
Abstract
BACKGROUND:
Alzheimer’s disease (AD) progressively impairs individual’s wayfinding ability. For older adults with AD, the decline of sensory acuity due to ageing and the deterioration of cognitive domains worsen their sense of direction.
OBJECTIVE:
This paper presents (1) a concept of wearable navigational assistance using haptic stimuli to help the individuals with AD for outdoor wayfinding and (2) its preliminary assessment.
METHOD:
A User-centered Design (UCD) with co-design methodology is applied through a survey that specifies the system requirements for the device. The survey is subcategorized into: (1) demographic of respondents, (2) acceptability, (3) wearability, (4) setting suitability, (5) usability, and (6) general concept. The respondents were the caregivers and clinical/medical experts of AD and dementia.
RESULTS AND DISCUSSION:
The proposed concept for the device is considered relevant mainly towards the early to moderate AD patients, due to the aspects of safety, uncomplicated functions, as well as unobtrusiveness and non-stigmatizing design features. However, this intervention should be followed by continuous practices for familiarization purpose.
CONCLUSION:
The gathered findings from this preliminary assessment encourage the implementation of a working prototype. Improved navigability allows the good performance of activities of daily living (ADLs) and maintains the good quality of life in older adults with AD.
Keywords
Introduction
The aging population increases each year and by 2050, the number of people above 65 years old is expected to be close to 2 billion [1] and cognitive impairments are expected to become a major issue. Dementia is an umbrella term describing a variety of diseases and conditions that advances when nerve cells in the brain (neurons) die or no longer function normally [2]. Among these pathologies, Alzheimer’s disease (AD) is the most common type of dementia amongst the old generation [3]. Accordingly, with the increasing aging population, the number of AD and dementia cases is simultaneously increased [4]. In parallel, although age is not the main factor of the disease, yet, most of the AD cases reside among older adults [5].
One of the most important factors that help to maintain the normal social functioning in older adults with cognitive impairments is the mobility skills [6]. It keeps the performance of activity of daily living (ADLs) and at the same time reduces the dependency. Older adults without AD remain stable in terms of their spatial navigation skills: the process of determining and maintaining trajectory from one point to another [7]. However, this crucial skill is deteriorated by AD due to the cognitive function deficits. AD often impairs individuals’ spatial cognition and representation that relate to wayfinding abilities [8, 9].
Further, older adults with AD also manifest sensory declines, similar to the healthy older adults. This problem worsens their sense of directions, as oriented search is linked with sensory – mainly the visual [10]. This wayfinding disability is usually referring to spatial disorientations, defined as the individual’s inability to orient in the environment as a result of focal brain damages [11, 12]. Conventional map and route-based navigations that rely predominantly on visual and sometimes with auditory supports may not be the best choice of modality for older adults with AD, due to these limitations.
AD also significantly affects the acceptance of peculiar things by its patients, hence limiting the possibility of intervention with technological approach, such as using the devices. This paper presents a conceptual design of a navigation device with alternative and uncommon signals i.e. haptic/tactile display to assist the wayfinding of older adults with AD. Considering the behavioral and cognitive issues caused by the disease, a co-design approach in accordance with User-centered Design (UCD) methodology [13] has been adopted to match the complications in products acceptance [14]. The initial strategy in meeting this aim was the conduction of a structured survey to gather users’ needs and requirements in proposing the appropriate technology/systems and related design aspects for the device.
Related works
Decline of spatial navigation due to ageing and AD progression
The associative factor between aging and spatial navigation is well recognized. Typically, wayfinding deficits increased exponentially with the age and the severity of the AD [12, 15]. This association is usually assessed by investigating the spatial/route navigation tasks. For instance, due to this wayfinding deficit, older adults tend to navigate only in the familiar routes or environments [16, 17], to avoid getting lost. Also, in navigating a route, older adults always took longer to reaching the target destinations and made more mistakes as compared to younger adults [18, 9].
While this is the case, spatial cognition and performance are worsened, as the cognitive domain is deteriorated in AD patients. In fact, spatial disorientation is diagnosed early in the development of AD, which is during the Mild Cognitive Impairment (MCI) stage [19]. Although not every MCI case ends up with full-blown dementia, the possibility to develop it is still high [20]. Number of studies found that adults with dementia were significantly slower in motion search tasks [21], unable to sense movement [22] and also reduced control of spatial focus [23] due to deficits in the working memory.
