
Abstract
BACKGROUND:
Four hemiplegia post-stroke patients with 10
OBJECTIVE:
1) To investigate the optimum inclination in a Rigid Tuned Ankle Foot Orthosis (RT-AFO) in order to stabilize stance knee kinematics in the sagittal plane for stroke patients with 10
METHODS:
Three dimensional gait measurements were performed in five conditions for four participants: walk without AFO (T1), walk with RT-AFO in 0
RESULT:
Application of tibial inclination in the AFO reduced the genu recurvatum in participants who experienced stroke. Genu recurvatum was significantly reduced in conditions T3, T4 (
CONCLUSION:
These results highlight the potential to optimize inclination of a Rigid Tuned Ankle Foot Orthosis for patients affected by stroke and also indicate the potential clinical applications of tuning the AFO in rehabilitation treatment of stroke patients.
Introduction
Stroke is one of the leading causes of adult disability in many countries including Thailand. In Indonesia, the prevalence of stroke is 0.0017% in rural Indonesia, 0.022% in urban Indonesia, 0.5% among urban Jakarta adults, and 0.8% overall [1]. In Vietnam, the prevalence of stroke is 415 out of every 100,000 people; in Sri Lanka, the prevalence of stroke is 9 per 1,000 people [2], and in Bangladesh the prevalence of stroke is 3 per 1,000 [3]. Meanwhile in Thailand the prevalence of stroke is estimated to be 1.88% among adults 45 years and older [4]. One of the negative effects of stroke is impaired mobility; only 50% of the stroke survivors regain limited levels of ambulation [4]. The effects of a stroke are determined by the extent and site of the brain injury. Around 40–60% of post stroke patients suffer from genu recurvatum and are treated with a rigid Ankle Foot Orthosis (AFO) [5].
Participants characteristics
Participants characteristics
The genu recuvatum gait is marked by a lack of tibial progression over the foot in stance which could be due to limited ankle range of motion (ROM) or insufficient hip extensor activity, allowing the pelvis to remain posterior to the hip during stance [6]. Ankle Foot Orthoses (AFO) are assistive devices commonly used to improve gait after stroke. This custom device improves gait and walking efficiency by manipulating the joint positions (through directing the ground reaction force), correcting abnormal ankle plantarflexion (ankle equinus) and knee hyper extension (genu recurvatum) during stance [7, 8, 9, 10].
In recent years many researchers have studied how to tune the AFO, with the intention of improving rehabilitation and orthotic management of post-stroke patients. Tuned AFOs can be occur by adding various heel heights under the AFO. This will alter the tibial inclination during stance phase and thus, change the knee flexion angle during mid stance.
This research focused on changing the anterior inclination of the tibia (AFO) to determine an optimum inclination to normalize lower extremity segment kinematics for individuals who had suffered hemiparesis secondary to stroke with genu recuvatum of 10
The aims of this pilot study were to investigate the optimum inclination of the Rigid Tuned Ankle Foot Orthosis (RT-AFO) to normalize knee kinematics for stability in the sagittal plane with 10
The study protocol was reviewed and approved by the Institutional Review Board at Siriraj Hospital, Bangkok Thailand (Si 584/2015), and was supported by the SSPO Fund. Assessment of participants was performed as required for custom orthosis prescription. All participants were cast for a plastic rigid AFO with ankle foot alignment in neutral position. The rigid AFOs were fabricated from 5 mm polypropylene and reinforced at the ankle by adding 3 mm polypropylene.
Four hemiplegia post-stroke individuals who were able to ambulate within the community were recruited as participants in this study (see Table 1). The mean age was 51 years (SD
Five conditions with different tibial inclinations. A. without AFO (T1), B. RT-AFO 0
Comparison spatio-temporal parameters when walking without AFO (T1) to other four conditions (T2,T3, T4, T5)
Gait measurements were performed in the clinical gait lab at the Sirindhorn National Medical Rehabilitation Institute (SNMRI), Thailand. Each subject carried out one gait analysis session and walked in five conditions (Fig. 1): without RT-AFO (T1), with RT-AFO in 0
Gait was analyzed using a motion capture system with 8 Vicon MX-T40 cameras (Vicon, Oxford, UK); 2 piA1000-48gc cameras (Basler, Germany); and 3AMTI force plates (AMTI, MA, USA). The sampling rates for the cameras and the force plates were 100 Hz and 1000 Hz respectively. The trajectories of 38 markers placed on anatomical landmarks, using a Plug-in gait full body model were collected (Fig. 2).
Plug in gait marker position on participants.
