
Abstract
Background/Objective:
Peripheral-nerve blocks (PNBs) using continuous-infusion of local anesthetics are used to provide perioperative analgesia. Yet little research exists to characterize the histopathological effects of continuous long-duration PNBs. Herein we test the hypothesis that continuous peri-neural bupivacaine infusion (3-day vs. 7-day infusion) contributes to histologic injury in a duration-dependent manner using an in vivo model of rat sciatic nerves.
Methods:
We placed indwelling catheters in 22 rats for infusion with low-dose (0.5mg/kg/hr) bupivacaine or normal saline proximal to the right sciatic nerves for 3 or 7 consecutive days. Hind-limb analgesia was measured using Von-Frey nociceptive testing. At infusion end, rats were sacrificed, bilateral nerves were sectioned and stained with hematoxylin and eosin and CD68 for evaluation of inflammatory response, and eriochrome to assess damage to myelin.
Results:
Animals receiving continuous infusion of bupivacaine maintained analgesia as demonstrated by significant decrease (50% on average) in nociceptive response in bupivacaine-infused limbs across time points. Both 7-day saline and bupivacaine-infused sciatic nerves showed significantly-increased inflammation by H&E staining compared to untreated native nerve controls (P = 0.0001, P < 0.0001). Extent of inflammation did not vary significantly based on infusate (7-day saline vs. 7-day bupivacaine P > 0.99) or duration (3-day bupivacaine vs 7-day bupivacaine P > 0.99). No significant change in sciatic nerve myelin was found in bupivacaine-infused animals compared to saline-infused controls, regardless of duration.
Conclusions:
Long-duration (7-day) bupivacaine infusion provided durable post-operative analgesia, yet contributed to equivalent neural inflammation as short duration (3-day) infusion of bupivacaine or saline with no evidence of demyelination.
Introduction
Peri-neural injection of local anesthetic to create a peripheral nerve block (PNB) has been long-used to control post-operative pain and improve patient outcomes Capdevila, 2009; Chelly, 2010). Using implanted catheters and continuous infusion pumps to administer local anesthetics over time can create long-duration PNBs that provide analgesia for multiple days following a surgical procedure. Long-duration PNBs maintain therapeutic range, providing a steady state of pain control that cannot be achieved with oral medications (Richman, 2006; Simic, 2018; White, 2003). PNBs have been shown to increase the speed of healing (Capdevila, 2009; Uslu, 2016), and improve long-term functional outcomes in patients (Capdevila, 1999; Capdevila, 2009; Chelly, 2010; Chelly, Greger, Al Samsam,, 2001; Chelly, Greger, Gebhard, 2001; Simic, 2018), while reducing the need for opioids and the frequency of drug-dependence (Klein, 2000; Richman, 2006; White, 2003)
Currently, the Food and Drug Administration (FDA) limits the use of PNBs for a maximum of three days due to the risk of indwelling catheter-associated infection (Capdevila, 2009) and the potential adverse effects of local anesthetic on myelin. However, these investigations have studied either non-standard doses of anesthetic or non-standard techniques, including intra-neural injection with high injection pressure (Brull, 2007; Kalichman, 1989; Kapur, 2007; Yang, 2011). Local anesthetics are associated with neurological toxicity in a dose dependent manner, however the effect of PNB duration is not well studied (Hogan, 2008; Ilfeld, 2017; Ilfeld, 2010; Jeng, 2010; Memari, 2016; Verlinde, 2016). The mechanism of local anesthetic-induced neurological toxicity may be linked to superoxidation and peroxidation (Yu, 2017). Previous laboratory models have indicated that injection of local anesthetics to create PNBs may lead to histological changes such as inflammatory infiltration, Schwann cell death and demyelination (Kalichman, 1989; Kapur, 2007; Voelckel, 2005; Yang, 2011). However, clinical reports of neurological complications following PNB are uncommon (∼3%) and generally resolve in days to weeks with no permanent damage (Ben-David, 2006; Brull, 2007; Candido, 2005; Hogan, 2008; Simic, 2018). Often these complications occur following bolus injection of local anesthesia or are associated with pre-existing pathology such as nerve trauma (Byram, 2020), diabetic neuropathy (Jeng, 2010; Markova, 2020) or advancing age (Yee, 1997). Literature supporting the efficacy and risks of long-duration continuous infusions of local anesthetics to create PNB greater than 3-days is scarce, and due to the morbidity associated with nerve biopsy, clinical studies do not include analysis of the treated nerve at histopathological level (Ilfeld, 2017; LeBlanc, 2005; Simic, 2018). Therefore, investigation of the histopathological effects of long-duration PNBs in preclinical models are needed to fully understand their impact on peripheral nerves, and support their use in practice for safe and effective pain control. Our study aims to fill the current gap in the literature pertaining to the extent of demyelination and inflammation associated with long-term infusion of low-dose bupivacaine.
