
Abstract
Background:
Most previous studies comparing the effectiveness of Plasma Exchange (PE) or intravenous immunoglobulin (IVIG) in treating Guillain-Barre syndrome (GBS) have focused on the short-term outcome at around 1 month.
Objective:
To compare the long-term efficacy of PE and IVIG at one year in adult patients with GBS.
Methods:
Eighty-one adult patients with acute GBS were randomized into two groups with a ratio of 2 : 1: PE (N = 54) and IVIG (N = 27). Patients were assessed with the Medical Research Council sum score (MRC sum score), GBS Disability Scale (GDS), and Functional assessment of acute inflammatory neuropathy (FAAIN) at baseline, ten days, one month, three months, and one year. Neurophysiological examinations were performed at baseline and three months following treatment.
Results:
There were no significant differences between groups in demographic, clinical, and laboratory data. Both treatments produced a significant improvement in all clinical rating scales in both groups that continued up to one year. There were significant differences in the time course of recovery in the MRC and FAAIN scales, with significantly more improvement in the IVIG group at 1 and 3 months, although there was no significant difference in outcome at one year. However the effect size showed measurable differences between the PE and IVIG groups across the different measures at one-year. Electrophysiological studies showed equal improvement in most measures in both groups at three months, with a slightly greater effect in the IVIG group.
Conclusion:
long term outcomes of IVIG and PE were equivalent. However the effect size showed measurable differences between the PE and IVIG groups across the different measures at one-year follow-up that indicate the superiorty of IVIG. There was also a tendency for improvement to be slightly faster in the IVIG group.
Introduction
Acute inflammatory demyelinating polyradiculoneuropathy (AIDP) is the most prevalent form of Guillain-Barré syndrome (GBS). Typically, acute motor and sensory symptoms develop with facial, bulbar, and respiratory muscle weakness. Myelin sheaths of spinal roots and peripheral nerves are frequently affected by the multifocal inflammatory process, although axons are occasionally compromised. After a few days, the weakness reaches its nadir. 25% of patients require mechanical ventilation, and 3.5% to 12% die from complications during the acute phase (R. A. Hughes & Cornblath, 2005; Y. A. Rajabally & Uncini, 2012; The Italian Guillain-Barre Study Group, 1996; Yuki & Hartung, 2012). Electrophysiological studies are essential for accurate diagnosis of GBS and distinguish between AIDP, primary axonal neuropathy, and the inexcitable and equivocal variants (Hadden et al., 1998; Yusuf A Rajabally, Durand, Mitchell, Orlikowski, & Nicolas, 2015).
GBS is believed to be an autoimmune disease produced by an immunological reaction against an infectious agent and leads to the presence of complement-binding IgM antibodies against the myelin of the peripheral nerves (Chhibber & Weinstein, 2012; van Doorn, Ruts, & Jacobs, 2008). The primary treatments are immune therapies such as plasma exchange (PE) (Chevret, Hughes, & Annane, 2017; Raphaël, Chevret, Hughes, & Annane, 2012) and intravenous immunoglobulin (IVIG) (Richard AC Hughes, Swan, & van Doorn, 2014). Clinical trials have shown that IVIG works when given within two weeks of the first sign of weakness, and PE works within four weeks (Chevret et al., 2017; Richard AC Hughes et al., 2014).
A number of randomized clinical trials (RCTs) have compared the effectiveness of PE and IVIG in treating GBS (Bril et al., 1996; Nomura, Hamaguchi, Hattori, Satou, & Mannen, 2001; van der Meché & Schmitz, 1992), with the primary endpoint being short-term outcome at around 1 month. Trials also have been conducted (Bril et al., 1996; Nomura et al., 2001; Plasma Exchange/Sandoglobulin Guillain-Barré Syndrome Trial Group, 1997; van der Meché & Schmitz, 1992) on specific groups of patients such as children (El-Bayoumi et al., 2011; Elahi, Ashfaq, Nisa, & Chachar, 2019; Saad et al., 2016), or in patients with the axonal type of GBS (Dada & Kaplan, 2004) or who received mechanical ventilation (MV) (Charra, Hachimi, Benslama, & Motaouakkil, 2014; El-Bayoumi et al., 2011). Other studies evaluated the efficacy of either IVIG (Richard AC Hughes et al., 2014; Kuwabara et al., 2001) or plasma exchange (Chevret et al., 2017; French Cooperative Group, 1987; Osterman et al., 1984; Raphaël et al., 2012; The French cooperative group, 1997) but with no direct comparison between them.