Sensory impairments effects the sense of direction
Older adults with AD alongside with cognitive and behavioral changes also manifest the sensory changes as they grow older. In particular, the sensory decline indirectly affects their spatial cognition and visuospatial representation that associate with the sense of direction [17]. Whilst, cognitive mapping [24] constructs the association between sensory acuity to the oriented search [25, 10].
Loss of color sensitivity and reduced depth perception and contrast sensitivity [26, 27] are the main issues in ageing vision. In the same way, older adults with or without AD usually show mild-to-moderate hearing impairment [28]. And yet, deficits in central auditory processing capacity and cognitive decline weaken the communication process [29], as well as visuospatial and auditory information in AD [30]. These sensory changes resulted in poor spatial navigation skill and wayfinding abilities in general.
Similar to vision and hearing, tactile acuity is progressively impaired due to aging [31] which contributes to the age-related impairment of sensorimotor and cognitive abilities. However, as proven by the assessment of speeded object identification task, individuals with AD maintained intact haptic priming, despite being highly impaired in recognition performances [32].
These pieces of information are feasible in designing the new devices using other sensing abilities, like haptic perception itself. This is the fundamental indication that encourages us to explore further on its unique qualities. Also, the conducted literature analysis did not elicit such an approach, which deviously certifies the innovativeness of our conceptual design.
The needs for alternative form of navigational assistances
Current navigational devices took advantage of the advance technological applications and its rapid ubiquity. The commercial map and route-based navigations that use Global Positioning System (GPS), is a very well established technique to meet the current wayfinding issues. Typically, this method of navigation supports predominantly on visual interactions and the common additional feature is the integration of auditory support, i.e. speech instructions or sound cues. Unfortunately for the older adults with AD, their most obvious sensory declines are both visions and hearings. Hence, these modalities may hinder the effective wayfinding.
The use of haptic/tactile stimulus as an output on feedback could be a good substitute to the current wayfinding method for individuals with AD, mainly due to the abovementioned limitations. In addition, since the spatial disorientation and sensory changes worsen the navigability in older adults with AD, the ideal navigational assistances should apparently be designed to support the remaining abilities.
Haptic devices (or haptic interfaces) are mechanical devices that mediate the communication between users and computers. In human-computer interaction (HCI), haptic feedback means both tactile and force feedbacks. Tactile, or touch feedback is the term applied to the sensations felt by the skin, and this feedback allows the users to feel things such as the texture of surfaces, temperature and vibration [33, 34].
Haptic/tactile-feedback for navigation
Presently, there is a growing body of research on the use of haptic/tactile modalities in the domain of mobile human computer interactions. This unique modality has been explored in a variety of applications such as the haptic-feedback system to sense of virtual objects [35], in surgical tasks [36], designing the human-computer interfaces [37], and for navigational instructions [38, 39, 40, 41]. Nonetheless, for wayfinding or navigational purposes, the existing body of works often focuses on individuals with severe visual impairment or blind people, and not specifically for the persons with cognitive impairment.
For instance, Zöllner et al. [38] conceptualized a mobile navigational assistance with Microsoft Kinect and optical marker tracking to help the indoor navigation of individuals with visual impairments. They created a belt embedded with vibrotactile outputs that were used to detect obstacles during wayfinding tasks.
Similarly, another study by Ertan et al. [39] described a wearable navigation system using haptic directional display integrated with a vest. The system gives haptic signals to the users’ back in the course of navigation. In a different study, Mann et al. [40] presented a blind navigation system with a Kinect 3D sensor range camera and a vibrotactile helmet. The vibrating actuators embedded inside the helmet convert depth information into haptic feedback, to allow the users in identifying depths for collision avoidances.
Closer to our goal is done by Grierson et al. [41] who investigated the applicability of tactile signals to assist the wayfinding of persons with dementia. In this study, they developed a wearable belt with vibrating motors. Participants were asked to navigate a series of routes within a hospital with the assistance of vibrotactile signals. This is where our design concept initiated but with a twist. We found that it is important to highlight the potentials of haptic/tactile stimuli to assist or improve the wayfinding of individuals with cognitive impairments to serve their different needs and issues.