To better understand the effect long-duration PNBs have on peripheral nerve structure and function, we examined the effects of continuous bupivacaine infusion on rat sciatic nerves, and compared 7-day bupivacaine infusion to the standard 3-day treatment. Additionally, animals in a sham surgery group receiving saline infusion were used to control for the physical effects of catheter placement served as a direct comparison for nociceptive response following surgery and histological changes in the sciatic nerve. We found that 7-day infusion of bupivacaine produced durable analgesia for the duration of treatment. Histological analysis indicated that 7-day bupivacaine infusion caused moderate inflammation that was not significantly different than 3-day bupivacaine infused (P = 0.72) or saline infused sham control animals (P = 0.37). Surprisingly, no appreciable damage to myelin was found in the sciatic nerves of 3-day or 7-day bupivacaine infused animals at 0.5 mg/kg/hr.
Methods
Animal surgery
Twenty-four healthy Sprague Dawley male rats (200–350 g) were anesthetized with isoflurane using a snout mask prior to catheter placement in the right hind limb (Fig. 1). Temperature was monitored using a rectal probe, and pre-operative administration of the NSAID Rimadyl (5 mg/kg) was used to provide additional analgesia. Surgical site was shaved and prepped by scrubbing two times with an iodine solution. Incision was made over the right posterior-lateral aspect of the thigh to gain visualization of the sciatic nerve trifurcation. A catheter (Polyethylene 50 tubing, Fischer Scientific, Waltham, Massachusetts, USA) was inserted with catheter-tip placed inferior to sciatic nerve then sutured in place to the semimembranosus muscle 5mm proximal to the sciatic trifurcation. The remaining catheter was tunneled subcutaneously to the base of the neck, where it was exteriorized. The catheter was attached to a harness with a swivel adapter at the base of the neck that was secured over the forearms and around the chest using rubber tubing and two 3.0 sutures (Fig. 1). This served as a secure connection point between the indwelling catheter and the syringe pump, and allowed the rats to have freedom of movement within their enclosures. The catheter patency was visually tested prior to closing the incision. The incision site was then closed using a combination of 4.0 sutures and Vetbond (3M Vetbond Tissue Adhesive 1469, 3M Center, St. Paul, MN, USA). Using a test animal positioning and stability of catheter placement was validated by continuously infusing a 1% methylene blue dye dissolved in 0.9% normal saline for 3 days prior to sacrifice, when sciatic nerve staining was assessed during necropsy. To identify any change in catheter position a mark was place on the catheter at the skin interface where it was exteriorized, and monitored for movement daily. Catheter positioning was verified on all animals at time of sacrifice on Day-3 or Day-7. One animal from the 7-day saline group was found to have a loss of correct catheter positioning and was removed from the study, another animal from the 7-day bupivacaine group was sacrificed due to failure to recover following surgery, thus the study was completed with twenty-two animals.

Graphical workflow: To determine if long-duration low-dose peri-neural bupivacaine infusion causes histopathologic damage to rat sciatic nerves A) Tunneling catheters were surgically placed over the right sciatic nerve of isofluorane anesthetized rats using an open approach. B) Rats were fitted with a harness and connected to a syringe pump for infusion. C) Animals were divided into two cohorts receiving either 0.5 mg/kg/hr bupivacaine or a sham group receiving normal saline for 3-days or 7-days. D) Hind limb analgesia was monitored using the Von-Frey filament analysis. E) At the time of sacrifice (end of Day-3 or Day-7) animals were perfused and both the catheterized right (treated) and native left (untreated) sciatic nerves were section for H&E, CD68 and myelin staining and analyzed to assess for signs of inflammation and demyelination.
Animals were infused with 0.9% normal saline (sham) or 0.5% bupivacaine solution (treated) as shown in Table 1. The bupivacaine dosage administered was 0.5 mg/kg/hr using the respective animal body weights measured at the time of surgery. Dose infusion was maintained by a syringe pump (Harvard Apparatus, Elite 11, model # 70-4501, Holliston, MA), and visually inspected daily for proper delivery.
