
Abstract
BACKGROUND:
Assistive technologies are playing vital role in frail seniors.
OBJECTIVE:
The paper presents the methodology and findings from the assessment of an active “intelligent” robotic rollator incorporating navigation assistance in frail seniors.
METHODS:
Thirty seniors, having moderate motor impairment were grouped into two categories according to their cognitive status. A complicated trail was defined to test their performance using a robotic rollator. The main descriptive statistics were given, while inference was performed via the corresponding parametric
RESULTS:
Navigation assistance was proved helpful to the cognitive impaired group. The results between the two groups were comparable in terms of completion time and success rate. The provided directional audio cues led to smoother walking paths and better orientation. There was no correlation between the MMSE values and the total time of the walk (
CONCLUSIONS:
The integration of navigation assistance in mobility assistance devices can help the elderly to effectively orient themselves in challenging and unknown environments.
Keywords
Introduction
Life expectancy at birth has increased by almost 20 years over the last half century [1]. According to the latest statistics, 962 million people are over 60 years old [2]. By the year 2050, it is estimated that more than 2 billion people will be aged 60 and over, and almost 400 million of them will be aged 80
Given the growth of the older population, health systems around the world should prepare to address the various health concerns of older persons. The leading causes of disability globally among aged 60 years or over, according to WHO estimates for 2012 are: unipolar depressive disorders, hearing loss, back and neck pain, Alzheimer’s disease and other dementias, and osteoarthritis. Falls is also a major cause of disability among older persons globally [4].
The loss of mobility, which is a very common occurrence, can be devastating to the elderly and seniors. The Census Bureau of the USA reports that mobility problems are the most common disability among the elderly [5]. Due to loss of mobility the falls and injuries are increasing and can be life-threatening. Mobility loss is also highly interconnected with depression. Mobility aids have been used to maintain independent mobility. Several studies have found that use of a mobility aid is a prospective predictor of increased risk of falling in older adults or is associated with falls and related injuries. Other studies have argued that use of the devices may actually increase risk of falling by causing tripping or by disrupting balance control through other mechanisms [6, 7, 8, 9]. According to the same study, although many studies have reported that mobility aids and/or environmental obstacles are associated with falls, the possible link between these two risk factors has not been studied. Furthermore, it appears that frame-walker-related injury can occur as a result of contact and/or “catching” of the mobility aid with environmental objects, such as carpets and doorframes that would not normally be considered obstacles [10].
Nowadays, there are a variety of mobility assistive devices in the market available. Gait assistive device users are involved at a significant percentage of fall-related injuries that end-up for hospital treatment [11]. 60% of all fall injuries concerning gait assistive device users occurred at home and 16.3% of the injuries associated with walkers (walking frames or rollators) occurred at nursing homes. Approximately 8.3% of injuries involving walkers and 12% involving canes happened in public places. Approximately 1.6% of walker injuries involved falls on stairs or steps [11].
Even though mobility aids can help in several issues, it is possible that the act of lifting the mobility aid (referring to walking frames or other similar devices) can lead to instability in the same way that lifting the foot can cause the centre of mass (COM) to fall toward the unsupported side during unassisted gait. By suddenly reducing the base of support (BOS), lifting the device could create a state of imbalance in which the COM lies outside the BOS limits. Moreover, the tendency of the walking frame to tip increases with the magnitude of the applied horizontal force and with the height of the walker [10]. When it comes to gait speed, the use of any walking aid, in particular walkers, results in a slower gait speed and requires considerably more energy and cardiovascular fitness than walking unassisted [12]. Also, as mentioned by [13], with a fixed frame walker, physiological cost index (PCI) was higher in a weakened elderly individual due to heart rate increase and lower walking speed.
There is little evidence to suggest whether the use of the walking aid alone leads to this risk or if it is related to the decreased level of physical function, increased frailty, and poorer general health that users of walking aids may have. However, inappropriate walking aid prescription, inadequate training of the user and un-prescribed use of walking aids are likely to exacerbate the problem [14].
The use of gait assistive devices, although can provide precious help for the elderly [13] or for the mobility-impaired, can also have limitations or adverse consequences. Studies show that 30% to 50% of people prescribed with a gait assistive device abandon their device soon after receiving it [15]. Furthermore, surveys indicate that almost half of the reported problems associated with cane or walker use fall under the category of difficult and/or risky to use [10]. 58.3% of knee osteoarthritis patients that possess a walking aid are non-users of the aid. At this case, nonuse is associated with less need, negative outcome, and negative evaluation of the walking aid [16]. Another example indicating the difficulty of finding and using an all-circumstances suitable gait assistive device is multiple sclerosis patients. According to [17] the vast majority of persons with MS who use a mobility aid own more than one type and about half own three or more different types of mobility aids. Persons with MS appear to “mix and match” different devices to suit their specific mobility needs.