Comparison knee joint flexion-extension angle of five conditions: T1, T2, T3, T4, and T5 with normal (shaded area).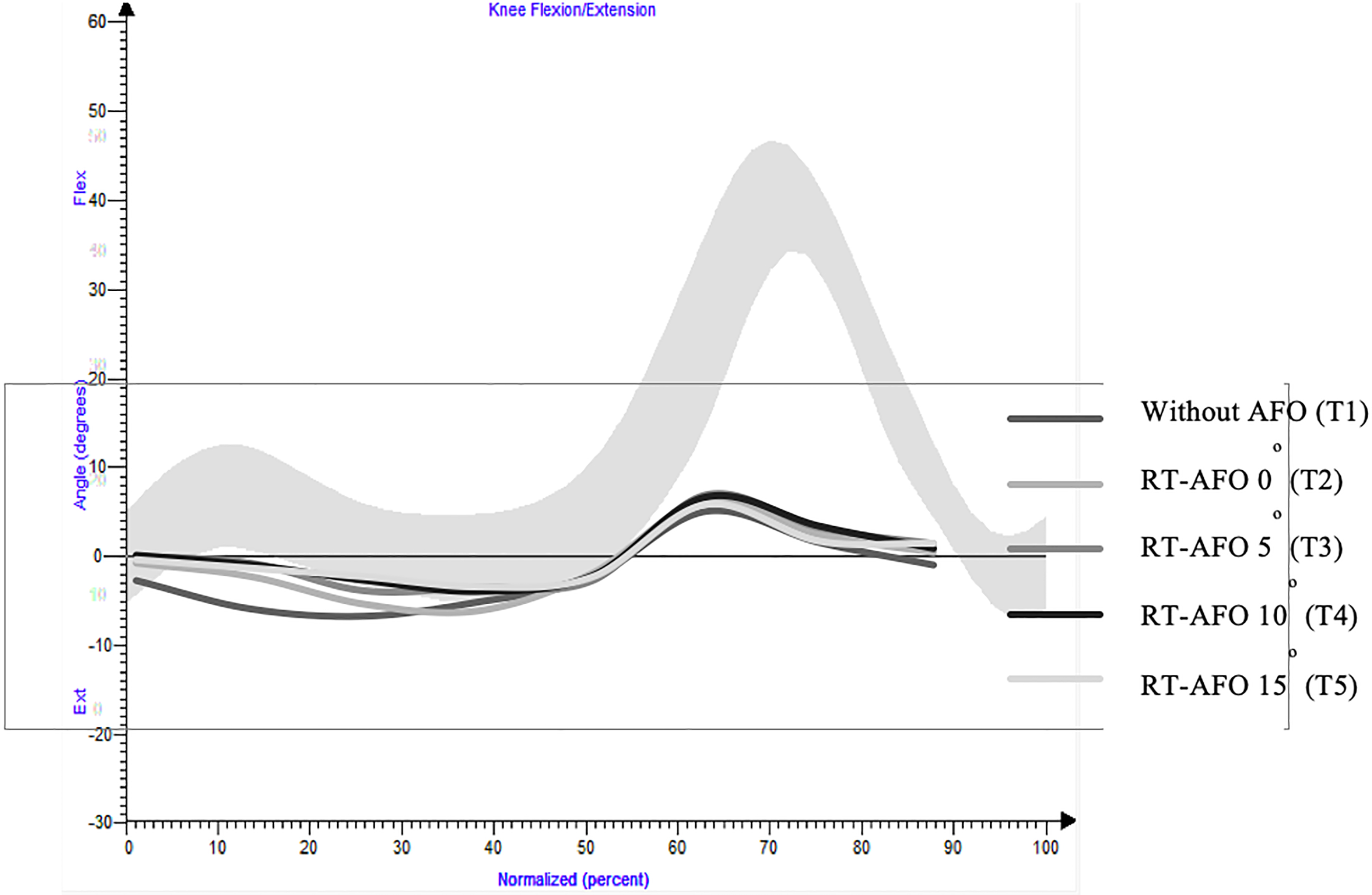
For statistical analysis, the nonparametric Kolmogorov-Smirnov test was used to assess normality and evaluate distribution of four participants. Paired
The mean knee flexion-extension moments throughout the gait cycle for all the participants in all five test conditions are shown in Fig. 3. A significant reduction of GR angle was seen in all 4 conditions (T2, T3, T4 and T5) of RT-AFO with
Discussion
This study investigated varying tibia inclinations to obtain the optimum inclination of a rigid Ankle Foot Orthosis for post-stroke patients with 10
This study showed the highest genu recurvatum angle in mid stance when subjects were walking without RT-AFO (T1) with a mean value of 17.2
The study results align with Jagadamma’s study which evidenced a reduction in the knee extension moment arm after using a tuned AFO Foot Combining (AFO-FC) in a patient with hemiplegic stroke [13]. The elimination of genu recurvatum in mid stance was achieved in which the SVA had been modified to 14
This study demonstrated that the RT-AFO was also responsive to changes in spatial-temporal gait parameters such as cadence, stride length and walking speed. Our study reported the highest cadence in T4 (RT-AFO
Results from T5 (RT-AFO
The reason for a significance reduction in cadence in the current study could be due to a sudden changing of tibial inclination angles as a result of the lifts provided. Our participants experienced all condition continuously in one day without any adaptation time. Jagadama mentions an adaptation time for new inclination of at least 3 months [16], Carmo et al. mentions three months of wear time in order to promote an increase of gait velocity, cadence, step and stride lengths for stroke patient [17].
This study reported no significant differences in stride lengths and walking speed with RT-AFO. Other studies reported the same results as ours on the effect of varying tibia inclination in children with cerebral palsy wearing an ankle foot orthosis [18]. Lewek et al., noted that improvement of the walking speed can be achieved through intense gait training using at least six weeks of combined treadmill-based gait training followed by over ground practice [18].
These aforementioned accomidations as well as our own study limitations must be considered, as we were limited in our sample size which reduces the power of this data. Therefore, studies with a larger sample and longer study periods are recommended. Only knee kinematics and kinetics of the affected side in the sagittal plane, specifically in mid stance, were examined. Further studies of the optimum inclination of RT-AFO should evaluate hip joint metrics, other points of the gait cycle and in other reference planes as well.
Conclusions
The results of this pilot study indicate that the optimum inclination of RT-AFO is 15
Footnotes
Acknowledgments
We would like to express our gratitude to directors of SSPO and SNMRI for their support, motivation and encouragement during our research. We also sincerely thankful to our patients for their cooperation and enthusiasm shown.
Conflict of interest
None to report.