Rat Infusion Duration and Treatment
Rat Infusion Duration and Treatment
Analgesia was measured using the Von-Frey filament method. Both the left and right hind paws were tested on day 1, day 3 and day 7. Both testing and recording of animal response was done by a blinded evaluator. Prior to data collection, rats were acclimatized to an acrylic box with a wire-mesh bottom for 10 minutes. The Von Frey monofilaments (monofilament, Stoelting Co., USA) were applied to the plantar surface of hind paw. Both the untreated native left hind limb and catheterized (treated) right hind limb were tested in each animals beginning with right limbs. The minimum weight of the monofilament able to elicit a response five out of 10 times (50% threshold) in each individual limb was recorded. One minute was given between applications of Von Frey filaments. The filaments were used in an up-down fashion, recording the minimum weighted filament able to elicit a response 5 out 10 times to determine 50% threshold value. In order to normalize responses across animals, a fractional value of nociception was determined for each animal by dividing the minimum weighted filament that elicited a 50% response for the untreated left limb by the minimum weighted filament that elicited a 50% response for the catheterized right limb. This created a single value that could be compared across animals and time points, and controlled for any baseline variation in nociception between individual animals and individual differences due to the systemic stress of undergoing surgical catheterization.
Histological sample preparation and staining
For histologic and immunohistochemical analysis, animals were anesthetized under 5% isoflourane and then intracardially perfused under deep sedation using 4% buffered paraformaldehyde in 0.1 M phosphate buffer. The catheter tip position was recorded at the time of sacrifice and compared to the internal position at time of placement. Left and right sciatic nerves were then dissected out and processed for paraffin embedding with careful attention of sampling nerve regions directly adjacent to the catheter tip. Sections of the nerves were cut on a microtome at a thickness of 6μm sections and stained with eriochrome to assess myelin integrity and CD68 to evaluate monocytic/macrophage infiltration and activation. Sample preparation and staining was performed as described in Yang et al., 2011. Additionally, nerves sections were stained with hematoxylin and eosin (H&E) to screen for other structural or inflammatory changes as described in Cardiff et al., 2014.
Histological analysis
Analysis was conducted using an Olympus BX50 microscope equipped with a Leica DFC295 camera and Leica Application Suite version 4.4 software for image capture. Sections were coded with random numbers and analysis of histological sections was conducted by a board certified neuropathologist unaware of both treatment group and animal identity. H&E stained slides were specifically assessed for peri-neural inflammation, neovascularization, and collagen deposition. CD68 stained slides were analyzed for peri-neural or intra-neural infiltration of macrophages. Myelin stained slides were analyzed for myelin stain loss and for the presence of myelin debris within macrophages. The semi-quantitative grading scales were developed with the goal of utilizing the entire scoring range, and individual slides were ranked from 0–3. Nerve sections without any abnormal findings were scored as 0. A score of 1 included rare macrophages, scant demyelination or minor inflammatory changes. While a score of 3 contained the maximal amount of macrophages, demyelination or inflammation in the entire slide set. Nerve sections that contained an intermediate level of abnormal pathology were scored as 2. Representative images were captured to represent each condition. For each nerve and condition the entirety of 2-3 sections ∼100 um apart were analyzed on the microscope from each nerve, the scores were then compared across conditions.
Statistics
All statistical analyses were done using the GraphPad Prism software v7.0d on Macintosh using guidelines for histopathologic scoring described in Gibson-Corley et al., 2013. Von-Frey filament test scores were compared to their respective controls and analyzed for statistical significance using the Mann-Whitney 2-tailed t-test. H&E, CD68, and Myelin scores were compared to their respective left-limb controls and analyzed for statistical significance using one-way ANOVA with Kruscal-Wallis correction and Mann-Whitney 2-tailed t-test for individual comparisons.
Ethics
All rat studies were approved by IACUC and conducted in accordance with oversight from the OHSU Department of Comparative Medicine’s veterinary team.
Results
Catheter placement
To first demonstrate accuracy of catheter placement and peri-neural delivery of infusate over time, a catheter was placed in a preliminary test animal, and infused with methylene blue dye for 3 days. At the time of post-infusion necropsy, the methylene blue dye stained a localized area of the sciatic nerve and surrounding connective tissue, indicating that the catheter tip was properly positioned and remained in place for the duration of the infusion (data not shown). Catheter placement was verified externally using the reference mark on the catheter on a daily basis and internal placement was verified at time of sacrifice. All animals had consistent catheter tip position between placement and sacrifice, with the exception of one animal which was excluded from the study at the time of sacrifice.