Age is also the greatest risk factor for cognitive impairment. Due to the ageing of population, the number of people living with cognitive impairment is expected to jump dramatically. The imminent growth in the number of people living with cognitive impairment is expected to place significantly greater demands on the health care systems. New technologies are urgently needed for patients with any level of cognitive impairment in order to assist them in normal daily activities (i.e. walking and navigating in known or unknown places).
Several robotic intelligent mobility aids have been presented in the literature, largely divided into two categories: robotic wheelchairs and robotic walkers [18]. Robotic walkers constitute a mechanized version of the standard walking frame and are further divided into three main groups [19]: the Standard Walking Frame (aka Zimmer Frame), designed to provide support to a person with a lower limb weakness, the Rollators which is a standard frame attached with wheels used where balance – rather than weight bearing – is the major problem, and the Reciprocal Frames, similar to the Standard Frames except that the frame is hinged on either side allowing the sides of the frame to be moved alternately. They are designed to accommodate a normal walking pattern with opposite arm and leg moving together. All robotic walkers are a robotized variation of the Rollator frame, ultimately identified with mobile robots.
Many robotic walkers have been developed, generally presenting the following functionalities: (i) Physical support; (ii) Sensorial assistance; (iii) Cognitive assistance; (iv) Health monitoring and (v) Advanced human-machine interface [20]. The platforms largely fall into two categories: passive and active devices [21]. While passive mobility aids either steer or brake, but cannot move forward without the human applying forces on them, active devices are equipped with actuators and thus, their motion and interaction behavior can be actively controlled. Some examples of intelligent mobility aids are the iWalker robot [22], the GUIDO system (Haptica Inc., Dublin, Ireland), the Personal Aids for Mobility and Monitoring “PAMM” SmartWalker [23], another system also called SmartWalker [24], the JAIST Active RObotic Walker (JARow) [25], Fraunhofer’s Care-O-bot and Care-O-bot II [26], the LEA robot (Robot Care Systems bv, Den Haag, Zuid-Holland) and other.
The acceptance and use of innovative assistive technologies among people with cognitive impairment and their caregivers is still challenging [27]. The performance of daily activities by device-assisted walkers is partially restrained by a series of factors, having to do with the assistive device limitations or/and the limitations emerged from environmental causes. Specifically oriented to walking-aids, valid and reliable assessment tools to classify and clarify their limitations or users’ satisfaction were not tracked. A recent thorough review revealed the most valid and reliable instruments for the subjective measurement of assistive devices [28].
The current paper presents the assessment of an active “intelligent” rollator in order to evaluate the positive effect of a robotic mechanism incorporating navigation assistance in frail seniors. The system is initially planned to be used in institutional spaces.
Materials and methods
Intelligent mobility assistance robot
The robotic system used in this work, is a collaborative effort of several European partners under the FP7 EU funded project “MOBOT” (Intelligent Active MObility Aid RoBOT integrating Multimodal Sensory Processing, Proactive Autonomy and Adaptive Interaction). Focus of the project was the development of robotic mobility aids that provide intelligent and active mobility assistance to the elderly, by supporting safe autonomous proactive control of the physical user-robot interaction, and enabling multimodal sensory processing and natural human-robot communication [29]. MOBOT (Fig. 1) integrates novel functionalities such as Sit-To-Stand assistance [30], indoor localization [31], navigation assistance [32], user following [33], obstacle detection and avoidance [34] and other, into a context-aware mobility assistance robot. For a more thorough presentation of MOBOT’s functionalities, the reader is referred to [35].
The MOBOT intelligent mobility assistant robot, used in the experimental sessions.
