
Abstract
BACKGROUND:
To avoid falls in older adults, current solution is compensation using mobility aids.
OBJECTIVE:
Evaluating satisfaction of older adults with follow-up from their general practitioner and physiotherapist regarding their mobility aid.
METHODS:
A telephone survey was carried using a satisfaction questionnaire in 86 patients aged 87
RESULTS:
Participants were satisfied with the follow-up from their general practitioner (78%) and their physiotherapist (93%) regarding their mobility aid. They judged the professionals competent, respectively 52% and 62%. Less than 50% of participants reported receiving advice and encouragement from the professionals regarding their mobility aid. The physiotherapist was preferred to the general practitioner regarding follow-up for the mobility aid. Follow-up of the professionals did not influence any change in mobility aid, which the patients determined themselves in two-thirds of cases.
CONCLUSIONS:
Participants were satisfied with the follow-up by the general practitioner and physiotherapist regarding mobility aids, nevertheless, their follow-up demands of professionals, were superficial as they did not truly use them as resources. General Practitioners, physiotherapists and relatives’ help have to communicate with each other to properly influence changes of mobility aid in elderly people at home.
Introduction
Falls are a common problem for older adults, occurring in 32% and 42% of people aged 70 years or older [1]. Falls can have serious consequences. Forty percent of falls require hospitalisation and falls are associated with a high death rate [1, 2]. The risk factors for falls are well identified and include mobility and balance deficits. Sixty percent of those above the age of 80 years report having walking problems and 20% of older adults report having disabling balance problems [3, 4].
Effective fall prevention programs in elderly subjects are multifactorial and include assistive technology [5]. There are not always available medical or surgical treatments for walking and balance disorders thus the only current solution is compensation using mobility aids to avoid the fall. Eleven percent of French people above the age of 60 years use a walking stick and 1.2% use a walker [6]. The choice of mobility aid is based on patient-centred criteria such as strength, balance, coordination, sensory function, cognitive state and environment [7, 8]. Studies agree that the choice must be based on each individual’s clinical context and the experience of a health professional [9]. A systematic review of 8 studies showed a positive effect of mobility aids on activities of daily living and quality of life of older users [10].
Many studies have evaluated compliance with the use of mobility aids at home by older subjects, and have found that around 60% of those who do not use their walking stick, 35% who do not use their walker and 50% who use their aid badly, have all an increased risk of falling due to their poor compliance [11, 12].
Non-use, as well as poor use, of mobility aids may result from a lack of follow-up care and patient dissatisfaction with the mobility aid [13, 14, 15, 16, 17]. Many studies have evaluated patient satisfaction with mobility aids but few have evaluated satisfaction with the follow-up received from professionals regarding use of the aid [16, 18, 19]. Moreover, in practice, the mobility aid is often prescribed during hospitalisation in a geriatric ward, but no follow-up by the hospital is provided once the patient is discharged home. The aim of this study was to evaluate the satisfaction of older adults with the home follow-up visits by their general practitioner and physiotherapist with regard to their mobility aid following discharge from a geriatric rehabilitation ward.
Materials and methods
Design
This was a prospective, questionnaire-based satisfaction survey carried out from the 17th of April 2015 to the 17th of October 2015. The survey was carried out by a single investigator by means of a telephone interview 3 months’ post-discharge from geriatric rehabilitation. Either the patient or a carer if the patient could not respond, was interviewed. If there was no reply to the first call 3 months’ post discharge, the call was repeated every week for a month.