Behavior and response
To validate the analgesia provided by treatment conditions, Von-Frey filament testing was used to quantify animal response to graded tactile stimulus (Bradman, 2015). Animals receiving bupivacaine displayed decremented nociceptive response to tactile stimulus in their catheterized right limbs as compared to saline infused sham animals (Fig. 2). A statistically significant difference was found between the saline control sham animals and bupivacaine infused animals in day 1 (P < 0.01) and day 3 (P = 0.05). On day 7 the efficacy of bupivacaine analgesia did not reach statistical significance (P = 0.07) due to a large variation in the 7-day saline control group. However, the diminished nociceptive response to tactile stimulus of the right limb in the bupivacaine treated animals remained consistent throughout all three time points, at roughly 50% that of the native left limb in each animal. This finding indicated that a durable analgesic effect was maintained for the duration of the study.
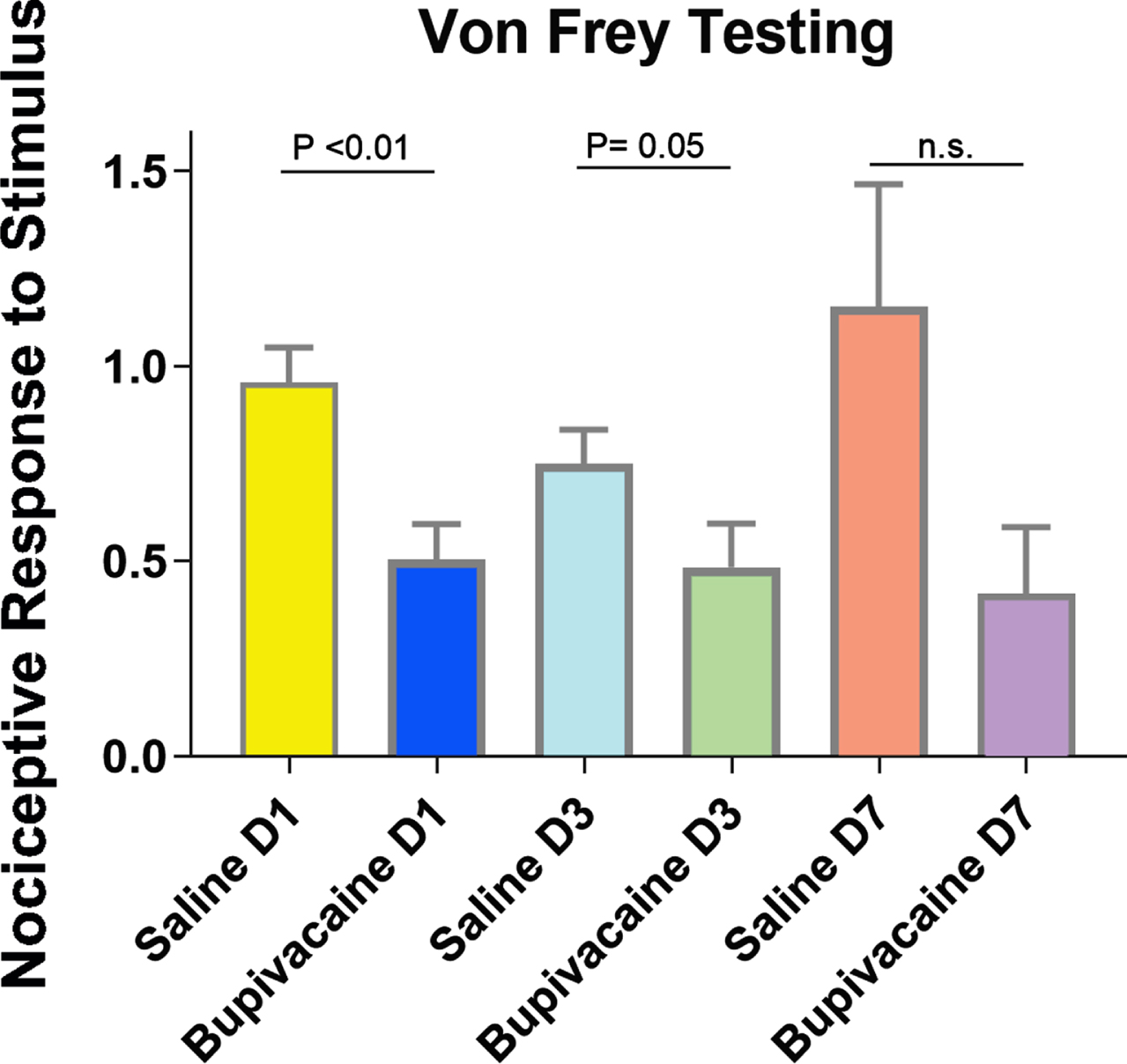
Results of Von Frey filament testing indicating analgesic effect in bupivacaine infused animals compared to saline infused sham animals. Graphically depicted as fractional value of nociceptive response to weighted filaments in catheterized right limb (treated) normalized to responses elicited in native left limbs for each individual animal. Nociceptive responses in animal groups exposed to saline (sham) or bupivacaine were compared on Day-1 (P < 0.01), Day-3 (P = 0.05), Day-7 (P = 0.07) (Mann-Whitney, 2-tailed Test). All columns indicate mean and standard error of measurement. Saline D1 n = 11, Bupivacaine D1 n = 10, Saline D3 n = 11, Bupivacaine D3 n = 10, Saline D7 n = 5, Bupivacaine D7 n = 5
To assess for histologic damage following infusion of bupivacaine or saline, we sectioned both the catheterized right and native left sciatic nerves from each animal and performed hematoxylin and eosin (H&E) staining. Nerve sections were analyzed for peri-neural inflammatory and structural changes such as