MOBOT’s intelligent functionalities have been developed using the Robot Operating System (ROS) [36], currently regarded as the most popular software framework for research and development in robotics [37]. The ROS contains a large collection of open-source drivers, algorithms, tools, and libraries for the development of various robotic tasks. MOBOT’s navigation assistance module deployed in this work, was built utilizing ROS’s navigation stack [38], which is extensively used by research teams around the world for autonomous robot navigation. ROS stacks comprise algorithms and tools with a specific objective, as for example, navigation. MOBOT’s navigation assistance task consists of the following sub-tasks: map building, odometry, and localization. To facilitate these sub-tasks, the rollator was equipped with two high-precision quadrature optical encoders on the two rear driving wheels, a laser range finder (Hokuyo UTM-30LX) on the front of the robot, facing towards the direction of motion, and an inertial measurement unit (IMU, XSensMTi-G-700 GPS/INS) mounted on the chassis of the rollator. Mapping was performed using the openSLAM Gmapping library. This creates maps of unknown environments using scan data from laser range finders. Prior to any experiments, a static map of the indoor environment was created. The position and orientation (i.e. pose) estimation of the robot, was performed using odometric information, relative to a starting position. This was achieved by integrating over time the rotation of the rear wheels, as measured by their respective quadrature encoders; a technique called dead reckoning. In this technique, the current pose is estimated by calculating the relative displacements from a previous pose [39]. Odometric pose estimation is a well-established method in robotics, providing good short-term accuracy. However, the integration of incremental motion over time inevitably leads to the accumulation of errors, due to, for instance, wheel slippage and measurement noise. This accumulation increases proportionally to the travelled distance [40] and may result in very large pose estimation errors. To handle this problem, the estimation of the robot’s angular velocity was calculated from the gyroscopic data of the IMU, and consequently fused to the estimation of its linear velocity, provided by the wheel encoders. This data fusion reduced the error estimation error and provided a more robust solution [41]. The estimation of MOBOT’s position and orientation on the known map, created prior to the experiments, is called “Localization”. This was attained using ROS’s Adaptive Monte Carlo Localization module, which provides probabilistic robot localization in 2D maps using a particle filter [42]. The navigation assistance system provides pre-specified auditory localization information and navigation instructions to the user while they have full motion control over the MOBOT rollator (manual control mode). The module considers the known pre-built map, along with a set of predefined guard points which have associated audio cues. Each guard point consists of two states: the “in” stathe and the “out” state. The transition to the “in” state is made when the rollator enters a circle of specified radius centered at the guard point. Conversely, the transition to the “out” state is made when the rollator exits this area. On entering a guard point, a precise directional audio cue is provided guiding the user safely on a direct route to a preselected destination. While inside the guard area, the audio cue is repeated every 3 seconds, until the user exits the specific guard point. The guard are treated as a directed path. This means that when the rollator exits a guard point, this is discarded and removed from the route. Only subsequent guard points are then considered.
The study was approved by the Bioethics and Deontology Committee of the Technological Educational Institute of Athens. A written informed consent was obtained from each participant. The evaluation study took place in a Greek rehabilitation hospital and examined the assistance provided by the robotic rollator focusing on the navigation functionality.