The overall conclusion from such trials has been that there is no obvious difference between outcomes, at least in the short term. The question we address here is how outcomes compare over the long term at 1 year. Only one previous study [15] followed patients over 1 year and found that although they continued to improve, both treatments were equally effective, at least when assessed with an early version (six points) of a disability scale. In the present study, we used the GBS Disability Scale (GDS), the Medical Research Council sum score (MRC sum score), and the Functional Assessment of Acute Inflammatory Neuropathy (FAAIN). Moreover, to the best of our knowledge, no clinical trial has been conducted in Egypt. Thus, we aimed to compare the long-term effect of PE and IVIG in Egyptian patients with GBS.
Material and methods
Study design, participants, and ethical approval
This study was a randomized prospective longitudinal parallel design that included 81 patients diagnosed with GBS according to the criteria of the National Institute of Neurological Disorders and Stroke (NINDS) (A. Asbury, 1978; A. K. Asbury & Cornblath, 1990) and the Brighton Collaboration (Fokke et al., 2014; Sejvar et al., 2011). The patients were consecutively recruited from the emergency department of the Neurology, Psychiatry, and Neurosurgery Hospital of Assiut University, Faculty of Medicine, Assiut, Egypt, from September 1st, 2021, to March 3rd, 2023. As the primary tertiary hospital in upper Egypt, Assiut University receives numerous referrals from different cities.
Inclusion criteria: Age ranging from 18 to 70 years within the first two weeks after onset.
Exclusion Criteria patients with metabolic and electrolyte disorders (hypokalaemia or hyperkalaemia), periodic paralysis, hypoglycemia, or malignancy, or other causes of peripheral neuropathy, other causes of acute paralysis of limbs such as ascending myelitis, myositis, inflammatory myopathies, hypothyroidism, porphyria, vitamins B1, B12 deficiency, and critical illness polyneuropathy.
This study was approved by the Institutional Review Board (IRB) of the Faculty of Medicine, Assiut University, as part of a research project with Approval Number: 17300680 and was registered on clinicaltrial.gov with ID: NCT05104762. The research complied with the 1964 Declaration of Helsinki of the World Medical Association and its subsequent revisions or a comparable ethical standard. All participants signed an informed written consent form to participate in the study.
Randomization
Patients with GBS receive PE or IVIG after being randomly classified into two groups using a closed envelope with a ratio of 2 : 1, respectively, as the IVIG is expensive and not available all the time in the hospital (see the flow chart in Fig. 1). The study was double-blind (participant and the outcomes assessor): the patients were not informed of the potential alternative therapies used in the trial. The outcome assessor did not know the type of treatment the patients received.
Baseline clinical data collection
All patients gave a complete medical history, and symptoms were quantified using the GBS Disability Scale (GDS), the Medical Research Council sum score (MRC sum score), and the Functional Assessment of Acute Inflammatory Neuropathy (FAAIN). Also, the neurophysiological assessment included nerve conduction studies, including the F wave and H reflex. Because the FAAIN was published in February 2022, we retrospectively assessed the scale at onset, ten days, one, and three months in approximately half of the patients recruited during the first six months of the trial with follow-up at one year while the remaining patients were assessed prospectively from the time of admission until the end of the year. In the current study, we retrospectively applied this scale based on the original study that validated the FAAIN in 2022. Their authors detected that the scale was reliable and valid in the functional assessment of GBS in the first validation step, which was based on a retrospective study (Lestayo O’Farrill, González-Quevedo, Gutierrez-Gil, Hernández-Cáceres, & Sistach-Vega, 2022).
Two groups were included in this study: The PE group (54 patients) underwent PE (COM.TEC- 9008021- Fresenius Kabi AG, Homburg, Germany), with 200–250 mL of plasma/ kg in five sessions (40–50 mL/kg per session) were exchanged every other day within 7–14 days with replacement by fresh frozen plasma. The IVIG group (27 patients) received IVIG (Immunoglobulin-G, Sk Plasma Co., Ltd., Seongnam, South Korea) in a dose of 0.4 g/Kg/day for five consecutive days.
