
Abstract
Background:
Visual field defects (VFD) usually do not show improvement beyond 12 weeks from their onset. It has been shown that repetitive presentation of a stimulus to areas of residual vision in cases of visual field defect can improve vision. The counterpart of these areas in the brain are the partially damaged brain regions at the perilesional areas where plasticity can be enhanced.
Objective:
We aimed to study the effect of navigated repetitive transcranial magnetic stimulation (rTMS) applied to perilesional areas on the recovery of patients with cortical VFD.
Methods:
Thirty-two patients with cortical VFD secondary to stroke of more than 3 months duration received 16 sessions of either active or sham high frequency navigated perilesional rTMS. Automated perimetry and visual functioning questionnaire (VFQ-25) were performed at baseline and after completion of the sessions.
Results:
The active group showed significant improvement after intervention, compared to the sham group, in both mean deviation (MD), visual field index (VFI) and in the VFQ-25 scores.
Conclusions:
Navigated rTMS is a new treatment option for post-stroke VFD as it can selectively stimulate areas of residual vision around the infarcted tissue, improving the threshold of visual stimulus detection which could be used alone or in combination with existing therapies.
Abbreviations
areas of residual vision direct current stimulation mean deviation homonymous hemianopia repetitive transcranial magnetic stimulation visual field defects visual field index visual functioning questionnaire-25 vision restoration therapy resting motor threshold.
Introduction
Visual functions are supported by various structures throughout the brain (Pambakian & Kennard, 1997). Visual field defect (VFD) is a common outcome of brain insults especially cerebrovascular strokes. Among these, homonymous hemianopia (HHA) is the most frequently encountered in clinical practice (Rowe et al., 2009). The prevalence of VFD ranges from 8.3% to 16% in the chronic stage of stroke (Townend et al., 2007), while it ranges from 7– 25% in acute and subacute stroke (Barker & Mullooly, 1997; Naeem, 2012). In a database of 11900 stroke patients, it was found in 60.5%, among whom HHA accounted for 35% (Ali et al., 2013).
VFDs usually show some recovery within a few months from onset due to resolution of edema and diaschisis, with only 5% of patients showing full recovery. However, by the 3rd to 6th month of onset, the condition tends to become stationary and further improvement is less likely (Gray et al., 1989; Zhang et al., 2006). In other studies, recovery occurred mostly in the first 10 days of injury followed by a plateau after 10– 12 weeks (And & Kolmel, 1991; Cassidy et al., 1999; Gray et al., 1989). Beyond this time point, very few cases develop spontaneous recovery (D. A. Poggel et al., 2001).
Current treatments for VFD comprise compensatory strategies and vision restoration by training (Sabel et al., 2020). Vision restoration therapy is one of the restorative therapies available for VFDs, where flashes of light are presented to the transition zone separating blind and intact visual fields to stimulate areas of residual vision (ARV) (Sabel et al., 2011). The positive effect is thought to result from reactivation of surviving perilesional networks (Jobke et al., 2009). These ARVs maintain some degree of functional capacity, which might underlie the phenomenon of blind sight where some unconscious vision exists in the blind field. These patients deny seeing objects presented in their blind field, yet their guesses to what is presented usually exceed chance. Blindsight has been ascribed to extra-striate pathways that survived injury (Sabel & Kasten, 2000). Plasticity occurs mainly in ARVs rather than areas of absolute blindness. These ARVs are the functional counterpart of partially damaged brain regions at the perilesional borders. Recovery of function, both early in life and in adults, is stimulation dependent and this stimulation can be either through visual experience, behavioral training or brain stimulation (Cavanaugh & Huxlin, 2017; Gothe et al., 2001; Sabel et al., 2011).
In the past few years, efforts were made to study the effect of different non-invasive brain stimulation techniques on the characterization and modulation of the visual information processing (Sabel et al., 2020). Visual cortex excitability using rTMS was studied using induced phosphenes analysis in blind patients with variable pre-geniculate lesions and different degrees of residual visual functions (Gothe et al., 2001). Results indicated an alteration in the TMS-induced activation of the deafferented visual cortex. It also showed reduced ability of phosphene induction in patients with higher degree of visual deafferentation especially those without previous visual experience. Among the non-invasive therapeutic possibilities, rTMS and direct current stimulation DCS were found to have a promising effect in patients with hemianopia (Sabel et al., 2020). For example, DCS combined with visual rehabilitative training can enhance recovery of visual field defects in stroke patients with the effects being stable over time (Plow et al., 2011; Plow, Obretenova, Fregni, et al., 2012; Plow, Obretenova, Jackson, et al., 2012). However, the degree of visual field restoration is still limited, prompting our search for alternative therapies.