Another essential point is most of the navigational assistances described above are the wearable technologies/devices. This is most probably because designing devices to be wearable improve the practicality of handling and operating [42, 43]. Furthermore, haptic/tactile feedback as forms of signals provides a simple, yet a promising form of directional cues that allows users to concentrate on the surrounding with other senses (vision and hearing) during wayfinding [44]. Besides, the vibrotactile signals that created the haptic simulation are less disruptive as compared to the auditory instructions, which is a suitable substitute for continuous feedback [38].
Technological interventions that utilize haptic/tactile modality to assist wayfinding have shown positive results, though most of them were meant for visually impaired and blind people. Furthermore, most of the existing wayfinding intervention strategies, which include the above-mentioned studies [38, 39, 41] focus on indoor navigation. This means, further research on navigational assistance for outdoor wayfinding purposes are highly recommended. The conceptual design that we propose employs the hybrid approach between; (1) the unique advantage of haptic/tactile, (2) device wearability, and (3) outdoor navigational strategies.
Conceptual design
The new device will use haptic stimuli as the signals, instead of reading a map display or listening to speech instruction in the course of navigation. For the maximum acceptance and integration, it is meant to be wearable in an easy invisible way. It provides the simplest possible information about the navigational instruction - left or right direction. The uncomplicated feature is crucial as to avoid distraction or confusion by the users when using this device during wayfinding tasks [38]. This is important because even a minor interference may cause misdirection to the individuals with AD. For that, the navigation device is conceptually designed to be worn as a pair on both sides of the appropriately chosen body parts.