Follow up
Clinical follow-up of each patient was performed using the GDS, MRC sum score, and FAAIN at ten days of treatment, then at one month, three months, and one year after treatment (Fig. 1). The neurophysiological assessment was performed at baseline and after the end of 3rd month of treatment.
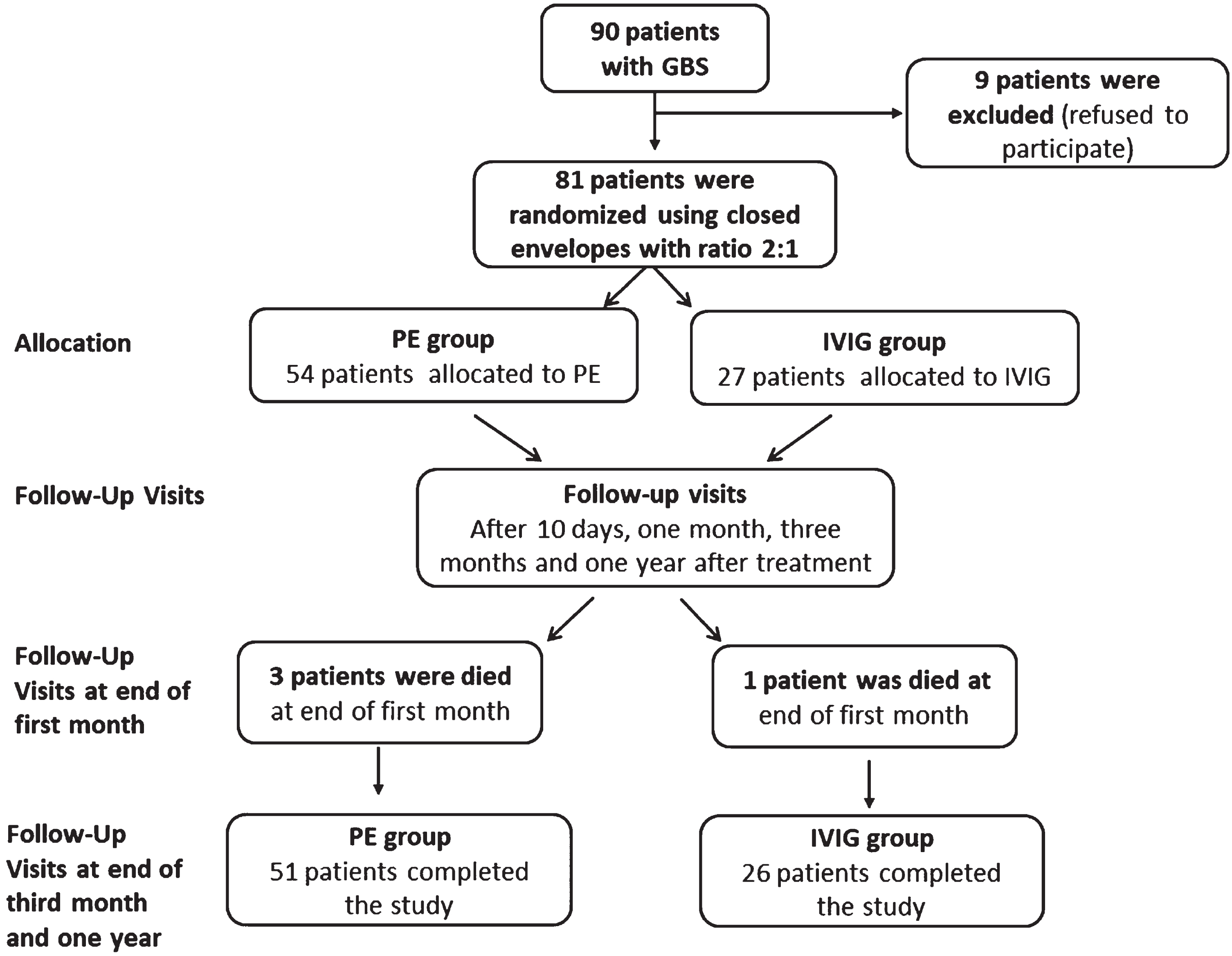
Flow chart.
