
Abstract
Background:
Traditional repetitive Transcranial Magnetic Stimulation (rTMS) remains applicable in speech studies on healthy participants. Although the procedure of inducing speech arrest by rTMS has been used for over 25 years, there are still significant discrepancies in its methodology.
Objective:
The study aimed to simplify and improve the old methodology of triggering speech arrest by (rTMS). Our goal was to establish the best step-by-step algorithm and verify the procedure on a representative group of participants.
Methods:
47 healthy, right-handed volunteers (23 men and 24 women) at a median age of 23 (range 19–34) were included in the study. Handedness was determined using the Edinburgh Handedness Inventory Test. After setting the individual’s motor threshold (MT) and heuristic choice of the place of stimulation, which targeted Inferior Frontal Gyrus (IFG), participants were asked to count downwards from 20 to 10. While counting, a series of 2-second pulses was generated at a frequency of 2 Hz at 120% or 150% of MT. The procedure was video-recorded and subsequently assessed by 3 independent reviewers and self-assessed by participants on visual analogue scales for the effect and comfort of stimulation.
Results:
Speech arrest was induced in 45 people (95.7%). Language dominance was determined to be either left-sided (for 42.2%) or bilateral (55.3%). Total speech arrest was observed more often in participants for whom Broca’s area was active exclusively in the left hemisphere.
Conclusion:
In our study, we present the step-by-step procedure for a simplified, as far as possible, methodology of inducing speech arrest using rTMS with its verification on a representative group of right-handed healthy individuals. Our results prove that the chosen stimulation parameters present a good efficacy ratio and seems to be justified. The traditional applications of rTMS in speech studies may be highly broadened if the methods used are further improved and simplified.
Abbreviations
Transcranial Magnetic Stimulation;
Edinburgh Handedness Inventory;
Laterality Index;
Motor threshold;
Visual analogue scale;
First dorsal interosseous;
Motor Evoked Potential;
Inferior Frontal Gyrus
Introduction
Since 1991 when Pascual-Leone first described speech arrest induced by repetitive Transcranial Magnetic Stimulation (rTMS) (Pascual-Leone, Gates, & Dhuna, 1991), new tools have emerged and enabled further studies of speech centre localisation and its function. TMS regionally manipulates cortical activity by excitation or inhibition of neurons for tens of milliseconds (Hallett, 2007). The external coil operates based on Faraday’s law of electromagnetic induction as it produces a rapidly changing magnetic field that penetrates the skull and induces an electrical current in the cortical neurons. In relation to Faraday’s law, the coil is the primary inductor, while the cortical region below the coil is the secondary conductor. Pascual-Leone et al. presented an innovative method of cortical stimulation with the use of rTMS (Pascual-Leone et al., 1991). Here, the impulses of specific frequency offer an insight into the neuroanatomical basis of brain functions (Devlin & Watkins, 2007; Hartwigsen & Siebner, 2013) and make it possible to examine speech arrest in real-time and on conscious patients. While there is a growing body of literature on rTMS, there remain discrepancies across studies in terms of the frequency, handling task, coil type, as well as time and place of stimulation (Epstein et al., 1996, 1999, 2000; Jennum, Friberg, Fuglsang-Frederiksen, & Dam, 1994; Michelucci et al., 1994; Wassermann et al., 1999). Additionally, there is no unified and effective protocol and only a few studies reported the individuals’ descriptions of the sensation of stimulation (Epstein et al., 1996; Pascual-Leone et al., 1991). It is important to distinguish between motor and nonmotor speech disruption, as suggested by Stewart et al. (Stewart, Walsh, Frith, & Rothwell, 2001). The first is associated with activity in the mentalis muscle, with subjects often feeling as though they had lost control of their facial muscles, and the second occurs when the speech disruption was not associated with any activity in the mentalis muscle and subjects often described a feeling of being unable to ‘get the word out.’
Clinical rationale for the study
High temporal resolution rTMS offers a non-invasive insight into speech organisation in the brain even without precise but not always available frameless stereotaxy used to target brain regions. The objective of this study was to reconsider the old methodology (Epstein et al., 1996; Pascual-Leone et al., 1991) to establish an easily available method for speech arrest based on anatomical landmarks and verify the updated procedure on a representative group of right-handed individuals.