The proposed positions to place the device are based on the recommendation by Gemperle et al. [45]. In the study, they presented the general areas (of body parts) that are most unobtrusive and suitable for wearable objects. Equally important, the built-in haptic signal will work most efficiently when it has the direct contact with users’ skins [46] hence, we proposed the integration with the clothes or underwear. Accordingly, the positions that we found appropriate for the integration are; shoulder, waist, thigh and top of the foot. Figure 1B shows these possible positions to place the device.
(A) The haptic/tactile stimuli on the wearable navigation device, with (B) the possible body part positions.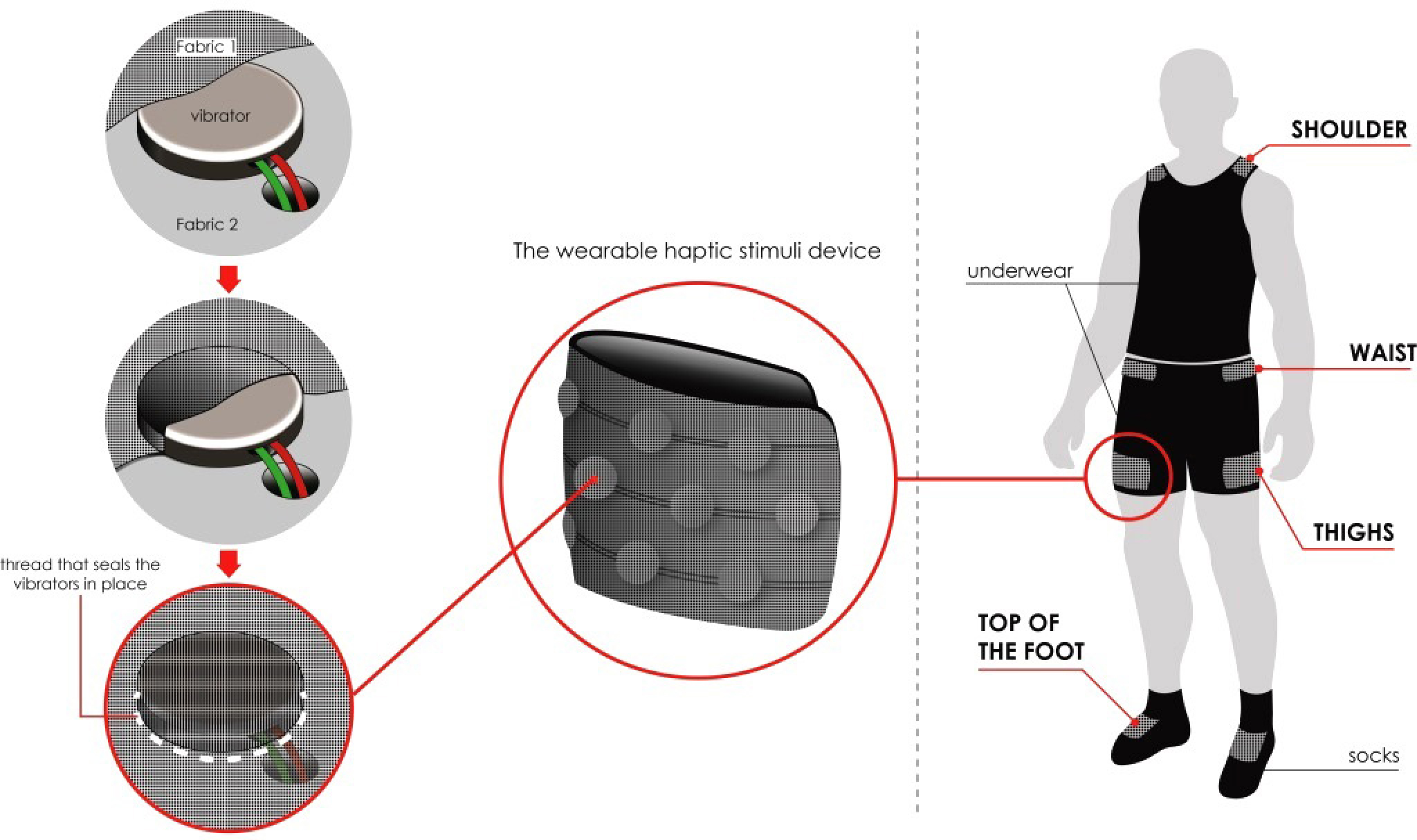
How the navigation device works (based on actual route in Milan, Italy).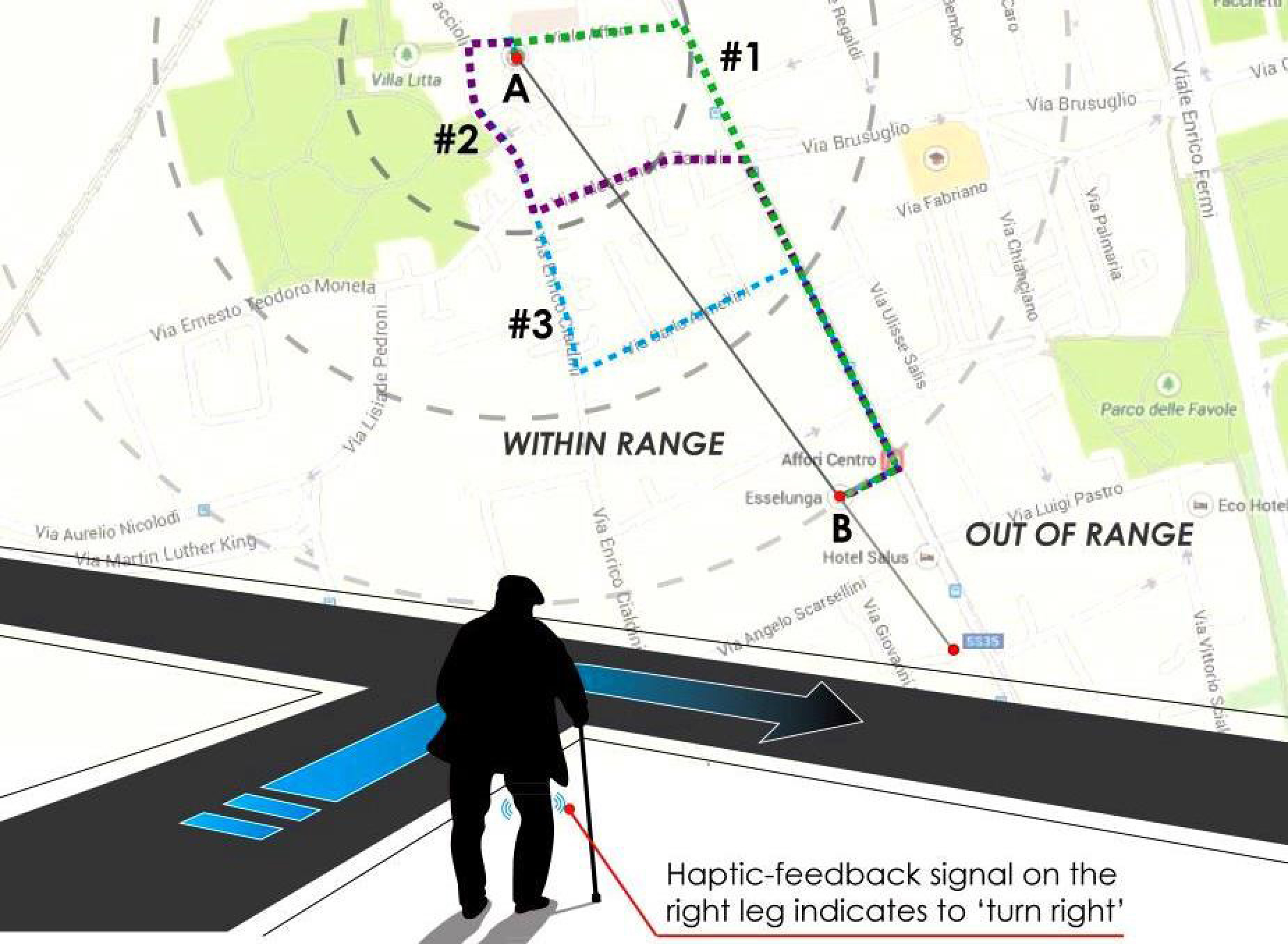
As shown in Fig. 2 that visualizes this proposed navigational concept, to go from point A (home) to point B (local supermarket), there are three routes the user can follow; #1 (Option 1), #2 (Option 2), and #3 (Option 3). In initiating the journey from point A, one may turn left or right and the haptic signals embedded in the system will start immediately. If he/she turns right, #1 will be the choice of route, whereas left is for #2 or #3. In order to go back from B to A, the signal will initiate as soon as the user got out of the place (B), and direct him/her into the correct route (#1, #2 or #3). During wayfinding, the users need to travel within the estimated range. However (in some inevitable cases), if they happen to accidently go beyond the range, a stronger signal will start immediately to guide them into the correct path.
The participatory or co-design approach [13] from the UCD method allows us to properly define the technical and aesthetical characteristic, as well as functionalities and plausible solutions to be implemented for the proposed device design. Based on its principle, this approach aims to include every stakeholder into the design and development process in achieving their necessities [47].
Method and participants
A survey was conducted as a preliminary assessment to investigate the feasibility of the design concept in terms of: (1) acceptability of intervention, (2) usability on users, (3) wearability of the device, and (4) setting suitability of interventions. There are several strategies to assess a design though the inclusion of users in the design and development process as suggested by [48]. Accordingly, background interviews and questionnaires are usually conducted at the beginning of the design project to obtain data