanding these concerns, the results suggest that Tele-AutoCITE can produce immediate therapeutic benefits in adults with chronic, mild to moderate, upper extremity hemiparesis that are not worse than those for in-lab CIMT. After suitable modifications to the design of the Tele-AutoCITE workstation to broaden the socioeconomic status of patients who can accommodate the device in their homes and reduce its cost, these promising results warrant verification by a large RCT.
Footnotes
Acknowledgments
Presented in part to the Annual International Meeting and Exposition of the American Telemedicine Association, April 2009, Las Vegas, NV and Annual Meeting of the American Congress of Rehabilitation Medicine, November 2013, Orlando, FL. There are no conflicts of interest to declare. Supported by the National Institute of Child Health and Human Development of the National Institutes of Health, Bethesda, MD under award number R01HD053750.