Material and methods
Ethical approval
All procedures performed in studies were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The local ethical board of the Poznan University of Medical Sciences approved this study (approval No KB 523/2011) and all participants gave prior written informed consent.
Study group
Participants were included in the study if self-determined as right-handed. The group of 47 healthy adults consisted of 23 men and 24 women and included three of the paper’s authors. All participants were Polish native speakers with a median age of 23, ranging from 19 to 34 years of age.
Study design
Determination of handedness
The Edinburgh Handedness Inventory (EHI) protocol was used to confirm all participants’ self-declared handedness (Oldfield, 1971). The participants with Laterality Index (LI) ranging from 48 to 100 qualified as right-handed and were included in the study.
The EHI is the most widely known and commonly adopted handedness determination method (Edlin et al., 2015). Alternative assessing tools included the Stanley Coren Handedness Inventory (Coren, 1993; Khedr, Hamed, Said, & Basahi, 2002), a 14-item handedness inventory (Epstein et al., 1999; Raczkowski, Kalat, & Nebes, 1974) and a handedness self-report (Epstein et al., 1996). However, these methods lacked the standardisation offered by EHI. Although the EHI is limited by its subjectivity, when administered correctly (Edlin et al., 2015), it makes it possible to compare the handedness test results. In our protocol, we used the original questionnaire and decile values of the Handedness Laterality Index (LI).
Determination of stimulation threshold
All subjects filled out a screening questionnaire (Rossi et al., 2009) along with its subsequent update (Rossi, Hallett, Rossini, & Pascual-Leone, 2011; Rossini et al., 2015). The presence of any contraindication was an excluding criterion.
The intensity of the subsequent rTMS was based on an individual’s motor threshold (MT). MT is the level of stimulator output necessary to elicit a visible twitch of any hand muscle on the contralateral side to the single-pulse stimulation over the motor cortex. To establish MT, we follow a previous ascending staircase protocol. We started with low (subthreshold) intensity and increased it to the minimum intensity required to elicit a twitch (Pridmore et al., 1998; Schutter & van Honk, 2006).We administered 10 pulses per intensity value to check for twitches, applying a 5 out of 10 rule (if a minimum of 5 out of ten pulses elicited a twitch, we considered it as appropriate, following the Rossini-Rothwell method (Schutter & van Honk, 2006)).
MT is used to determine the percentage of rTMS stimulator output needed to induce speech arrest. MT reflects differences in neuronal density and excitability (Hallett, 2007) and it differs across individuals. MT is determined using single TMS pulses and EMG records of compound motor action potentials from the right first dorsal interosseous (FDI) muscle or the presumed dominant abductor pollicis brevis (Pascual-Leone et al., 1993). Alternatively, MT can be established as the percentage of stimulator output required to elicit a Motor Evoked Potential (MEP) of > 100μV (Watkins & Devlin, 2008) or > 50μV (Flitman et al., 1998) in more than 5 out of 10 consecutive pulses (Rossi et al., 2011). Two strategies include assessing active and resting motor potential (Rossi et al., 2011; Rossini et al., 2015). Interestingly, MT estimates obtained using these two methods do not differ by more than 2% of the maximum stimulator output (Epstein et al., 1996). We assessed the visible twitch effect of any dominant hand’s muscle following a single TMS pulse over the contralateral motor cortex in 5 out of 10 pulses (based on active motor potential), as this is the simplest and most time-efficient methodology. Mean percentage of stimulator output to generate the effect was 59.6 % (range: 40-82).
One of the first rTMS studies on speech reported induction of epileptic seizures (Wassermann et al., 1999). Following improvements to safety guidelines, there have been no reports of serious adverse events to date (George et al., 2002).
Speech arrest
The stimulation was localised 8 cm from a tragus measured tangentially to the preauricular line (Epstein et al., 1996) and targeted the inferior frontal gyrus (IFG). A figure-eight (butterfly) coil measuring 75 mm in diameter (C-B60) and generating a biphasic pulse was placed horizontally and stabilised as the subjects were seated and asked not to move their heads. A Magnetic Stimulator MagPro R30 (Medtronic), operating at the frequency of 2 Hz and a duration of 2 seconds, proved to be most effective in our preliminary studies.