associated to the needs and expectations of users. Meanwhile, although this intervention concerns individuals with AD, attaining feedbacks from them could be insubstantial because this survey requires a clear justification of preferences and definite reasoning. Thus, the target respondents of the survey were; (1) caregivers and (2) clinical/medical experts of AD and dementia.
We postulate that these respondents could be the best communication mediators and information pro- viders who represent AD patients for the questions and issues related to dementia in general. This is because, they recognize the distinctive behavioral and cognitive changes of the AD patients and have the most knowledge base about patients’ caregiving need [45].
In addition, the ethical issues related to the appropriateness of this proposed intervention towards the target users have been adequately considered before we administered the survey. This ethical consideration was initiated with the advice from dementia experts we are currently working with. For this reason, there was no need for the questions related to the ethical issues for this particular assessment. However, in the future and with an extended population that includes the participation of AD subjects, this matter will certainly be taken into account.
The survey was distributed online to the selected AD and dementia institutions in the United Kingdom, Italy and Malaysia based on the availability, recommendations and the established networking. It was made of both close-ended and open-ended questions, but the respondents could also add their additional comments where necessary. Before the questions began, we provided the detailed description of the proposed navigational assistance concept. Here, we explained the approach and reason of the choice of a haptic system through the drawings as previously presented in the Conceptual Design section. We supposed that the description was necessary since the proposed concept is unlike the ordinary or existing navigational devices. The description also explains the technical terms used that might not be familiar by the respondents. At the end of the questionnaire but before the completion of this assessment, the respondents were asked to state their full understanding of the proposed concept based on their general technological knowledge.