Primary outcome measure
1. The GBS Disability Scale (GDS): This scale assesses the degree of disability, and it has six levels: 0 points (healthy), 1 point (minor symptoms and capable of running), 2 points (able to walk 10 m without assistance but unable to run), 3 points (able to walk 10 m across an open space with help), 4 points (bedridden or wheelchair-bound), 5 points (requiring assisted ventilation for at least part of the day), and 6 points (dead) (R. Hughes, Newsom-Davis, Perkin, & Pierce, 1978; van Koningsveld et al., 2007).
2. Medical Research Council sum score (MRC sum score): this scale assessed muscle power and gave a sum score of muscle power in both upper limbs and lower limbs in points from zero (no power) up to 60 (full power) (John, 1984; Ruud P Kleyweg, Van Der Meché, & Schmitz, 1991).
3. Functional assessment of acute inflammatory neuropathy (FAAIN) in GBS: FAAIN-GBS is a new functional assessment proposal for GBS. This scale is used to include all GBS variants. It includes two subscales (extension and intensity). The FAAIN extension subscale evaluates the number of body segments exhibiting neuropathic sensory, motor, and/or dysautonomic symptoms and/or indicators. The lumbosacral, dorsal, lower cervical, upper cervical, and cranial segments are assigned. In GBS, the intensity subscale shows the progressive decline in motor function. Both dimensions are independent and assign 7 degrees. The ultimate score is determined by averaging the two dimensions. This final score varied from 0 to 7, including 0.5, 1, 1.5, etc., and can be categorized as mild (grades 1 or 2), moderate (grade 3), or severe (grades 4, 5, or 6). FAAIN-GBS is particular for the functional evaluation of inflammatory neuropathies, such as GBS, and discriminates the transition from one functional grade to another with high sensitivity (Lestayo O’Farrill et al., 2022).
Secondary outcome measure
1. Neurophysiological studies: The median, ulnar, posterior tibial nerve (PTN), and common peroneal nerve CPN) were studied in all patients as early as possible using the Nihon Kohden Machine model 9400 (Japan), according to (Carpenter & Reddi, 2012), and three months later. F-waves can also readily be recorded from calf muscles by stimulating the tibial nerve in the popliteal fossa (Fisher, 2007; Mesrati & Vecchierini, 2004)
Statistical analysis
Statistical analysis was conducted using Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 26; Armonk, NY: IBM Corp.). Graph Pad Software Inc. prism version 8 was used for graphs. A frequency and proportion analysis was performed for qualitative variables, while quantitative variables were presented as Mean±SD. The Chi-square test was used to compare differences in frequency between the two groups, and an independent t-test was used to compare differences in means between them. A paired t-test was used to compare differences in means in the same group. One-way repeated measure ANOVA was used to assess the effect of time in each group separately. Two-way repeated measure ANOVA was used to assess group X time interactions. Non-sphericity was compensated using the Greenhouse-Geisser correction.
Results
Table 1 summarizes sociodemographic and baseline clinical data. Eighty-one participants were recruited with a mean age of 37.64±17.11 years ranging from 10–75 years old. 54 cases received plasma exchange, and 27 received IVIG. There were no significant differences between both groups regarding age, gender, onset, and duration of the antecedent events and other clinical variables.
Baseline assessment of demographic and clinical data among studied groups
Baseline assessment of demographic and clinical data among studied groups
AIDP: Acute inflammatory demyelinating polyradiculoneuropathy; DVT: Deep venous thrombosis; F: Female; GBS: Guillain Barre Syndrome; ICU: Intensive care unit; M: Male. Independent t-test was used to compare differences in means between groups. Chi-square test was used to compare differences in frequency between groups. Fisher’s Exact Test was used to when cells count less than 5.