The strength of the stimulus was calculated as 120% of an individual’s MT. While participants were counting downwards from 20 to 10, stimulation was triggered randomly over the left hemisphere. If no effect was observed, we elevated the strength of the stimulus to 150% of an individual’s MT. After a 15-minute break, the procedure was repeated over the right hemisphere. The procedure was recorded using a 12 megapixel camera. The further points of methodology are described and discussed in detail in the Discussion section.
Evaluation of the results
Three independent investigators as well as the participants themselves assessed the stimulation effects after watching video recordings. A positive response was declared when the subject was unable to utter a numeral - ‘total speech arrest’, or when inadequate or semantically changed numeral was produced - ‘subtotal speech arrest’ (Thiel et al., 2005). Participants assessed the study’s effect and comfort for left and right hemisphere stimulation using the visual analogue scale (VAS) designed by the authors of the manuscript. Volunteers marked a cross on two 0 –10 cm scales. In the case of the first one, 0 cm meant minimal speech arrest effect and 10 cm meant maximal speech arrest effect; for the second one, 0 cm meant minimal comfort during the stimulation and 10 cm meant maximal comfort. The scale was verified in the pilot study. The participants described the speech arrest for each stimulated side as the ‘Cannot recall a word’ and ‘Cannot articulate a word’ effects.
Tasks performed during rTMS language mapping vary significantly and may involve counting (Epstein et al., 1996, 1999; Jennum et al., 1994; Michelucci et al., 1994; Pascual-Leone et al., 1991), object naming (Wassermann et al., 1999), reading (Jennum et al., 1994; Wassermann et al., 1999), pseudoword reading, verb generation, action naming (Stewart et al., 2001). Converging evidence from direct cortical stimulation and functional MRI revealed that object naming is a more sensitive measure of speech localisation than counting (Petrovich Brennan et al., 2007). This finding suggested that automated speech tasks, such as counting, may not fully engage putative language networks and therefore are not optimal for language localisation.
Conversely, sequential number counting, an overlearned speech pattern, may be preserved in aphasic patients, which makes it particularly convenient for language mapping. This approach is reasonable in patients unable to perform more complex tasks or as the first step in a detailed language mapping (Petrovich Brennan et al., 2007). Here, we asked participants to count downwards which was not an automated speech task.
We increased the cognitive challenge by asking participants to count downwards. This task requires inhibition of perceptual or memory triggers, using a Supervisory System (Shallice, 2004), which executes monitoring, overseeing and controlling during automatic attention processes. Counting downwards, similarly to random number generation, is an attention-demanding task that engages working memory and executive processes. We chose these tasks as they require: holding information ‘on the line’, suppression of habitual counting and internally driven response generation and monitoring of responses (Jahanshahi et al., 1998).
Statistical analysis
The analysis was performed using StatSoft Statistica v10.0 and Analyse-it for Microsoft Excel v3.53 software. Methods of descriptive statistics, such as frequency (n), and arithmetic means for normally distributed variables were adopted. Otherwise, medians were used. The Shapiro–Wilk test was used to assess normality. To compare differences between the groups, the chi-square test or Fisher’s exact test were used for categorical variables, and the Mann–Whitney U test for continuous variables. Correlations between the self-assessed efficacy and comfort of stimulation and motor threshold and efficacy or comfort parameters were calculated using the Spearman rank correlation method. A p-value below 0.05 was regarded as statistically significant.
Results
A positive effect of stimulation, i.e. speech arrest, as assessed by investigators, occurred in a total of 45 individuals (95.7%). The mean stimulator output to generate the effect was 59.6%; range 40–82%. In 30 out of 45 (66.7%) participants, 120% of MT stimulator output was enough to induce speech arrest while the remaining 15 (33.3% of participants) required stimulation with 150% of MT. Table 1 shows the participants’ mean motor threshold characteristics based on the general effect of the stimulation. In two participants, no effects were elicited during stimulation. They did not respond to stimulation of 150% of MT. We decided not to exceed the strength of the stimulus over 150% of MT in these two participants due to the level of their discomfort. Table 2 represents the parameters used to induce the positive speech arrest effect in the remaining participants.