Recently, neuro-navigated TMS has been used as a non-invasive preoperative assessment tool for patients undergoing brain tumor resection and epilepsy surgeries (Paiva et al., 2012; Säisänen et al., 2010). This technique relies on utilizing 3D MRI of the patient’s brain to create subject-specific head models. Consequently, accurate stimulation of cortical regions could be achieved in order to outline targeted functional areas in the cortex (Ruohonen & Karhu, 2010).
The hypothesis of the current study is that stimulation of the perilesional, seemingly healthy brain tissue bordering the lesioned visual cortex, would result in clinical improvement. This is based on the aforementioned concept of ARV and the fact that TMS can change the excitability of visual cortex (Gothe et al., 2001). Navigated rTMS would be the most suitable technique to achieve this precise targeting.
We aimed to study the effect of navigated repetitive transcranial magnetic stimulation (rTMS) applied to perilesional areas in patients with post-stroke cortical VFD. To our knowledge, this is the first randomized controlled trial testing the effects of perilesional rTMS on VFDs.
Methods
This is a prospective, randomized, double blind, case-controlled study conducted in the neuromodulation lab of the neurology department, Ain Shams University after approval by the local IRB. All participants gave an informed written consent.
A total of 35 patients with cortical VFD secondary to ischemic stroke were recruited for the study, yet only 32 patients completed the study (3 patients dropped out; 2 due to difficult transportation and 1 patient did not follow up after receiving the sessions).
Inclusion criteria included age more than 18 years, a duration of lesion of more than 3 months, and brain imaging showing an infarction involving visual cortical area. Patients were excluded if they had VFD or any visual disturbance of ocular origin or any contraindications for rTMS such as history of epilepsy, skull bone defects, or implanted metallic devices.
Patients were randomly assigned to either active or sham groups by sealed envelope method.
On the initial visit, medical history was taken including duration since insult and type of visual defect, followed by neurological examination with special focus on clinical visual field examination by confrontation method to verify the presence of a VFD.
Assessment
Assessment was done prior to and after 16 rTMS sessions using the National Eye Institute Visual Functioning Questionnaire-25 (VFQ-25) (developed by RAND under sponsorship of NEI) interviewer form (Mangione et al., 2001), and automated perimetry (Humphrey field analyzer 3 by Carl Ziess – Meditech for static field testing) to examine 30-degree field of vision from center of fixation using the full threshold 30-2 and obtain the mean deviation and visual field index. Reliability criteria were established as < 20% fixation losses or < 33% false negative errors or false positive errors according to the perimetry user manual (Humphrey Instruments, Inc.). Mean deviation (MD) refers to the calculated deviation from the expected visual threshold value for a person of the same age and ethnicity. Subjects who are able to see dimmer stimuli than those of similar age are given positive MD values, while subjects who need brighter stimuli are given negative MD values. MD values for reliable tests typically range from+2 dB to – 30 dB (Goñi & Maja, 2016). Visual field index (VFI) expresses the visual field status as a percent of a normal age- adjusted visual field (Goñi & Maja, 2016; Paiva et al., 2012).
Procedures
Target selection using head model
Three-dimensional magnetic resonance imaging (3D MRI); T1WI with 200 cuts of 0.9 mm sections was obtained and used to create a virtual head model for each patient using Visor 2 software (ANT-Neuro, Berlin, Germany). The head model was then segmented to separate the scalp, skull and brain layers. Targets for stimulation were determined and marked on the head model for each patient. Four targets were selected to be along the outer border of the lesion in the nearest seemingly healthy perilesional tissue (Fig. 1). At the beginning of each session, a neuro-navigation system (Visor 2, ANT-Neuro, Berlin, Germany) was used to co-register the head model to patient’s actual head, and to track coil position relative to the stimulation target on the head in real-time during the entire session.