Table 2 shows the results of the clinical follow-up. A one-way repeated measure ANOVA with the main effect of time (at admission, 10th day of treatment, end of 1st month, 3rd month, and one year) revealed a significant improvement in all clinical rating scales (P value < 0.0001) in both groups. However, two-way ANOVA repeated measure analysis with time and group as main factors revealed a significant interaction with more improvement in the IVIG group (p-value = 0.010) for MRC sum score and (p-value = 0.005) for FAAIN. There was no significant difference in the change in GDS scores (Fig. 2). Post hoc t-tests showed that differences first appeared at one month and three months in the MRC and GDS scores (p-value = 0.019 and 0.033, respectively), although the outcomes were equal at one year. However the effect size at one year for MRC sum score, and for GDS are moderate (0.43, and 0.35 respectively) suggesting a noticeable difference between the PE and IVIG groups at the one-year follow-up. In the case of FAAIN, there’s a larger effect size (0.52) at one year follow up, indicating a relatively stronger difference between the groups on this measure compared to the others. These effect sizes suggest that there are measurable differences between the PE and IVIG groups across the different measures. Larger effect sizes generally indicate more substantial differences between the groups.
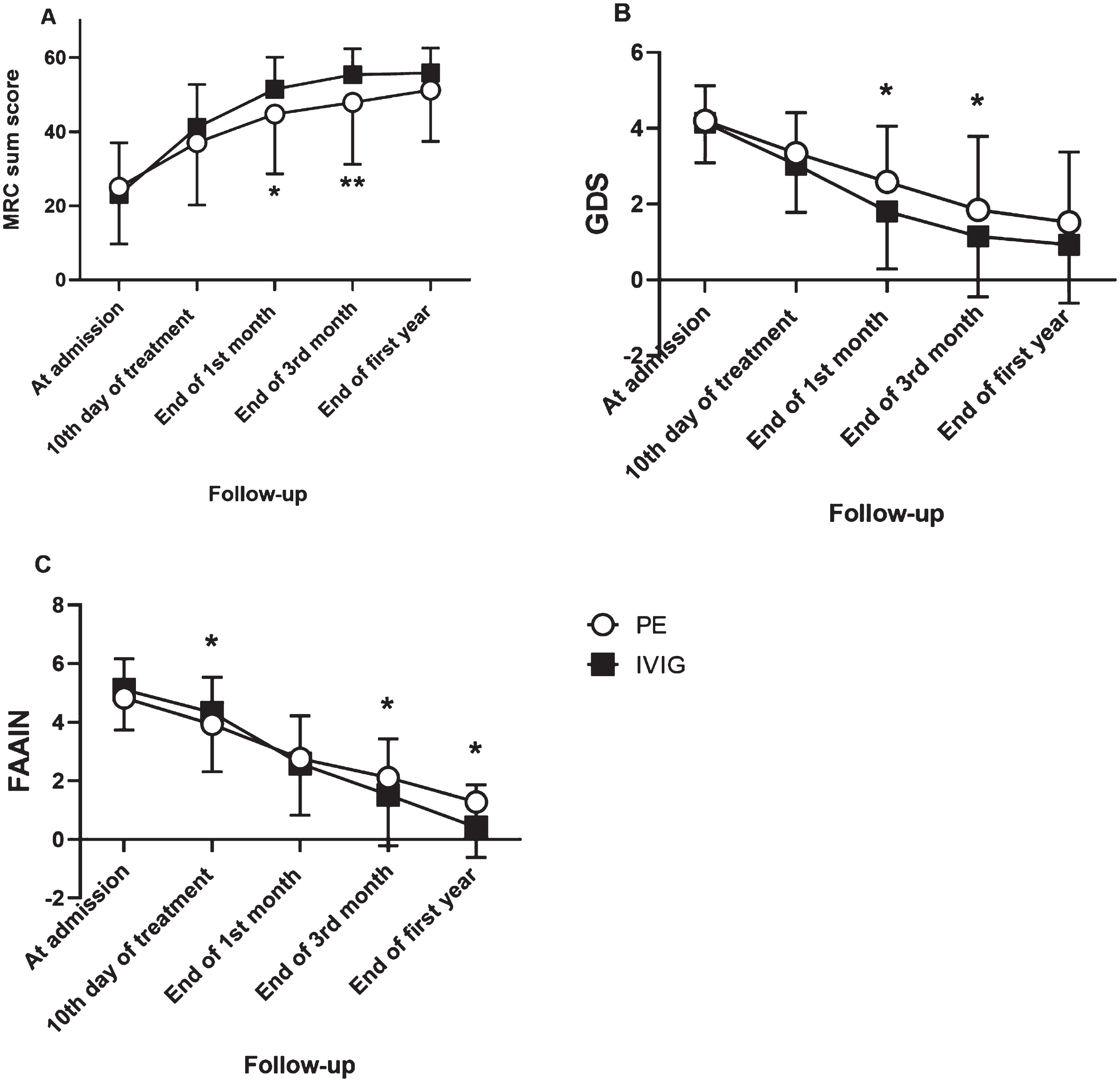
A, B, and C: show changes in the mean score of different clinical rating scales. A: Medical research council (MRC) sum score, B: GBS disability scale (GDS), and C: Functional assessment of acute inflammatory neuropathy (FAAIN). The significance between groups at each assessment was demonstrated in the figure with * for p < 0.05; and ** for p < 0.01.