Participant’s mean motor threshold characteristics due to the general effect of the stimulation
Participant’s mean motor threshold characteristics due to the general effect of the stimulation
Speech arrest’s characteristics according to the localization of the effect
a–description in the text; * - any of pairs marked with an asterisk differ at P < 0.05.
Speech arrest occurred after stimulation over both left and right hemispheres in 26 people (57.8%) and exclusively over the left hemisphere in 19 participants (42.2%). None of them exhibited any effects after stimulation applied exclusively over the right hemisphere. The concordance rate between the effect and no effect after stimulation over the left and right hemisphere was 59.6%; positive concordance rate –55.3% (effect after stimulation over the left and right hemisphere); negative concordance rate –4.3% (no effect after stimulation over the left and right hemisphere). There were no significant differences in stimulation parameters between the group exhibiting positive speech arrest with stimulation applied exclusively over the left hemisphere and bilateral stimulation.
The stimulation evoked a total speech arrest in 38 (84%) participants. In participants with bilateral positivity of speech arrest, the stimulation elicited effects predominantly over the left hemisphere. Total speech arrest as an effect of left hemisphere stimulation was observed more often in those with effects over the left hemisphere exclusively when compared to participants with bilateral positivity (OR = 3.33 (0.77–14.42), p = 0.182). There was a significant difference in the total speech arrest between participants who exhibited an effect with stimulation applied exclusively over the left hemisphere and those exhibiting bilateral effect with stimulation over the right hemisphere (OR = 5.33 (1.25–22.82, p = 0.027). The difference in the prevalence of subtotal effect for all simulations in participants with bilateral speech arrest regardless of the stimulated hemisphere was significant (OR = 4.23 (1.10–16.31), p = 0.049). Table 3 summarises the details of stimulation effects according to effect type.
The characteristics of the effect’s type
*Calculated with Fisher’s exact test.
Table 4 presents the participants’ self-assessment of stimulation. All participants with the effect of speech arrest experienced the ‘Cannot articulate a word’ effect more often than the ‘Cannot recall a word’ effect (62% vs. 38%). The self-assessed effect of stimulation did not correlate with its comfort, neither for the left (r = –0.269, P = 0.119) nor the right hemisphere (r = –0.067, P = 0.708). Neither the individual’s motor threshold nor the final stimulator output used to generate speech arrest correlated with the grade of subsequent speech arrest effect assessment. An increasing percentage of the stimulator output used in a speech arrest induction significantly lowered stimulation comfort for the left hemisphere (r = –0.354, P = 0.037) but not for the right (r = –0.078, P = 0.654).
The characteristics of the participant’s self-assessment
a–visual analogue scale (range 0–10 cm); * - any of pairs marked with an asterisk differ at P < 0.05.
Finally, in participants with speech arrest present exclusively following the stimulation over the left hemisphere, the self-assessed effect of the stimulation tended to be higher than in the group with positive bilateral speech arrest after stimulation over the left or right hemisphere. However, the self-assessed mean comfort of the stimulation was comparable in the two groups, as was the mean percentage of stimulator output needed to generate the effect.
We proposed a standardised procedure for a test of speech arrest (Fig. 1.), which included the latest improvements of rTMS in studies on speech function. The procedure is efficient and simple to follow with no need to use tools such as neuronavigational software and hardware which are not always readily available. To the best of our knowledge, it is the biggest study on speech arrest induced by rTMS in right-handed healthy participants so far.