neovascularization, increased collagen deposition and inflammatory cell infiltration. Comparison between the catheterized right and native left sciatic nerve served as an internal control and revealed a significant increase in inflammation in right nerves across all treatment conditions regardless of infusate or duration (Fig. 3A/a) (left vs 7-day saline P = 0.0001 and left vs 7-day bupivacaine P < 0.0001). The level of inflammation caused by saline or bupivacaine was not significantly different (7-day saline vs. 7-day bupivacaine P > 0.99) and was not duration-dependent (3-day bupivacaine vs 7-day bupivacaine P > 0.99).
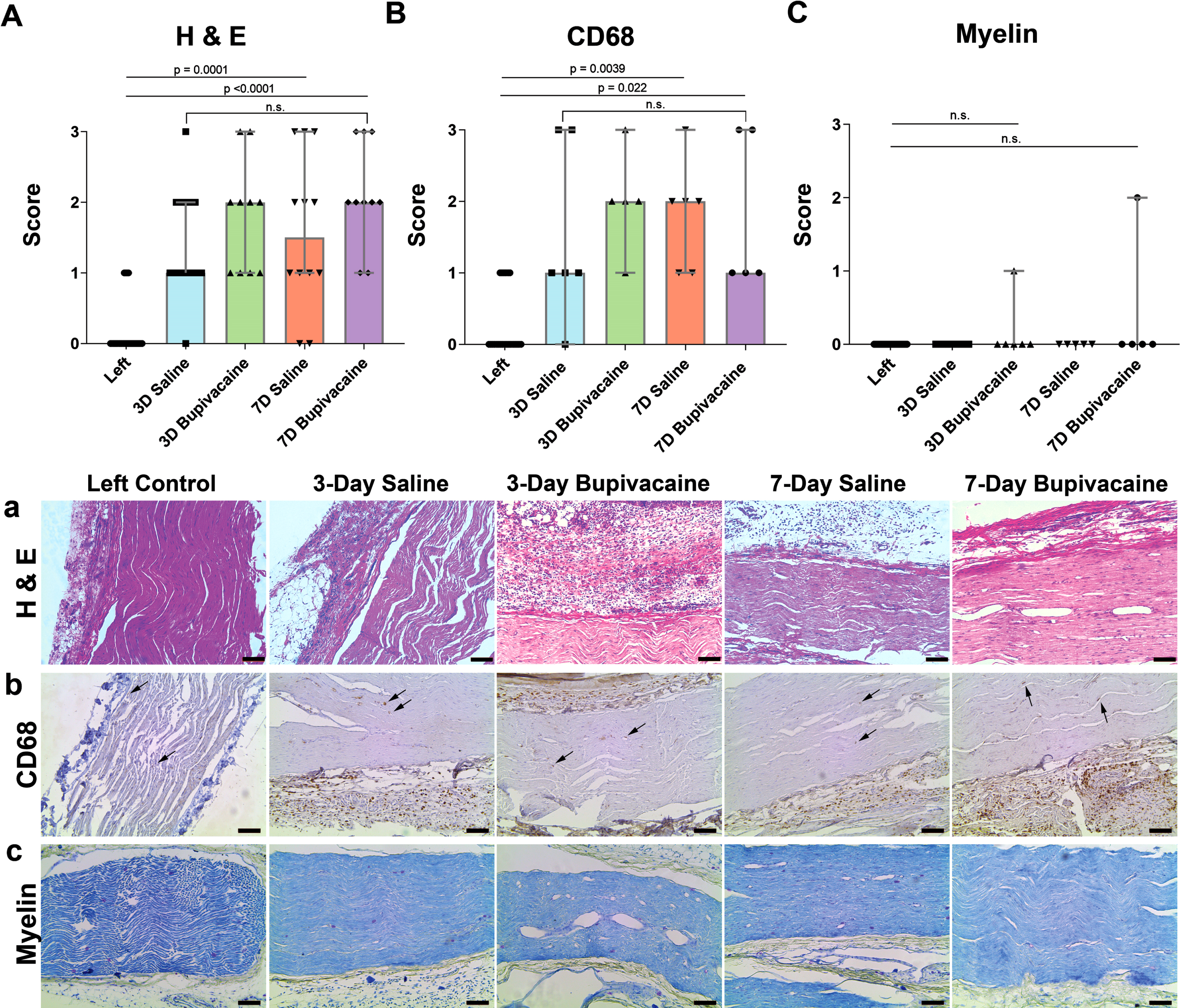
A) Results of H&E staining analysis showing increased inflammation in both saline and bupivacaine treated right sciatic nerves compared to left untreated controls in both 3-day and 7-day cohorts. Inflammation was similarly significant across treatment conditions when compared to left control nerves (ANOVA) regardless of infusate or duration (7-day saline P = 0.0001 and 7-day bupivacaine P < 0.0001). The level of inflammation caused by saline or bupivacaine was not significantly different (7-day saline vs. 7-day bupivacaine P > 0.99; Mann-Whitney 2-tailed Test) and was not duration-dependent (3-day bupivacaine vs 7-day bupivacaine P > 0.99). a) Representative images of nerve sections stained with H&E. B) Macrophage infiltration increased significantly in both saline and bupivacaine treated right sciatic nerves when compared to left untreated controls (7-day saline P = 0.0039 and 7-day bupivacaine P < 0.022; ANOVA) but did not differ significantly between treatment conditions or duration (7-day saline vs. 7-day bupivacaine P > 0.90; 3-day bupivacaine vs 7-day bupivacaine P > 0.99; Mann-Whitney 2-tailed Test). b) Representative images of nerve sections stained with CD68. Arrows indicate rare CD69 + intra-neural macrophages. C) Results of myelin staining analysis showing no significant change in myelin across conditions (3-day bupivacaine vs left control P = 0.158 and 7-day bupivacaine vs left control P = 