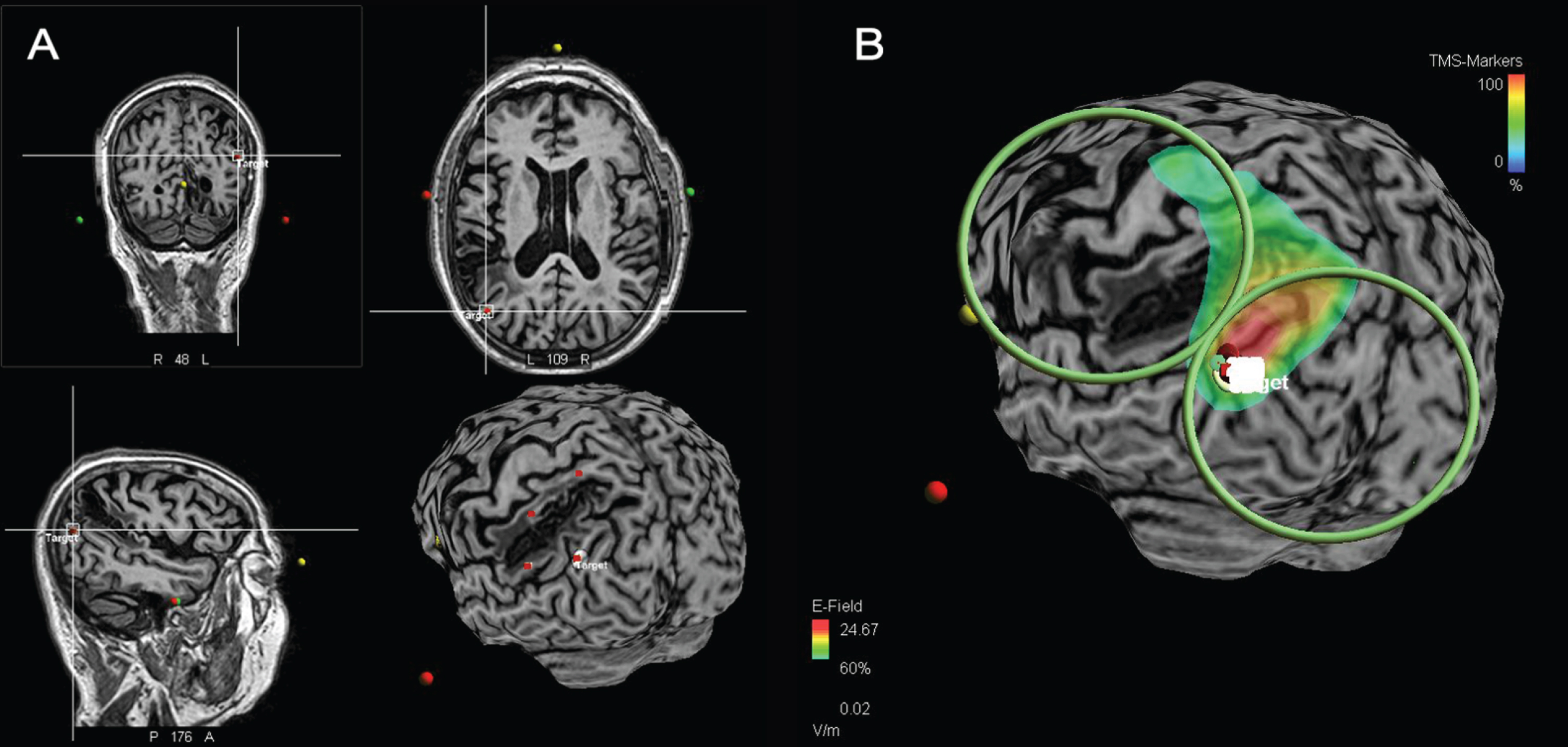
MRI brain and brain model of one patient. (A) The 4 perilesional stimulation targets (red tags; down right) (B) coil orientation and magnetic field during a TMS session.
Patients in the active group received a total of 16 rTMS sessions that were scheduled to be every other day. Each of the four predetermined perilesional targets was stimulated for 4 consecutive sessions of 1000 pulses each, for a total of 4000 pulses per target point, then shifting to the next target till all 4 were covered over 16 sessions.