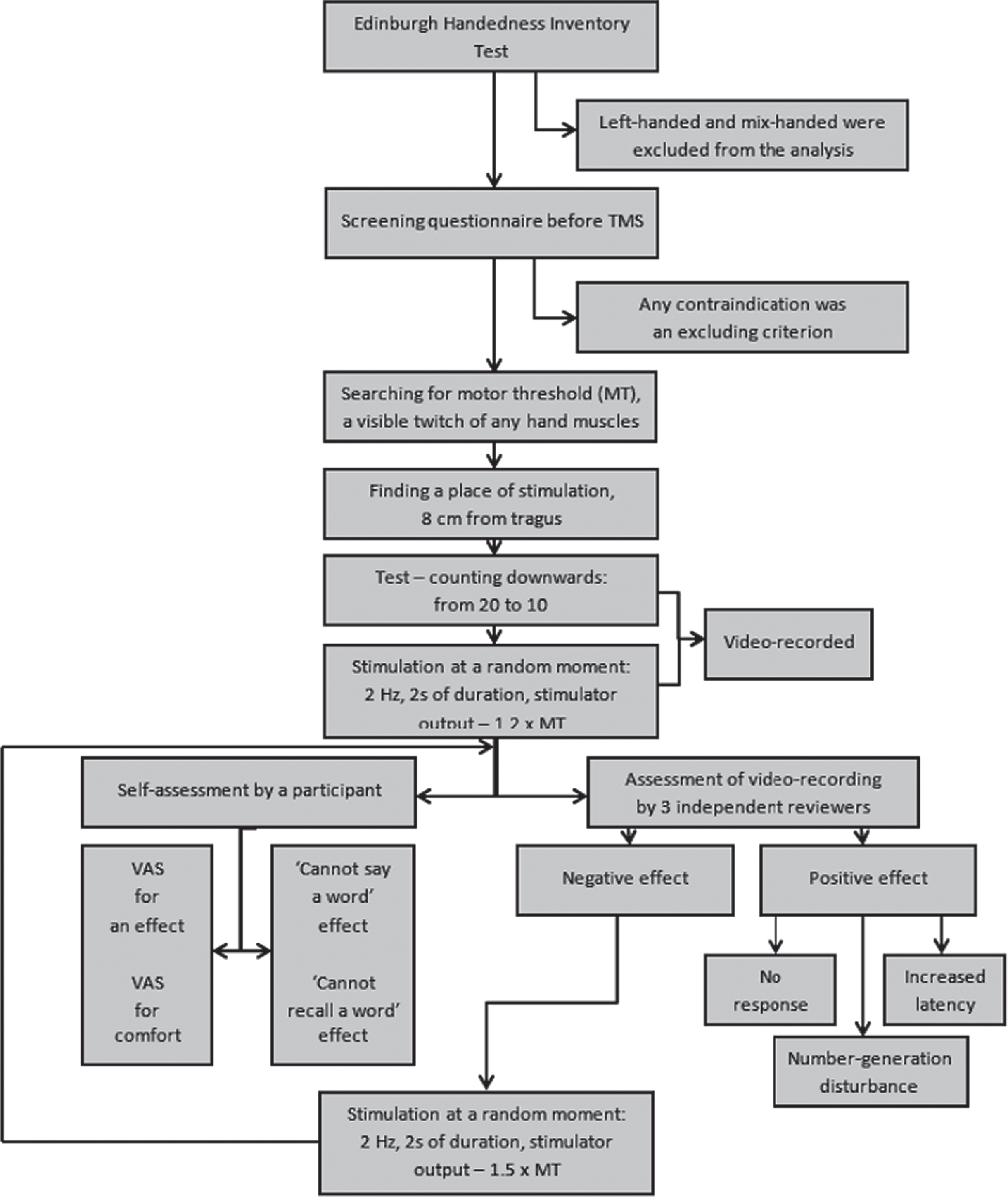
Step-by-step procedure of inducing speech arrest by repetitive Transcranial Magnetic Stimulation. Description in the text.
The motor cortex for orofacial, pharyngeal, laryngeal muscles and Broca’s areas are involved in the motor component of speech. The motor cortex is linked to the execution of speech production and motor speech control. Broca’s area, located in the IFG, functions as the centre of lexical, grammatical and phonological processing (Sahin, Pinker, Cash, Schomer, & Halgren, 2009). Since both the motor cortex and Broca’s area are functionally connected (Greenlee et al., 2004). IFG stimulation may induce speech disruptions.
Functional, anatomic or heuristic criteria are mostly applied to target and stimulate a chosen cortical region (Devlin & Watkins, 2007). When the functional criteria are used, participants perform a task while being stimulated (Gough, Nobre, & Devlin, 2005). Currently, neuroanatomy gives an effective method of speech centre localisation. A more precise navigated TMS involves using a traditional TMS coil fused with a frameless stereotactic MRI or CT brain scan-based online navigation system (Tarapore et al., 2013). Fiducial markers or anatomical landmarks enable localised stimulation with an error of about 5.7 mm (Ruohonen & Karhu, 2010) in navigated TMS. However, the availability of navigated TMS is still limited making it difficult to adopt in clinical neuroscience.