0.135; Mann-Whitney 2-tailed Test). c) Representative images of nerve sections stained for myelin. All columns indicate median and 95% confidence interval. Significance P < 0.05. All scale bars = 100μm. Left n = 22, 3D saline n = 6, 3D bupivacaine n = 6, 7D saline n = 5, 7D Bupivacaine n = 5, with 3 replicates per condition for H&E and 2 replicates per condition for CD69 and Myelin stains.
Immunohistochemical staining for CD68 was used to measure intra-neural and peri-neural macrophage infiltration (Fig. 3B/b). Intra-neural macrophages were rare under both conditions and did not differ significantly between groups (3-day bupivacaine vs left control P = 0.158; 7-day bupivacaine vs. left control P = 0.135). When compared to native left sciatic nerves, peri-neural macrophage infiltration was significantly higher in catheterized right sciatic nerves (7-day saline P = 0.0039 and 7-day bupivacaine P < 0.022). However, the extent of peri-neural macrophage infiltration did not differ significantly between infusate groups or duration of infusion (7-day saline vs. 7-day bupivacaine P > 0.90; 3-day bupivacaine vs 7-day bupivacaine P > 0.99). Comparatively intra-neural macrophages were rare and did not differ between treatment groups.
Finally, sciatic nerve sections were stained for myelin to assess for potential demyelination and damage to Schwann cells. Little to no disruption or loss of myelin was found in the catheterized right sciatic nerves of either saline or bupivacaine treated animals in both the 3-day and 7-day cohorts (Fig. 3C/c). Myelin structure and staining density of the right sciatic nerves were not significantly different (P > 0.9999) when compared across treatment groups, or to native left sciatic nerves. Together, these results indicate that catheter placement and 7-day infusion of low-dose bupivacaine causes peri-neural inflammation similar to that of normal saline or to the current FDA recommended maximum of 3-day bupivacaine infusion. Additionally, infusion of bupivacaine for 7-days at 0.5 mg/kg/hr did not result in damage to sciatic nerve myelin.