Each session lasted for 580 seconds and consisted of 1000 pulses with a frequency of 10 Hz, at 90% of RMT determined in the abductor pollicis brevis according to the method described by Rossini et al. (Rossini et al., 1994). A total of 25 trains were administered, 40 pulses per train with 20 seconds intertrain interval. The coil handle was directed downwards at 45° of the sagittal plane to ensure that the induced electric field was perpendicular to the underlying gyrus (Zhang et al., 2006) (Fig. 1). To this end, we used the MagVenture MagPro X100 repetitive transcranial magnetic stimulator (Farum, Denmark) and a figure of eight coil (MagVenture cool B65) with an outer diameter of 75 mm.
Patients in the sham group received similar pattern of stimulation yet using a sham coil. It is magnetically shielded, yet optically identical to the active coil, producing sounds and sensations similar to the active coil without expected therapeutic effects.
A stimulus intensity at 90% RMT was employed rather than phosphene threshold in the current study since the average intensity of stimulator output is much less for RMT 40.6±6.78% (Ah Sen et al., 2017) compared to that for phosphene threshold that ranges from 75% to 85% (Mulckhuyse et al., 2011). This was supported by a pilot study of 12 patients, in which only 3 patients could perceive phosphenes and one of them developed an epileptic fit at a stimulus intensity 60% of maximum stimulator output (El Nahas et al., 2019).
Statistical analysis
Statistical analyses were done using SPSS (IBM SPSS ver. 20, NY, USA). Level of significance was defined as p < 0.05 using T test for continuous variables (results are referred to as means±standard deviation), and Chi square test for categorical ones (results are referred to as frequency and percentage). Paired samples T-Test was used to compare means±standard deviation of each group before and after rTMS stimulation. Pearson correlation was used to correlate pre-treatment visual parameter with treatment efficacy.
Results
Thirty-two patients completed the study, 25 males and 7 females. The active group consisted of 21 patients: 17 males (81%) and 4 females (19%) with a mean age of 58.3 (±11.7) years. While the sham group consisted of 11 patients; 8 males (72.2%) and 3 females (27.3%), mean age 55 (±8.5) years. There was no significant difference in type of VFD or side of lesion between the two groups (Table 1).
Demographic data and Clinical characteristics at baseline of Active and Sham groups
Demographic data and Clinical characteristics at baseline of Active and Sham groups
MD, mean deviation; VFI, visual field index; VFQ-25, visual functioning questionnaire-25; *Chi test.
Clinical characteristics of studied sample at baseline (Table 1): Mean duration of illness of the active group was 5.9 (±5.8) months compared to 7.1(±3.3) months in the sham group being statistically non-significant. There was no statistically significant difference regarding baseline mean deviation (MD), visual field index (VFI) values and visual functioning questionnaire (VFQ-25) between active and sham groups.
Inter-group difference between baseline and post-stimulation (Table 2): Mean difference of MD was significantly greater in the active group than sham group for the right and left eye; p = 0.04, and 0.003, respectively. Mean difference of VFI showed significant difference between both groups in favor of the active group; right VFI and left VFI; p = 0.001 and 0.008, respectively. Mean difference of VFQ-25 was also significant in favor of the active group; p = 0.04.
Post rTMS: inter-group mean difference of perimetry and VFQ-25 scale
MD, mean deviation; VFI, visual field index; VFQ-25, visual functioning questionnaire-25. *p value is significant if < 0.05.
Intra-group difference between baseline and post-stimulation (Table 3):
Intra-group comparison of mean values: MD, VFI and VFQ-25 for Active and Sham groups at baseline and after rTMS
MD, mean deviation; VFI, visual field index; VFQ-25, visual functioning questionnaire-25. *p value is significant if < 0.05.
The active group showed statistically significant improvement in MD values post-stimulation for the right and left eyes (p = 0.008 and 0.001; respectively). Also, there was statistically significant improvement of the VFI values of the right and left eyes (p = 0.002 and 0.02; respectively). While VFQ-25 values showed a trend towards improvement in the active group (p = 0.06) (Fig. 2). On the other hand, none of the measured parameters showed significant improvement in the sham group.