Participants
Patients were recruited from the 17th January 2015 to 17th July 2015 from the ortho-geriatric rehabilitation department of Hôpital Charles Foix, part of the Groupe Hospitalier Pitié Salpêtrière-Charles Foix, Assistance Publique-Hôpitaux de Paris (APHP). This department admits patients with recent fractures, particularly proximal femoral fractures (PFF), for multidisciplinary rehabilitation. The department is situated at Ivry-sur-Seine, in the Val-de-Marne region of France. Patients were included if they were 75 years or older and being discharged to their home, and with an Mini Mental State Examination score
Flow chart of participation in study. PFF: Proximal femoral fracture.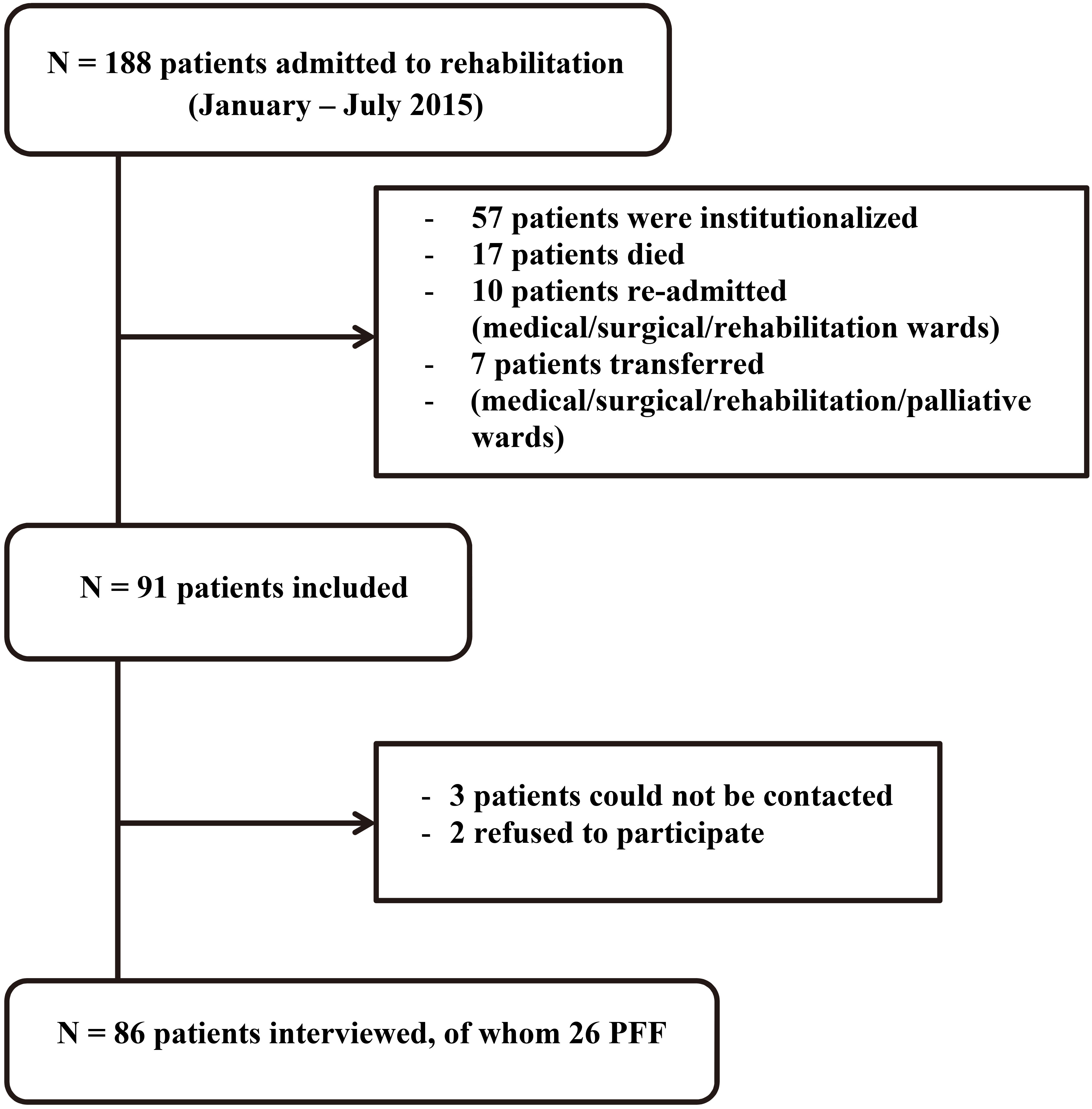
The interview questionnaire (Appendice), on which the telephone interviews were based, was developed with the department rehabilitation professionals: occupational therapist, physiotherapist and psychomotor therapist, regarding home-management of mobility aids. The first version was submitted to 5 voluntary patients during their stay in the department. Their feedback was taken into account for the final version. Two versions were designed: one for patients and one for carers. The content of these versions was identical, simply the formulation of the questions varied. Whenever possible, the patient was interviewed and only if this was impossible, was the carer interviewed. The questionnaire consisted of 3 parts: the first evaluated use of the mobility aid at home, the second the patient’s satisfaction with the mobility aid follow-up mobility by their general practitioner, and the third, which was similar to the second, assessed satisfaction with mobility aid follow-up mobility by the out-patient physiotherapist. The questionnaire consisted of 9 closed, multiple-choice questions, 29 binary response questions, 2 open-ended questions and 3 based on a Likert-type scale for satisfaction rated from 1–5 (1
Data analysis
Descriptive analyses (means and standard deviations for quantitative data, and numbers and percentages for qualitative data), were carried for satisfaction with follow-up for mobility aid by the general practitioner and physiotherapist. Sub-group analyses were carried out for participants with proximal femoral fractures, the most prevalent medical condition.