The results of this study demonstrated that 0.5 mg/kg/hr long-duration bupivacaine infusion does not cause statistically significant nerve inflammation, as compared to saline-infused sham controls. Additionally, no significant change in myelin staining was found across conditions, indicating a total lack of myelin toxicity. The first study to explore the continuous infusion of bupivacaine in rat sciatic nerves, found that prolonged exposure caused peri-neural inflammation and infiltration and activation of macrophages within the nerve (Yang, 2011). This study used a similar catheterization procedure and a continuous infusion apparatus to deliver local anesthetic to the sciatic nerve. However, the Yang et al., study used a roughly 3-5-fold higher dosage of bupivacaine (100 ul 0.5% or 0.75%/hr versus ∼35 ul 0.5%/hr). This difference in dose likely resulted in higher toxicity and myelin damage, not seen during our study. To determine if lower dosages typically used in the clinical setting for continuous PNBs also confer anesthetic related toxicity on peripheral nerves and Schwann cells, we repeat the study to identify pathological changes at the sciatic nerve in response to extended long-duration PNB. For this study we used a bupivacaine concentration and rate that was slightly higher (0.5 mg/kg/hr) than FDA approved continuous infusion rates for children (0.2mg–0.4 mg/kg/hr) that have been previously validated in clinical studies to provide efficacy in post-operative pain control (Dadure, 2009; Simic, 2018). Further, conducting this investigation in preclinical models is the only method that allows ethical analysis of treated nerve on a histological level.
Local anesthetics such as bupivacaine have been shown to cause neuron and Schwann cell death in a time (Yang, 2011) and concentration (Yu, 2017) dependent manner. In this study we used a bupivacaine dose of 0.5 mg/kg/hr (35 ul 0.5%/hr), which provided durable analgesia to the animals for the 7-day duration of PNB as indicated by the sustained ∼50% decrease in nociceptive response measured via Von-Frey testing (Fig. 2). At this concentration and duration there was no appreciable damage to nerve myelin, or increase in inflammatory response greater than that observed in the saline infused sham group or 3-day bupivacaine infused animals representing the FDA standard limit of duration (Fig. 3).
To assess for analgesic effect of continuous bupivacaine infusion we relied on the Von Frey method which uses weighted filaments to identify the threshold of nociceptive stimulation required to elicit a response (limb withdrawal, postural change, cleaning, muscle tension) (Bradman, 2015). This method has been long used to study allodynia, where hyperalgesia in an animal lowers the threshold of nociception causing an animal to respond to a less weighted filament. Conversely we and others have found that this method also applies for measuring analgesia, where an animal with an increased threshold of nociception requires a greater weighted filament to elicit a response than would be required in absence of analgesia (Cheong, 2020). The Von Frey method has it flaws, mainly in the inherent subjectivity of interpreting animal behavior as a surrogate for perceived sensation of pain, and the time consuming nature of data collection. However, we have found that using blinded evaluators, we are able to reliably identify animals that have received analgesia Von Frey filaments. We find that individual animals that are naïve of surgery/treatment, have slightly different thresholds of nociception and/or display different levels of behavioral responses to identical stimuli at baseline. Therefore, some data normalization is required to statistically compare response between individual animals and groups. We felt that comparing the response in limbs of animals who have endured a surgical procedure to those of surgery-naïve animals would be confounded by the systemic stress of undergoing surgery. Therefore, we chose not to compare thresholds pre and post-surgery in individual animals. Instead we used the native left limb as an individual comparison, and divided the filament weight required to elicit a response in the catheterized right limb by the filament weight required to elicit a response in the native left limb in each individual animal during all post-operative time-points. All animals tested were subjected to the same surgical procedure and had fluid delivered to the sciatic nerve, with the only difference being the addition of bupivacaine to the infusate and duration of infusion. This ensured that all data points were collected from animals under identical conditions, and had similarly endured the systemic stresses associated with surgically implanting a catheter. This data was then graphed as the fractional nociceptive response to demonstrate post-operative pain control.
Using this technique, we show that hind paws that received bupivacaine infusion had a decreased nociceptive response compared to native left limbs or the limbs of saline infused sham animals. Analgesia remained similar across time points, however statistical significance was lost between the treatment and control groups when comparing the 7-day animal cohorts (P = 0.07). This was first thought to be a sign of tachyphylaxis—a well described neural effect following continuous administration of local anesthetic (Choi, 1997; Lipfert, 1989; Thalhammer, 1995; Wilder, 1996), which may have contributed to a decline in analgesic effect and statistical significance. Tachyphylaxis in response to local anesthetic was demonstrated in a study that used repeat injections of lidocaine to rat sciatic nerves; following each subsequent injection a decremented duration of nerve block was observed, coinciding with an increase in drug clearance from the tissue (Choi, 1997). However, the analgesic effect in this study was maintained throughout time points, as the 7-day bupivacaine treated animals showed a similar loss of sensation as compared to 1-day and 3-day bupivacaine infused animals. The loss of significance in this case was due to variation within the 7-day saline sham cohort, which showed a larger standard error compared to the bupivacaine treated animals (Fig. 2). The increased standard error is largely the result of one animal in the 7-day saline infused sham group which showed signs of hyperalgesia following surgical catheter placement. It was surprising that allodynia was not more commonly observed in the sham saline control group that received no post-operative nerve block.