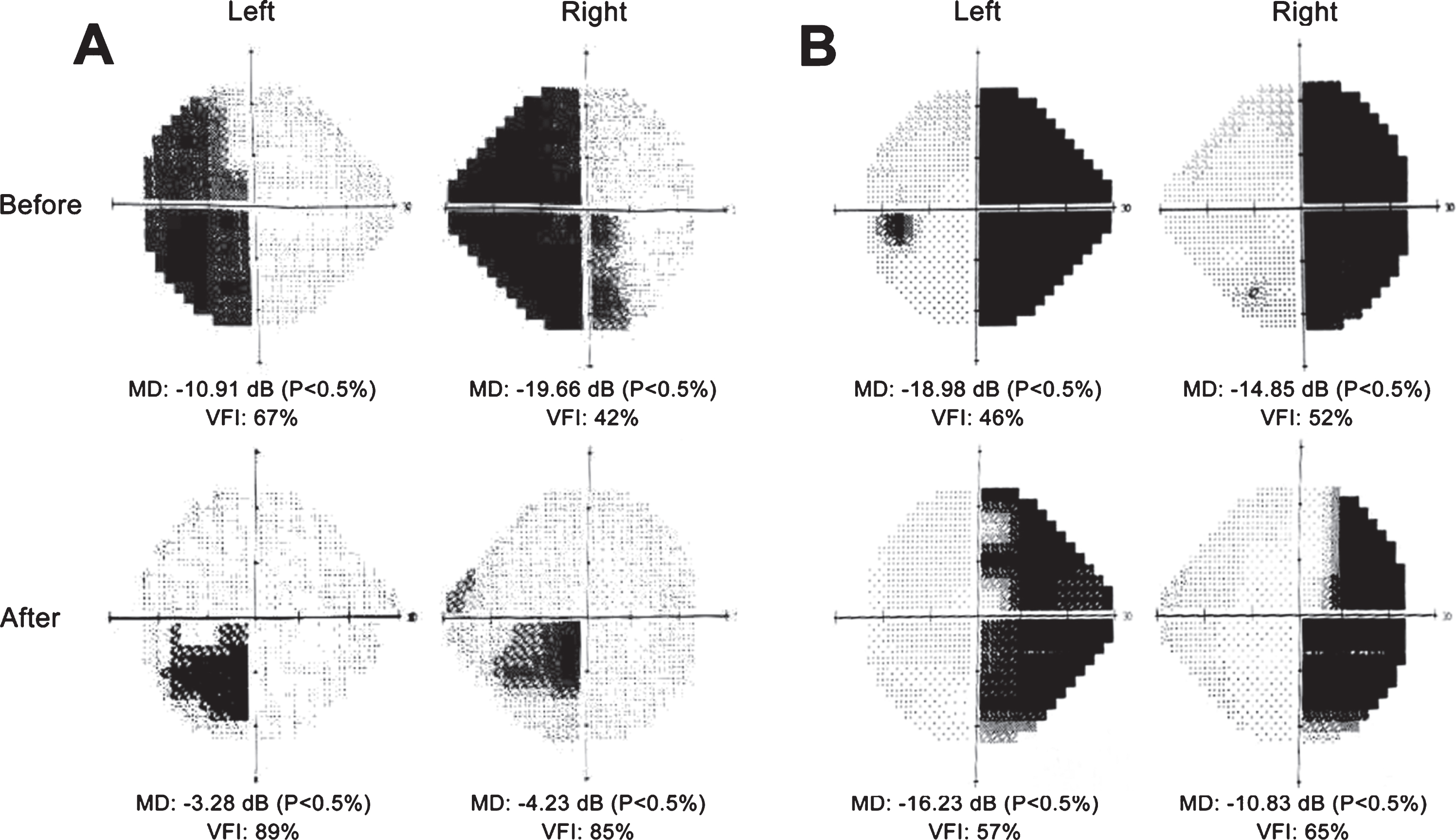
Automated perimetries of two patients (A and B) before and after intervention: (A) shows good improvement of right HHA with residual defect in right lower quadrant. (B) shows moderate improvement of left HHA with clearance of VF being more apparent in the upper medial field.