We compared satisfaction with home follow-up by the general practitioner and the physiotherapist, using a McNemar test for paired data, since some participants had both a general practitioner and a physiotherapist and answered both satisfaction questionnaires. In order to identify predictive factors of change in mobility aid during the 3 months, univariate analyses were performed with Chi2 test for qualitative data and a Wilcoxon test for quantitative data. Then, a multivariable logistic regression model was used, according to a forward stepwise strategy. For all analyses, bilateral tests were carried out with an alpha risk of 0.05. All analyses were conducted with Microsoft Excel 2007 and SAS statistical software, version 9.3.
Ethics
The study was declared to the French Data Protection Authority (Commission Nationale Informatique et Libertés), declaration number: 1547216, date 24.11.2011. All data were anonymised for analysis.
Results
Sample characteristics
One hundred eighty-eight patients were admitted to the department during the 6 month study-period (Fig. 1). Of these, 57 (30%) were institutionalised, 17 (9%) deceased, 7 (4%) were transferred to another department, 10 (5%) were re-admitted and 6 (3%) were bedridden, thus excluded. Among the 91 subjects included, 3 could not be reached by telephone, despite re-attempts, and 2 refused to participate in the survey citing mistrust or complaints following their stay in rehabilitation. In total, 86 (45.7%) patients, of whom 26 had proximal femoral fractures, participated in the telephone survey.
Respondents were mostly female (78%), aged 87
Satisfaction with follow-up for the mobility aid by the general practitioner
Ninety-four percent of participants consulted their general practitioner within the 3 months following hospitalisation, of whom 62% were seen at home. Sixty-five percent considered their relationship with their general practitioner as “quite good” or “very good”. During the interviews, 94% of participants reported never seeking advice regarding the use of their mobility aid since they returned home either because they did not think it was necessary (63%), because they could not get a convenient appointment (14%), because it was felt that the general practitioner would not know (16%), or for no reason (7%). Forty-two percent said that they had been encouraged by their doctor to use their mobility aid. Only 21% said they had received advice from their general practitioner regarding the mobility aid unprompted. Sixty percent considered their general practitioner to be interested in their mobility and 78% of patients were “quite satisfied” or “very satisfied” with the follow-up received from their general practitioner regarding their mobility aid.
Satisfaction with the mobility aid follow-up support from the physiotherapist
Seventy-three percent of patients reported having received physiotherapy during the 3 months post-discharge from rehabilitation, 90% of which was at home. Of the 27% who did not receive physiotherapy, this was reported to be due either to the fact the patients had not contacted the physiotherapist and did not consider it necessary (
General practitioner or physiotherapist?
Participants consulted their general practitioners more often than their physiotherapists during the 3 months following discharge. Participants reported feeling more encouraged and guided by the physiotherapist than by the general practitioner. Physiotherapists were considered to be more competent than general practitioners regarding the mobility aid. Overall, participants were more satisfied with their physiotherapist than their general practitioner regarding the follow-up they received about their mobility aid (Table 1).
Satisfaction with follow-up for the mobility aid by the general practitioner and physiotherapist
Satisfaction with follow-up for the mobility aid by the general practitioner and physiotherapist
Results are expressed as
Predictive factors of change in mobility aid during the 3 months post discharge home from rehabilitation (
In 70% of cases, changes in mobility aid were de- cided entirely by the participant, more rarely at the suggestion of the general practitioner (14%) or the physiotherapist (7%). Several factors were related to the change in mobility aid: being female, being discharged with a walker, a long stay in rehabilitation, and having outpatient physiotherapy. In contrast, being discharged with no mobility aid or a walking stick and receiving advice from the general practitioner reduced the probability of changing mobility aid at 3 months (Table 2).