Clinical outcomes along the course of disease among studied groups (long-term with follow-up after one year of survival cases)
PE: Plasma Exchange; IVIG: Intravenous immunoglobuline Independent t-test was used to compare differences in means between groups. One-way ANOVA repeated measure analysis for each group with the main effect of time, Two-way ANOVA repeated measure analysis interaction time x group. Paired t-test was used to compare differences in means in same group. *Effect sizes were estimated with Cohen’s d, indicates standardized difference between group means comparisons, with values of 0.2, 0.5 and 0.8 representing small, medium and large effects respectively (Cohen, 1988).
Table 3 summarizes the motor and sensory conduction studies at two-time points, pre-treatment and three months post-treatment. The two treatments produced equal improvements in almost all measures except for the following: F-wave latency (all four nerves, apart from common peroneal IVIG group), SDL latency (common peroneal nerve only), CMAP amplitude (common peroneal IVIG group only), sensory conduction velocity (PE group only) and median nerve sensory amplitude. There were two measures in which IVIG treatment produced a greater improvement than PE. IVIG produced a larger increase in CMAP amplitude after stimulation of ulnar or tibial nerves than PE. This was confirmed statistically by a lack of interaction in two-way rm ANOVAs (main factors of time and treatment group) on all measurements apart from the amplitude of ulnar and tibial CMAPs.
Motor and sensory conduction studies pre-treatment and three months post-treatment (survival
PE: Plasma Exchange; IVIG: Intravenous immunoglobuline Paired t-test was used to compare differences in means in same group. Two-way ANOVA repeated measure analysis interaction time x group.
Table 4 summarizes the number of patients with no electrophysiological responses pre-treatment and three months post-treatment. In all cases, the number of absent responses declined or remained the same after three months of treatment. Chi-squared analysis showed that the improvements were equal in both treatment groups. Significant recovery was observed in both median and ulnar nerves in the PE group, while there was a significant recovery of responses in the motor conduction of the posterior tibial nerve and F wave of the median, ulnar, and PTN nerves in the IVIG group.
The number of survival patients with absent electrical response of studied nerves (motor and sensory) pre-treatment and 3-month post-treatment among studied groups
PE: Plasma Exchange; IVIG: Intravenous immunoglobuline *3 patients died in Plasma Exchange group before the end of first month, **1 patient died in the IVIG group before the end of the first month.
In the current cohort, 5 patients received PE followed by IVIG within the first month of illness due to lack of improvement. Despite the significant improvement in their MRC sum score (p-value = 0.005) at the different time points (at admission, 10th day of treatment, end of 1st month, 3rd month, and one year), the mild improvement in their GDS did not reach significance. The subgroup analysis of these five patients is illustrated in the supplementary material (see Table S1, S2)
The randomized clinical trials comparing the effectiveness of PE versus IVIG in treating GBS have usually measured short-term outcome at around one month. Some papers have reported that PE is superior to IVIG (Buzzigoli et al., 2010; Dada & Kaplan, 2004; El-Bayoumi et al., 2011; Saad et al., 2016), while others found IVIG to be more effective than PE (Charra et al., 2014; El-Ghanem, Gomez, Nasar, & Souayah, 2016; Elahi et al., 2019; Kalita, Kumar, & Misra, 2019), but the overall consensus is that both treatments are similar. However, there have been very few studies of long-term outcome at 1 year, and to our knowledge, no long-term prospective clinical trial has been documented in Egypt in adult patients with GBS. There has been one retrospective analysis on children in Upper Egypt (Assiut) (Saad et al., 2016) and a second prospective analysis on mechanically ventilated children with GBS in Lower Egypt (Mansoura) but only for a short-term follow-up (4 weeks after discharge) (El-Bayoumi et al., 2011).