We decided to adopt a methodology to make the whole procedure as accessible as possible. Traditionally, rTMS coil positioning may follow the heuristic criteria using a 10–20 system (Pascual-Leone et al., 1991) or be based on the external anatomical points such as vertex, inion or tragus. We took scalp measurements (Epstein et al., 1996) as this method does not require the use of sophisticated tools.
Stimulation parameters
In the previous studies, stimulation frequencies ranged from 4 (Epstein et al., 1996, 1999, 2000), 5–18 (Wassermann et al., 1999), 16–20 (Michelucci et al., 1994), 25 (Pascual-Leone et al., 1991) to 30 Hz (Jennum et al., 1994). However, a study by Epstein and colleagues (Epstein et al., 1996) revealed that rates as low as 4 Hz are highly effective at blocking speech output, and limit the accompanying discomfort. Additionally, train length can vary from 1 second (Jennum et al., 1994) to 10 seconds (Pascual-Leone et al., 1991). In our study, we tried to minimise any possible risk and assess the efficacy of 2-second stimulation at 2 Hz. We achieved a 95.7% stimulation effectiveness which supports the application of this methodology.
There was variability across the coils used: Cadwell Rapid-Rate Magnetic Stimulator (Michelucci et al., 1994; Pascual-Leone et al., 1991), Cadwell High-Strength Magnetic Stimulator (Epstein et al., 1996; Wassermann et al., 1999), MagPro biphasic (Jennum et al., 1994), custom circular and figure-eight (butterfly) coil (Stewart et al., 2001), which was the most widely adopted variant at the time this study took place (Tarapore et al., 2013). It is recommended that the coil be oriented horizontally as then the stimulation bundle penetrates cortex areas most effectively (Epstein et al., 1996). Too high parameters of stimulator output may exceed the pain threshold and induce interpretational obstacles such as facial muscle contraction. Therefore, as recommended by Epstein (Epstein et al., 1996), we find it reasonable to use 120% of MT in the first speech arrest attempt and 150% of MT in the second attempt if necessary. Importantly, the increasing stimulator output percentage correlated significantly with discomfort assessment. Therefore, the upper limit of the stimulation values should be deemed to be 150% of MT (Mottaghy, Sparing, & Töpper, 2006).
Video recording
The video recordings enabled the precise documentation of the stimulation procedure and a non-biased analysis of its effects and positivity (Lioumis et al., 2012) by several independent reviewers. Additionally, the study volunteers could be consulted about the experiences and accompanying emotions. This enabled more thorough documentation of the experiment (Lioumis et al., 2012).
Assessment
We decided to compare the effects of speech arrest across participants by subtyping them (Thiel et al., 2005). Our methodology had the second-highest efficacy of positive speech arrest in comparison with seven previously published rTMS studies (Tarapore et al., 2013).
Interestingly, total speech arrest was observed significantly more often in participants with a speech centre active exclusively in the left hemisphere (Table 3). Participants whose speech centre was active bilaterally tended to present a subtotal stimulation effect, especially because of the effect for the right hemisphere. This is in favour of the hypothesis that speech centre activity inhibition has a greater impact on its function when the speech centre is located exclusively in the left hemisphere. Knecht et al. (Knecht et al., 2000) as discussed by Devlin and Watkins (Devlin & Watkins, 2007), presented similar findings where strongly lateralised subjects were more severely affected by unilateral TMS than those with more bilateral language organisation. Considering pre-morbid differences, the right hemisphere is more or less receptive to language before any reorganisation occurs. Essentially, the right hemisphere may play an important role in the determination of the likelihood of the right hemisphere compensation following left-sided damage.
Self-assessment
We introduced the novel procedure of speech arrest self-assessment based on a special scale, inspired by the Visual Analogue Scale used in pain assessment. The volunteers were also asked about the level of discomfort while being stimulated to consider the ratio safety/efficacy. We further suggest that the participants should be asked whether they assess the effect of stimulation as ‘Cannot recall a word’ and ‘Cannot articulate a word’ to get an insight into the subjective experience of the stimulation.