In the multivariate analysis, professional interventions were no longer found to have influenced the change in mobility aid at 3 months, the only factor that influenced this change was having been discharged with a walker (OR
Of the 26 patients admitted for proximal femoral fracture, if the mobility aid was considered suitable for use in the patient’s home and the patient had received advice from the physiotherapist, there was reduced change in mobility aid at 3 months (Table 3).
Predictive factors of change in mobility aid during the 3 months post discharge home from rehabilitation in patients with proximal femoral fracture (
26)
Predictive factors of change in mobility aid during the 3 months post discharge home from rehabilitation in patients with proximal femoral fracture (
Multivariate analysis was not carried out for this sub-group because the number of participants was too small.
The first impression of the results of this survey suggested home follow-up of the mobility aid was satisfactory, both quantitatively and qualitatively. Almost all patients consulted their general practitioner during the 3 months post-discharge and 73% underwent outpatient physiotherapy at their home. These were good results which indicated that this population received privileged regarding home care. Indeed, the Paris region has the highest regional density of medical practitioners and a density of physiotherapists of 141 for 100 000 inhabitants compared with 92 nationally [20, 21]. There satisfactory follow-up data were in accordance with the recommendations of the French Health Authority regarding the post-discharge period in older adults, which specify that outpatient interventions should be provided following discharge home [22]. The quality of the follow-up support was also judged to be good, as over three-quarters of participants reported an overall, satisfaction with the advice they received during home visits from their GP and physiotherapist regarding their mobility aid. The professionals were considered competent in this domain. This was important since falls prevention programs recommend teaching the correct use of mobility aids such as walking sticks and walkers [12, 23]. However, other studies of follow-up have suggested that patients are generally dissatisfied and find home support to be insufficient [13, 14, 24]. This difference may be explained by the fact that the majority of participants in the present study used their mobility aid (79%), which implied that they were satisfied with it, which facilitated satisfaction with the associated follow-up, but also by the fact that different procedures exist depending on the country. The percentage of mobility aid usage was higher in the current study than in other studies. For example, 60% of older, Danish subjects living at home and 50% of English subjects over the age of 75 years living at home used their mobility aids [11, 13]. The present result was also much higher than that found in an Australian study of patients over the age of 70 years 6 months post discharge home from orthopaedic rehabilitation in Australia. Only 56% used the mobility aid that they had used prior to their surgery [25]. The “good” usage observed in the present study could be related to the 3 month time interval chosen for the survey. Patients were still in the early post-hospitalisation phase and thus still required their mobility aid since they had not fully recovered their independence, particularly the sub-group of participants with proximal femoral fractures. The results regarding use of the mobility aid could also be attributed individuals self-reporting, at distance by telephone interview. Responses may have depended on the perception and judgement and cognitive state of the participant, in contrast with other studies that were based on face-to-face interviews in the patients’ homes, or on evaluation by physiotherapists or occupational therapists [11, 25]. We believe that the high level of participation in the survey (only 2 refusals) and the high level of interest in the study noted by the investigators from both patients and carers interviewed also act as indirect indicators of satisfaction. Nevertheless, despite the appearance of an overall satisfaction with the mobility aid support received, we considered that this first impression was deceptive. The participants may have been satisfied overall by the follow-up care received from general practitioners and physiotherapists, but this actually reflects the low-level of exigency demanded in terms of follow-up care quality. Participants reported being “quite satisfied” or “very satisfied” with professionals, despite the fact that during the 3 months post discharge less than 50% reported having actually received advice regarding their mobility aid. Furthermore, over half of the respondents said that they received no encouragement from their general practitioner and over one-third said the same of their physiotherapist. The participants did not report asking for professional advice to ensure that they were using their mobility aid correctly. Less than 10% of participants said that they had sought advice from professionals regarding their mobility aids during the 3 months following their return home. The quantity of exchanges between participants and professionals thus appeared to be low, and the follow-up for the mobility aids dissatisfactory, despite the global satisfaction of the participants. This low-level of patient demands and expectations, and the reported infrequency of advice-seeking (because they did not feel it to be