In order to justify the specific objectives of this preliminary assessment, the questions are subcategorized into six segments; (1) demographic of respondents, (2) acceptability, (3) wearability, (4) setting suitability, (5) usability, and (6) general concept. Table 1 shows these segments and its questions, as well as the scores and the descriptive analysis.
Survey analysis on the acceptability, wearability, setting suitability and usability of haptic-feedback navigational device for individuals with Alzheimer’s disease (AD)
Survey analysis on the acceptability, wearability, setting suitability and usability of haptic-feedback navigational device for individuals with Alzheimer’s disease (AD)
Forty two respondents (
According to the UCD principles, we considered that even the AD patients are the primary users of the device, but the overall intervention – in assisting the wayfinding of persons with dementia, includes a bigger stakeholder structure that comprises of patients’ caregivers, family members, nursing homes staffs and managers etc. Everyone who directly or indirectly involves has an active role in the device use and its management. However, even if the collected data had polarized initial results, the assessment on real users (AD patients) by means of Usability Testing will be performed soon after the development of the functioning prototype. Results presented in the next section comprehend both answers to closed questions and open comments.
The importance to identify if the proposed conceptual design of navigational assistance is acceptable by the users (persons with AD) is highly appropriate. In fact, it is one of the primary concerns of the investigation, before the design concept may be forwarded into the next stages; prototyping, usability testing and implementation. Specifically for this segment, we need to understand how the new proposed navigational assistance is received by the users, positively or negatively. As previously mentioned, none of the persons with AD took part in this preliminary assessment, since they might not be able to clearly opinionate their perceived views. Having said this, the feedbacks from the caregivers and the AD experts are already a convincing dataset and may determine the success of this proposal in its initial stage.
Firstly, we asked if the persons with AD would use this new navigational device as well as if they can cope with the continuous use to get familiarized with the concept, since it is a new form of navigational assistance. The quantitative data confidently shows that the respondents received the proposal well, with most of the respondents agreed that this concept is practical to be used by the target users.
The following questions directly looked into the ‘acceptability’ of this proposed design concept. Once again, most of the respondents (62.3%) rated acceptable and only 4.8% rated highly unacceptable. The further qualitative analysis show that the high percentage of acceptance might be due to the proposed concept provides the uncomplicated features. The simple features are clearly meant to minimize their confusion caused by the spatial disorientation and navigational disabilities, especially during the complex wayfinding tasks.
In terms of wearability, the respondents were first required to choose the most preferred positions to place the device or to trigger the haptic/tactile stimuli. The body-part positions are based on suggestions by Gemperle [45], and with possible integration on underwear. Results show that both waist and shoulder shared the same highest score (26.2%), while thighs and other positions were the least favored (9.5% and 16.7% respectively).
In this segment, respondents were also asked to rate (on the scale of 1 to 5, with 1 represents the minimum score of agreement and 5 for the maximum) if it is appropriate to integrate or attach the device onto users’ clothes or underwear. This is purposely for the practicality of use, as previously discussed. Positive feedbacks were gathered for this specific question, with 31.0% of the respondents rated 4/5 and 26.2% rated 5/5. Results indicate the possibility to explore more on the wearable aspect of the navigational device. From the proposed clothes or underwear, respondents mostly preferred the singlet (35.7%) and secondly the briefs (26.2%) to be integrated or attached with the device. These selections validate the most preferred body-part positions as justified earlier – singlet is suitable for shoulder, while the brief is appropriate for waist-length and abdominal area.
From the usability viewpoint, the respondents were required to rate (using the same scale of 1 to 5) the unhelpfulness/helpfulness of the proposed concept of navigation. Most of them (62.3%) rated the device as ‘helpful’ which indicates its usefulness for wayfinding. Next, they were asked if they preferred the navigational assistance to be a standalone device. Standalone here means the device works on its own without the integration of another device, such as mobile phone. For this, the majority (45.2%) approved the concept of standalone device.
However, when they were asked if additional features such as visual and auditory instructions were needed, 42.9% were unsure of this, and 33.3% prefer the additional features. The following question rectified this disagreement. Accordingly, given the choices of additional modalities: [1] speech instruction, [2] visual instruction, and [3] both speech and visual instructions, mostly agreed that the essential additional features to the device are; speech instructions (40.5%) and both speech and visual instructions (also 40.5%).