The mean reduction in nociceptive response measured in animals with bupivacaine treated limbs was relatively stable at ∼50% across all time-points, compared to native left limbs or right limbs of sham animals receiving saline infusion. In contrast to a study which measured measure limb withdrawal in response to heat and pinch following a single bolus of bupivacane, Vladimirov et al., found complete unresponsiveness of the limb at 100-minutes post-bolus. In our study the gradual administration and significantly longer time course of administration used in this study, likely allows for both tachyphylaxis, and/or increased drug clearance from surrounding tissues to diminish effect in comparison to response following a single bolus, therefore we are still able to elicit some response to higher weighted filaments in bupivacaine treated limbs (Thalhammer, 1995; Vladimirov, 2000). Furthermore, saphenous innervation extrinsic to the sciatic nerve, may contribute to some minor response to Von Frey filament testing, and is why only 50% decrease in nociception is observed in bupivacaine infused animals.
Interestingly, microscopic examination of the nerve using H&E and CD68 staining revealed perineural inflammatory infiltrates in the right sciatic nerves in both saline and bupivacaine infused animals in both 3-day and 7-day cohorts. The 7-day bupivacaine infusion did not result in significantly greater inflammation in right limbs compared to the saline infused sham animals, this demonstrates that physical placement of the catheter itself and fluid flow are contributing factors to the histological changes observed in treated nerves. Additionally, these results may indicate that physical trauma of catheterization, fluid infusion, or the introduction of foreign materials (i.e. skin flora) have greater contribution to inflammation than long-duration low-dose peri-neural infusion of bupivacaine to rat sciatic nerves over a 3–7 day period.
With any nerve block, proximity of the catheter or local anesthetic to the nerve is crucial to achieving adequate analgesia (Gorsewski, 2012). In delivering regional anesthetic, there remains an inherent risk of intra-neural penetration by a needle or catheter (Hadzic, 2004; Kirchmair, 2016; Vlassakov, 2018). Though rare in practice, physical placement of an anesthetic delivery device in relation to the nerve has been shown to cause neurological deficits (Fredrickson, 2009; Jeng, 2010; Verlinde, 2016) and traumatic nerve damage (Hadzic, 2004; Sakura, 1995). In this study, the uniformity of histological findings seen across animals—regardless of infusate or time course—further suggests that catheter placement and anesthetic delivery were consistent across animal groups and treatment conditions.
This study determined that low dose bupivacaine maintains analgesia with minimal inflammatory effect on rat sciatic nerves. Conversely, the previous study by Yang et al., 2011 found that a 3-5-fold higher dose of bupivacaine resulted in toxicity in a time and concentration dependent manner. In order to fully resolve the therapeutic window of bupivacaine infusion, further analysis is needed to find the upper limit where toxicity begins to occur. Additionally, novel local anesthetics are continuously being developed with desirable pharmacologic profiles. Our infusion model is an ideal system to test the safety and efficacy of novel anesthetics, and by incorporating the use of bupivacaine in parallel could serve as a comparative control to standardize histological findings and behavioral studies.
In conclusion, our study demonstrated the efficacy and safety of low-dose bupivacaine administration for extended durations up to 7-days. Long-duration infusion maintained analgesic effect without significant inflammation or damage to nerve myelination as compared to saline infused controls. These results indicate that continuous low-dose infusion of bupivacaine is a safe and effective option for post-operative pain control. Additional research into this topic is imperative as long-duration nerve blocks likely have the potential to reduce the use of oral opioids post-operatively.
Respective contributions
Tobias Robinson, Jeffery Kirsch and John Butler contributed to the conception and design of this study. Material preparation, data collection and analysis were performed by John Butler, Tobias Robinson and Jared Edwards. Histological preparation and analysis was provided by Marjorie Grafe and Tobias Robinson. The manuscript and figures were created by John Butler, with commentary and editing provided by other coauthors. All authors read have read and approved the manuscript.
Conflict of interest statement
John T. Butler, PhD has no conflict of interest.
Tobias J. Robinson, MD has no conflict of interest.
Jared R. Edwards, MD has no conflict of interest.
Marjorie R. Grafe, MD, PhD has no conflict of interest.
Jeffrey R. Kirsch, MD has no conflict of interest.
Funding statement
Funding was provided by the OHSU Department of Anesthesiology and Perioperative Medicine.