necessary), suggested that participants wished to be the main decision makers regarding their mobility aid, even if they were convinced of the professionals’ competencies. They seemed to wish to express their freedom of choice, determining their own mobility needs without external advice. About two-thirds (70%) of participants changed mobility aid on their own initiative, as previously observed in other studies [25, 26]. In the present study, professional intervention did not influence the change in mobility aid, except for those with proximal femoral fracture who changed based on advice of the physiotherapist; however such advice was inconsistent, reported by only 45% of participants. The study by Thomas et al. found that the change determined by the patient was totally inappropriate in 32% of cases, underlining the correlation between an early change in mobility aid post-discharge, poor use of the mobility aid and the risk of further falls, whether the change was appropriate or not [25]. It was not the aim of the present study to evaluate the appropriateness of the change decided by the patient and we did not have the means to do so. It is not possible to determine how appropriate (including consideration of medical state and level of independence) subjective judgements by the patients were. With regard to the risk of patients inappropriately changing mobility aid, studies recommend close, regular, follow-up with regularly re-evaluation of the use of the mobility aid at home and appropriate adjustments [11, 13, 17, 26]. Other than the general practitioner and physiotherapists, participants reported seeking the advice of their relatives (family and friends) (
Lastly, the results of the survey showed that patients were more satisfied with their physiotherapist than their general practitioner regarding their mobility aid. The physiotherapist was preferred and provided more advice, encouragement, interest, and was perceived as more competent than the general practitioner. The physiotherapist was probably considered as specialised in functional rehabilitation whereas the general practitioner is often considered as simply prescribing physiotherapy. It is true that French medical training includes very little regarding mobility aids. However, despite the more favourable opinion of the physiotherapist, the general practitioner had a greater influence regarding change in mobility aid, with 14% and 7% of changes influenced by the general practitioner and physiotherapist respectively. The fact that the patient considered the doctor as having the sole right to prescribe a mobility aid could explain this result which contrasted with the patients’ opinion of quality of follow-up. At the time of writing, the physiotherapist charter states that they can prescribe mobility aids [27]. It thus seems important to improve communication between general practitioners and outpatient physiotherapists regarding the follow-up of older patients.
Very old persons with multi-pathologies and loss of autonomy were globally satisfied with the post-discharge follow-up by their general practitioner and outpatient physiotherapist, with a preference for the latter. However, participants were satisfied because they had low demands regarding their needs, and only rarely sought advice from professionals regarding their mobility aid. Although patients appreciated the follow-up, it did not influence the decision to change mobility aid, which they made themselves. There was a risk of misuse of the mobility aid and of falls. Despite the fact participants recognised the competencies of their general practitioner and physiotherapist, they more often turned to their relatives, suggesting professionals should work together with relatives. Similarly, as for hearing and vision, it is necessary to inform patients and their relatives that mobility is a dynamic physiological process that is altered by aging and certain pathologies, leading to a risk of falls. However, gait deficits can be compensated by mobility aids and professional advice. With regard to professionals, initial training and continued professional training should focus more on mobility aids. In the near future, progress in robotic aids, including intelligent mobility aids, will revolutionise the management of gait and balance problems. Professionals will need to be competent in the use of these new aids to optimise their use.
Footnotes
Acknowledgments
The authors would like to thank the rehabilitation team at SSR Gérontologie I in Hôpital Charles Foix. The authors thank M. Tawileh, MD, for English editing and revision.
Conflict of interest
None.
Appendix
Patient questionnaire
Which mobility aid(s) to you currently have at home?
Walking stick Walker with 2 front wheels Walker with 4 wheels (rollator) Walker with no wheels None Other, specify: … If 2 or more mobility aids: Which do you consider to be your main mobility aid? (for the following questions will use the term main mobility aid for the questions)
Do you use your main mobility aid? (y/n)
If YES (reply then go to Q3/)
Where do you use it? – indoors? (y/n) – outdoors? (y/n) How often?
often: every day regularly: 1–3 times per week rarely: only for certain occasions Is it the same mobility aid you had when you were discharged from the rehabilitation department of Hôpital Charles Foix? (y/n) (if yes, please go to Q3)
If NO: who suggested/requested the change of mobility aid?
yourself someone close to you (family/friend) your General Practitioner (GP) your physiotherapist a professional carer someone else, specify: ? why did you change mobility aid?