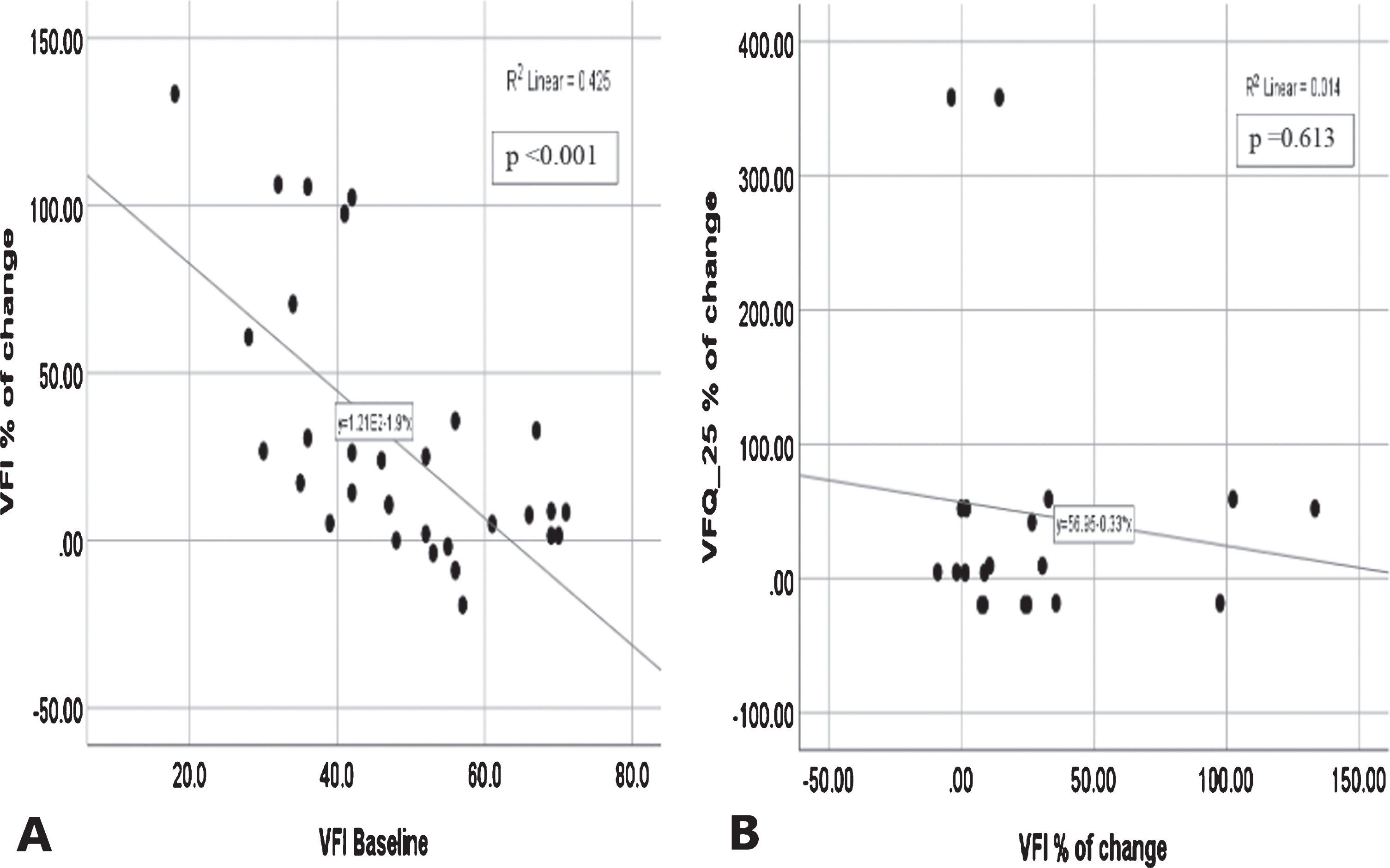
Active group scatter plot showing correlation between percentage of change VFI after intervention and (A) baseline VFI, (B) percentage of change VFQ-25 after intervention.
We correlated VFI at baseline with the percent of change after active r TMS sessions, it was found that the improvement was better with milder deficit rather than major ones (statistically significant correlation; r = – 0.652, p < 0.001) (Fig.3). On the other hand, percent of change in VFI did not show any significant correlation with percent of change inVFQ-25 after active r TMS sessions (r = – 0.117, p = 0.613).