Clinical outcome
There was no significant difference in the number of patients in each group who needed ICU admission, MV, the number of days on MV and the length of hospital stay. This agrees with the recent findings published in a systematic review in 2023, which reported that there were no significant differences between PE and IVIG regarding the length of hospitalization and duration of MV (Zaki et al., 2023). However, this contrasts with the findings reported in other studies on adults. Van der Meché and Schmitz, 1992 and Kleyweg et al. 1994 reported that IVIG treatment required less artificial ventilation and for a shorter duration (R. P. Kleyweg, van der Meché, & Schmitz, 1994; van der Meché & Schmitz, 1992). Also, El-Ghanem et al. 2016 reported that patients who received IVIG were less likely to need endotracheal intubation and spent less time on MV, with decreased mortality and a shorter length of hospital stay (El-Ghanem et al., 2016). Moreover, Charra et al. 2014 found easier withdrawal of MV and shorter hospital stays in the IVIG group when comparing the efficacy of IVIG versus PE in the treatment of MV adults with GBS (Charra et al., 2014).
The current findings contrast with some previous results in children. Elahi et al. 2019, found that patients treated with PE had considerably longer mean ICU and ventilator stays than the IVIG group in children (Elahi et al., 2019). Also, Saad et al. 2016 reported that children were less likely to need MV and reduced the length of hospital stay after PE (Saad et al., 2016), and El-Bayoumi et al. 2011, found that children who did require MV received it for less time after PE, with a tendency for a shorter Paediatric Intensive Care Unit (PICU) stay (El-Bayoumi et al., 2011).
Effect of therapy on the primary and secondary outcomes of GBS
The current study did not find statistically significant differences between groups at baseline clinical data and at ten days after treatment; however, a significant interaction between groups along the course of follow-up (time X groups) with more improvement in the IVIG group for MRC sum score and for FAAIN at 1 and 3 months, while at one year, outcomes were equivalent. However measuring the effect sizes at one year suggested that there were measurable differences between the PE and IVIG groups across the different measures (MRC, GDS and FAAIN). Larger effect sizes generally indicate more substantial differences between the groups. There was also more improvement in a small number of electrophysiology outcomes at three months in the IVIG group.
This agrees partially with previous studies, which assessed the disability outcome of both therapies using the HDS. Van der Meché and Schmitz 1992 and Kleyweg et al. 1994, reported that the superiority of IVIG over PE was due to greater improvement in disability grade, quicker time to improve one functional grade, and a shorter time to achieve independent mobility (R. P. Kleyweg et al., 1994; van der Meché & Schmitz, 1992).
Kuwabara et al. compared the efficacy of PE and IVIG in 24 patients with IgG anti-GM1 positivity in 2001 (10 were treated with IVIg and 14 with plasmapheresis). The IVIg group had significantly lower HDS 1, 3, and 6 months after commencement and a greater chance of resuming independent locomotion at six months. IVIg therapy resulted in faster recovery and fewer residual problems than PE therapy (Kuwabara et al., 2001). In addition, Kishore et al. 2014, observed that both PE and IVIg therapies were beneficial in reducing the disability grade at all time points, i.e., at presentation, immediately after therapy, and four weeks later, with a marginal advantage of PE over IVIg (Kishore et al., 2014). Meregildo-Rodriguez and Bardales-Zuta 2021, in their retrospective investigation, found that functional outcome as measured by the modified Rankin scale (MRS) was statistically comparable among patients treated with IVIG or PE. (Meregildo-Rodriguez & Bardales-Zuta, 2021). Jacobs et al. 1996, reported that among their 31 anti-GM1–positive GBS patients, IVIG therapy was more effective than PE, with 21 patients treated with IVIg recovering faster than 10 patients treated with PE, although detailed data of prognostic factors such as distal CMAP amplitudes were not provided (Jacobs et al., 1996). Bril et al. 1996, determined that IVIG’s efficacy in treating GBS was comparable to that of PE (Bril et al., 1996).