Speech arrest results
Khedr et al. (Khedr et al., 2002) investigated right-handed subjects and recorded left-sided language cerebral dominance in 87.5%, bilateral cerebral representation in 8.2%, and right-sided language cerebral dominance in 4.2%. In our study, we present the opposite results. Speech arrest was induced after stimulation over the right and left hemispheres in 57.8% and exclusively over the left hemisphere in 42.2% of volunteers. The differences in the results may result from the methodology applied. Khedr et al. (Khedr et al., 2002) considered only total speech arrest as an effect of the stimulation and used the Stanley Coren Handedness Inventory (Coren, 1993) to assess the participants’ handedness. The predominance of the bilateral positivity of speech arrest may be supported by Cogan et al. (Cogan et al., 2014) who established a bilateral sublexical speech sensory-motor system. Hickok et al. (Hickok & Poeppel, 2007) and Price et al. (Price, 2010) also demonstrated bilateral speech centre activity. The activation of the right inferior frontal cortex in language processing has been shown in both aphasic patients and healthy participants (Raboyeau et al., 2008).
There is a growing body of evidence that both hemispheres may have similar relevance to the process in the healthy brain (Hartwigsen & Siebner, 2013). The right cerebral hemisphere significantly contributes to normal language processing (Lindell, 2006). Furthermore, the right hemisphere may be either facilitating (Raboyeau et al., 2008) or deleterious (Lindell, 2006; Rosen et al., 2000) in language recovery after left IFG damage, which offers exciting possibilities in the domain of neurorehabilitation (Flöel et al., 2012).
Limitations of the methodology
Since we had limited access to advanced tools, such as navigated rTMS, when conducting this study, we were inspired by this limitation and worked towards creating a simplified, common procedure. It may be doubtful whether the activation of significantly more bilateral cortical and subcortical brain networks than previously reported results from the use of a counting task (Vanlancker-Sidtis, McIntosh, & Grafton, 2003). The coil placement was determined using the heuristic approach, which does not account for individual differences in cortical morphology. Moreover, we did not induce a speech arrest effect in two participants. We hypothesise that this may be due to increased skull thickness and decreased field permeability. However, we believe that the outcome of inducing speech arrest in over 95% of the study participants proves the reliability of our methodology.
A positive side-effect
All participants, who were doctors and medical students (including the paper’s authors), agreed that an experience of speech arrest greatly increased their understanding and empathy for people suffering from aphasia. It is an uncontested and immeasurable advantage of this cognitive research and an interesting application.
Conclusion
Repetitive Transcranial Magnetic Stimulation still constitutes an important tool in the determination of cortical speech centre activity. Involvement of the new methods enriches possible data interpretation. Our results of positive speech arrest in 95.7% of participants of a large group of 47 right-handed healthy individuals prove that the chosen stimulation parameters present a good efficacy ratio and their use in subsequent analyses seems to be justified. The traditional applications of rTMS in speech studies may be highly broadened if the methods used are further improved and simplified.
Future directions
Further studies are necessary to determine whether such results indicate that people with bilateral speech centre activity experience less extensive effects of ischemia on speech centre activity and therefore fewer instances of post-stroke aphasia. We suggest that the use of a tool such as a voice analyser might be beneficial for the objectification of speech arrest assessment in future studies.
Role of Authors
All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Conceptualisation, M.B., M.W., A.C.C. and J.H.; Methodology, M.B., M.W., A.C.C. and J.H.; Investigation, M.B., M.W., A.C.C., M.B., P.D., A.B. and J.H.; Formal Analysis, M.B. and M.M.; Resources, M.B., M.W., M.B., P.D., A.B. and J.H.; Writing - Original Draft, M.B., A.C.C. and M.B.; Writing - Review & Editing, M.W., P.D. J.H.; Visualization, M.B.; Supervision, M.W. and J.H.; Project Administration, M.B.
Other Acknowledgments
The authors thank all participants who agreed to participate in the study and the Students’ Scientific Society of Poznań University of Medical Sciences for the fruitful cooperation.
Conflicts of interest
None.