Discussion
Among the several therapeutic options for VFDs, non-invasive brain stimulation targets the area of infarction in the occipital lobe (Sabel et al., 2020) whereas, behavioral training with VRT adopts the concept of border training through presenting visual stimulation to the eye (Sabel et al., 2011). Plow et al. 2011, combined both techniques where anodal DCS was applied to both occipital poles in conjunction with VRT, with resultant visual field improvement. However, this improvement did not translate into better visual functional recovery. And it is not clear whether the reported improvement could be attributed to VRT or to the effect of DCS on the intact side (Plow et al., 2011).
In contrast, the current study employed a different technique by stimulating the border of the infarcted region using navigated rTMS. We reasoned that might be equally or more effective than presenting visual stimuli to the eye (Kasten et al., 1998). The use of a neuro-navigation system based on patient’s MRI allowed for the precise identification and targeting of cortical perilesional areas which can be replicated accurately for each patient along the sixteen rTMS sessions. We assumed that seemingly healthy, perilesional brain areas can be selectively stimulated to restore visual field in cortical VFDs. In line with our hypothesis, it was previously suggested that intact islands in the visual cortex and around a lesion can be activated by repeated stimulation. This was referred to as border training and it aims to train and restore vision at the border of the scotoma (Raffin et al., 2020). Areas adjacent and functionally related to infarcted tissue can take over some of the lost function as shown by a recent study demonstrating resting state functional connectivity between the occipital cortex and other brain regions in patients with HHA. This suggests a possible role of precuneus and occipital pole connectivity on attention-modulated visual field improvement (Halbertsma et al., 2020). Also, Nelles et al. used functional MRI to show activation of the extra-striate cortex during stimulation of the hemianopic field (Nelles et al., 2007). Moreover, it has been reported that the brain tends to neglect the impaired field of vision, which results in non-use of the areas of residual function and thus depriving them from any synaptic connectivity (Dorothe A Poggel et al., 2006).
Our approach is in line with studies on motor recovery, where areas adjacent to a lesion of the motor cortex were shown to be able to take over the function of the injured tissue (Liepert et al., 2000).This is supported by the presence of markers suggestive of neurogenesis, axonal sprouting, and gliogenesis in human post-stroke perilesional brain tissue (Jin et al., 2006; Sanin et al., 2013). Thus, the improvement of VF defect reported in our study can be ascribed to the ability of rTMS to stimulate areas of residual vision around the infarcted tissue, that might have an increased threshold to visual stimuli and are reflected in perimetry charts as grey areas (Sabel et al., 2018).
Our study included a homogenous group of lesions restricted only to cortical infarctions, the stimulus was directed to the perilesional cortical areas that showed no evidence of infarction after 3 months of stroke, assuming that these areas can be activated to restore part of the impaired visual field.
Results showed significant improvement, objectively by automated perimetry, and subjectively by the VFQ-25 functional questionnaire. Similar improvement on perimetric assessment and activities of daily living was previously reported by Mueller et al. 2003, using VRT wherein they included optic nerve lesions, in addition to cortical lesions (Mueller et al., 2003).
The observed improvement is not likely to be the result of spontaneous recovery because the duration of VFD was beyond 3 months and up to 24 months from onset. In most studies, improvement beyond the first 3 months was rarely reported (And & Kolmel, 1991; Cassidy et al., 1999; Gray et al., 1989). Moreover, all of our patients reported that their visual fields were stable before therapy, and that they noted relatively rapid improvements during the short rTMS period.
Conclusion
Sixteen sessions of high frequency perilesional rTMS resulted in improvement of cortical VFDs both by perimetry and on a subjective basis even beyond 3 months of stroke. Verification of these results on a larger sample and in different brain pathologies is required, together with a long-term follow up study for the endurance of therapeutic effects. Confirmation of the efficacy of this technique (navigated perilesional TMS stimulation) might open new avenues for rehabilitation of other post-stroke sequalae such as motor and speech deficits. Also, combined application of perilesional stimulation with VRT may have an augmenting effect on visual field restoration.
Conflict of interest
None
Footnotes
Acknowledgments
Ain Shams neuromodulation research lab and equipment used in this study were established through a grant from the Science & Technology Development Fund (STDF) in Egypt [project ID 2893, capacity building]. The funding source played no role in the planning, analysis, or writing of this article.
Funding sources
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.