you were no longer satisfied with it you felt you no longer needed it it was defective you were offered another one which was considered to be better other reason, specify: … If NO, why do you no longer use your main mobility aid?
you are no longer satisfied with it? you feel you no longer needed it it is defective other reason, specify: … Do you feel that your main mobility aid is adapted for your home? (y/n) Do you remember having received advice regarding use of your mobility aid from therapists at the Hôpital Charles Foix rehabilitation department? (y/n) If YES: Do you feel that the advice from the hospital therapists regarding your mobility aid were useful to you when you returned home? (y/n) Would you say that you were: not at all/fairly/ more or less/quite/very satisfied with the care you received from the therapists during your stay at Hôpital Charles Foix? (scale 1-2-3-4-5) Have you consulted your GP since your discharge from the rehabilitation department of Hôpital Charles Foix? (y/n)
IF YES (reply then go to Q16/) – at home? (y/n) – in the medical practice? (y/n) IF NO, why? (reply then go to Q19/)
you did not manage to contact your GP you contacted your GP but he/she was not available you did not contact your GP because you did not feel it necessary other reason, specify: … Overall, how would you describe your relationship with your GP: not/fairly/more or less/quite/ very satisfactory? (scale 1-2-3-4-5) With regard to the use of your main mobility aid since your return home, have you contacted your GP:
to adjust your main mobility aid? (y/n) to better understand how to use your main mobility aid? (y/n) because of undesirable effects caused by your main mobility aid? (y/n) because you would like to change your type of main mobility aid? (y/n) because you would like to stop using your main mobility aid? (y/n) other reason, specify: … If you did not consult your GP regarding the use of your main mobility aid since your return home, why?
you have not seen your GP since your return home you feel that your GP lacks availability regarding your mobility aid
you think that your GP would not know you did not feel it necessary to ask your GP you do not know why other reaon, specify: … Did your GP encourage you to use your main mobility aid since your return home? (y/n) Has your GP given you spontaneous advice regarding the use of your main mobility aid since your return home? (y/n) Do you think your GP has the competencies/knowledge necessary to advise you regarding your main mobility aid and its use? (y/n) Do you think your GP is interested in your mobility/in your mobility? (y/n) Would you say you are: not/little/more or less/ quite/very satisfied with the follow-up you have received from your GP regarding your main mobility aid and its use? (scale1-2-3-4-5) Have you had any physiotherapy since your discharge from the Hôpital Charles Foix rehabilitation department?
If YES (reply then go to Q 28/) – at home? (y/n) – in an outpatient clinic? (y/n) If NO, why? (reply then go to the end of the questionnaire)
you did not manage to contact a physiotherapist you managed to contact a physiotherapist by the/she was not available (either for a home visit or in the clinic) you managed to contact the physiotherapist but he/she does not do home visits you did not contact a physiotherapist because you did not feel it was necessary other reason, specify: … With regard to the use of your main mobility aid since your return home, did you consult your physiotherapist:
to adjust your main mobility aid? (y/n) to better understand how to use your main mobility aid? (y/n) because of undesirable effects caused by your main mobility aid? (y/n) because you would like to change your type of main mobility aid? (y/n) because you would like to stop using your main mobility aid? (y/n) other reason, specify: … If you did not consult your physiotherapist regarding the use of your main mobility aid since your return home, why?
you feel that your physiotherapist lacks availability regarding your mobility aid
you think that your physiotherapist would not know you did not feel it necessary to ask your physiotherapist you do not know why other reason, specify: … Did your physiotherapist encourage you to use your main mobility aid since your return home? (y/n) Has your physiotherapist given you spontaneous advice regarding the use of your main mobility aid since your return home? (y/n) Do you think your GP has the competencies/knowledge necessary to advise you regarding your main mobility aid and its use? (y/n) Would you say you are: not at all/fairly/more or less/quite/very satisfied with the follow-up you have received from your GP regarding your main mobility aid and its use? (scale1-2-3-4-5) With regards to your main mobility aid and its use since your return home, have you consulted:
Someone close to you: family, friends, neighbour Your carer Your home help Your sports instructor Your pharmacist Your nurse Your psychomotor therapist Your occupational therapist Your medical equipment retailer Other person, specify: … Nobody