In terms of environmental setting suitability, the majority agreed that this intervention strategy is best to be implemented mainly in an outdoor environment. Again, from the scale of 1 to 5, 35.7% rated 4/5 and 33.3% rated 5/5. For the outdoor wayfinding purposes, respondents agreed that the proposed device is useful to facilitate the users to navigate; (1) to the nearest parks, markets, hospitals, etc., (2) to use the public transportations, and (3) socializing inside community. Thus, as many other outdoor wayfinding interventions [49, 50, 51], the data suggest that the respondents approved that this outdoor navigation device is more appropriate to be used within the neighborhoods they live in.
Furthermore, most of the respondents recommended that the users should not be allowed to travel alone too far with any navigational assistance devices. Given the proposed range of allowed travel distances, 31.0% chose less than 1 km, 26.2% chose the range of 2 to 4 km, 23.8% preferred 5 to 6 km, and none of them chose the longer range of distance (above 7 km). The preferred short distance is appropriate for the users’ safety, by means of reducing their risk being in an open space unattended for a long period of time. This is therefore justified that the proposed device should be designed to be used within their neighborhood that only involves the normal daily routines/activities and covers not so wide travel range (between 1 to 4 km).
There are some important concerns raised from the further analysis of the corresponding qualitative data. These concerns are important to be considered to improve the proposed design concept. In terms of its functionality, even the quantitative analysis positively demonstrated that the device is acceptable and practical to be used, introducing a new form of navigational assistance itself could be a challenge especially for the target users; AD patients. However in this case, the qualitative analysis suggests that if the issues of familiarity and training can be resolved, the proposed concept can be successfully implemented. Here, many of the respondents recommended to provide a manual in a simple lay language to the caregivers and therapists, who will get familiarized with the device before they can train the real users.
Another important point is the design of the wearable device itself. The selection of suitable materials to be used for the wearable device should consider the appropriateness of long hours of use, as well as of different environmental and contextual climates. Here, comfortability and unobtrusive are the key criteria to be considered. This is to avoid the post-implementation issues faced by the users, possibly due to the skin sensitivity and differential climate conditions. In addition, giving a discreet look at the design is crucial because the too noticeable device may cause discomfort and stigmatizing to the users.
Proposed system architecture for the wearable device.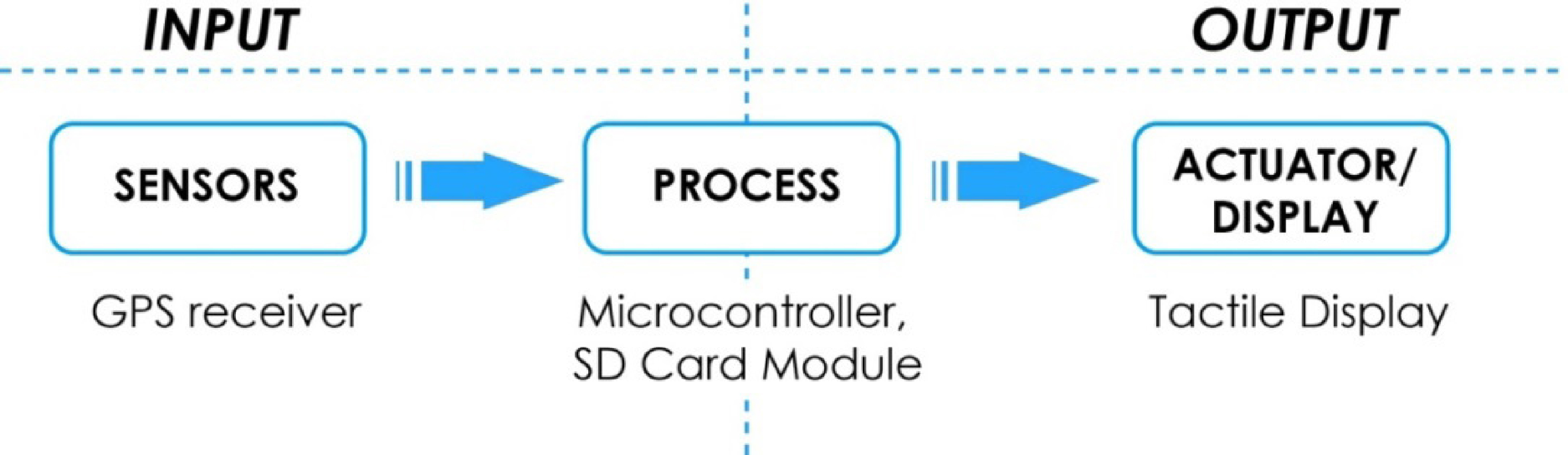
Finally, as many of them agreed, this intervention should be targeting to the individuals in the early stage of cognitive impairment. The level of consciousness and cognitive function in AD patients are worsen as the disease progresses [52, 2], which affect their spatial disorientation and the ability to navigate simultaneously [7, 11]. This specific concern is raised because those in the severe stage might not be able to perceive the haptic stimuli as forms of wayfinding signals. This apparently approved one of the main research objectives, which is to provide a navigational assistance to the AD patients who are not yet institutionalized. Typically, persons with AD who still live at home are in the early to moderate stage of the disease [53].