Regarding therapeutic complications, there was no significant difference between therapies in the present study. The complications related to PE were hypersensitivity reaction (allergic reaction) in three patients (with discontinuation of PE in two patients and shifted to receive IVIG). DVT complicated by pulmonary embolism was recorded in one patient. Complications related to IVIG included DVT in two patients with no allergic reactions reported. This agrees with the findings reported in a recent systematic review in 2023, which demonstrated that the risk of patients experiencing complications after treatment with PE and IVIG was statistically insignificant (Zaki et al., 2023). However, Bril et al. 1996 found that IVIG may be administered safely without an excessive relapse risk despite a greater complication rate in patients treated with PE (Bril et al., 1996).
For PE, additional complications were catheter placement procedures, hypotension, hypocalcaemia, and allergic reactions (Ara et al., 2017; Kaya et al., 2013). For IVIG, they were a higher risk of thromboembolic complications in patients treated with a second immunoglobulin dose (Kapoor et al., 2020; Y. A. Rajabally, 2022; Y. A. Rajabally & Kearney, 2011)
Regarding mortality, in this study, there were no differences between therapies. However, Meregildo-Rodriguez and Bardales-Zuta 2021 found a tendency toward decreased mortality among PE patients (Meregildo-Rodriguez & Bardales-Zuta, 2021). On the other hand, El-Ghanem et al. 2016 reported that patients who received IVIG had decreased mortality (El-Ghanem et al., 2016). A recent systematic analysis from 2023 found that it was impossible to delineate the effect of treatment regimens on the mortality rate of GBS patients because most studies did not analyse mortality rates. (Zaki et al., 2023).
Electrophysiological findings as a secondary outcome in GBS
In the current trial, there was no significant difference in the electrophysiological findings between the two groups at baseline; nevertheless, there was a substantial improvement in the electrophysiological data three months following therapy for both groups, with significant improvement in amplitude of distal CMAP of both ulnar and posterior tibial nerve among IVIG group compared with PE. This partially agrees with the previous results reported by Kuwabara et al. 2001, who demonstrated that the CMAP sum score at six months tended to be greater for the IVIg group (Kuwabara et al., 2001).
We also observed recovery of electrophysiological responses in patients with no electrical response at baseline, although there was no significant difference between the two treatments.
From an economic point of view, PE had lower drug costs than IVIG, and since there were no significant differences between groups in terms of needing MV, number of days on MV, length of hospital stay, or complications, PE was cheaper than IVIG. This differs from the report of Tsai et al. 2007 who found that even though IVIG therapy has high drug costs, it was associated with statistically significant cost savings due to a shorter hospital stay, lower costs for procedures and hospitalisation, fewer complications, and fewer patients who need assisted MV compared to a PE group (Tsai, Wang, Liu, Sheng, & Lee, 2007).
Strengths of the study: In the present study, we used the newly proposed clinical rating scale (FAAIN-GBS) for the functional assessment of GBS, which underwent the first validation step based on a retrospective study (Lestayo O’Farrill et al., 2022). To our knowledge, the current clinical trial is the first prospective study to use it in assessing GBS. The second point of strength was the inclusion of different clinical scales (motor and functional scales) as well as electrophysiological assessment.
Limitations of the study: the first limitation is the relatively small sample size. Second, the lack of long-term electrophysiological assessment at a one-year follow-up. Third, the lack of comprehensive assessment of treatment-related complications. Finally, we were unable to assess the IgG anti-GM1 positive subgroup of GBS in the current study, as these tests are unavailable in our city.
Conclusion
The current study indicated that the final one-year outcome were equivalent. However measuring the effect sizes at one year suggested that there are measurable differences between the PE and IVIG groups with superiorty of IVIG. The time course of improvement was also slightly faster, particularly at 1 and 3 months in the IVIG group. However, Treatment with PE was less expensive.