From all the above results, we may suggest that the respondents found the device relevant to be implemented towards the persons with AD based on three main reasons: (1) the safety aspect when the patients wearing/using it is ensured, (2) its simple functionality that applies to individuals in both early and moderate stages of AD and MCI, and (3) its unobtrusiveness and non-stigmatizing aspects that could augment a high acceptance by the users.
Spatial navigation skill is related to mobility and autonomy. The improved navigation skill allows the persons with AD to perform and maintain their activities of daily living. This will at the end result in keeping their good Quality of Life (QoL). In general, the results of this preliminary assessment demonstrate the positive feedbacks on the overall concept and suggest that this intervention is practical to be used by the target users and the concept has a great potential to be implemented in real-world applications pragmatically.
However, the assessment also suggests that the practicality of using solely haptic stimuli for the navigational modality by individuals with AD should be further examined and its feasibility is still need to be measured quantitatively. Therefore, another assessment - Usability testing will be carried out soon using a functioning prototype. Then again, several modifications on the design concept will be made based on the results of this preliminary assessment before the first prototype can be developed and assessed.
The working prototype is still under construction because the design concept was still in its initial stage. However, the system should support its main functionality or features as the design concept proposes. The device consists of (1) the input: GPS receiver, acceleration sensor, and Secure Digital (SD) card module and (2) the output: haptic or tactile display made of vibrators. Figure 3 illustrates the proposed system architecture for the device.
Technically, the sensors (GPS and accelerator) are used to detect users’ location information that comprises of; (1) the real time location and orientation, (2) starting point and the destination, and (3) several possible routes (from Fig. 2) that are saved in the SD card. An Arduino microcontroller is used to control the hardware and process these provided information. The device is designed be standalone without any integration of mobile application or any visual display, since it is meant to emphasize the alternative modality for navigation, i.e. the haptic/tactile stimuli.
When the users navigate on the saved routes, the microcontroller uses the input data from the sensors to trigger the vibrators. The information on the several positions where vibrators should be triggered is also saved in the SD card. These positions are mostly located on the junctions and corners where the users need to turn left/right to reach the designated destination. The haptic stimuli are created with multiple mini vibration motors or vibrators at regular intervals of mean threshold (20 mm to 50 mm) according to body positions [45]. These series of vibrators will be embedded between the two layers of fabrics and sealed together using threads, as shown in Fig. 1A.
Since there is a dearth in outdoor wayfinding strategies especially for the people with cognitive impairment, we hope that our proposed conceptual design of wearable navigational assistance may fill the gap. This navigational device is expected to improve the navigability of older adults with AD, mainly in an outdoor environment. Then again, as implicit memory for haptically-explored objects is preserved in those with mild AD [13, 31], only continuous practice gives an encouraging result. Therefore, before the development of a functioning prototype, it is necessary to understand the potential of this conceptual design from the perspectives of the (AD and dementia) experts in its initial stage. This was indeed justified through this preliminary assessment.
Footnotes
Acknowledgments
This work was supported by the collaboration between Laboratory of Innovation and Research about Interior (Lab.I.R.Int) and Biomedical Sensors and Systems Lab (Sensibilab) from the Department of Design, Polytechnic University of Milan, Italy.
Conflict of interest
None to report.