The evaluation scenarios were tailored to meet the needs of the research using both objective and subjective criteria. To this end, a multi-disciplinary team was established to coordinate the project, constituted by a biomedical engineer, a robotic engineer and a physiatrist. The objective evaluation of the robotic rollator was based on the collected various data from the multiple sensors integrated in the robotic rollator-type device. The subjective assessment of the device was another major issue [28], and was achieved by using three already validated questionnaires [43, 44, 45].
Design and experimental setup
The objective of the cognitive assistance scenario was to assess the integrated navigation functionality of the MOBOT robotic rollator, related to the assistance of the end user when navigating in a trail. MOBOT provided the audial navigational assistance described in the previous section. The experimental premises were mapped prior to the trials, while the navigational trails, along with the guard points and their associated audio cues, were designated on the map and encoded into the system before initiating the experiments.
According to the research hypothesis, the cognitive assistance functionality would assist subjects from Group B (cognitive impairment group, MMSE
Layout of the navigation trail at the rehabilitation hospital.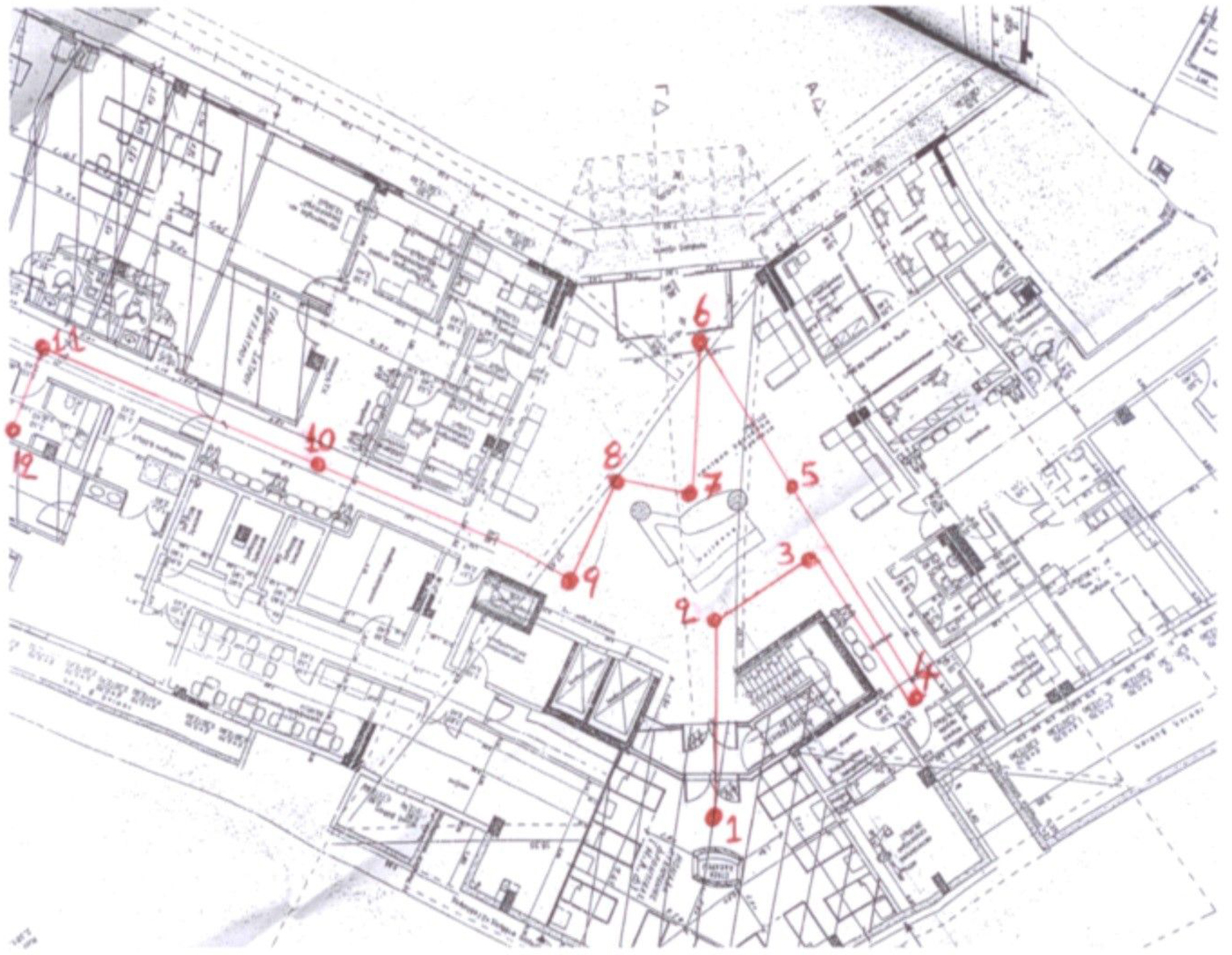
1 2 3
The appropriate audio cues for each point on the navigation trail where imported in the system (Table 1).
Audio cues list
Both Group A and Group B performed the navigation trail with the MOBOT rollator-type device used in a leading mode. All participants were instructed about the final targets prior to initiating the experiment. They were instructed to try to reach the designated targets by following the directional audio cues provided by MOBOT. No period of familiarization or practice run using the MOBOT rollator was required before starting the route and no doorways had to be negotiated. The hospital staff was not allowed to give any hint or help during trials. MOBOT’s navigation assistance was provided when MOBOT reached a certain area defined around each one of the points. Each audio cue was repeated every 3 seconds until the participant has left the critical area of the point (Fig. 3). During the experiments, all participants were accompanied and supervised by health professionals in order to help or stop the experiments in case a subject was tired and prevent falling or other unexpected situations. There was no stop for the patients between the targets and the system was automatically recording the time elapsed for each target.
Critical areas of the trail.
The recruitment process was very time consuming since the right subjects had to fit the evaluation strategy. The participation was on a volunteering basis with no other incentives provided. Due to the health conditions of the target group there was also a great risk of drop out that could be caused due to fatigue by the requested tasks. An extended period of screening and evaluation of the potential subjects and their medical files was conducted. Both inpatients and outpatients of the rehabilitation hospital as well as of other collaborating geriatric settings were examined. The inclusion criteria of the subjects were: (i) being users of an assistive device (rollator type) for at least a month, (ii) having a moderate motor impairment (habitual use of rollator, gait speed
Performance metrics
The MOBOT rollator-type device was assessed during the experiments using both objective and subjective performance measures.
Objective measures:
success rate (first/intermediate/final target position) task completion time (first/intermediate/final target position) stopping time
Subjective measures:
Additional objective measures (walking trajectories, gait parameters captured by laser sensor) which can be applied in future work were also collected during the experiments.
Sample descriptive characteristics
Note.
Total time of the walk
a. Grouping Variable: Gender. b. Not corrected for ties.
Total time of the walk.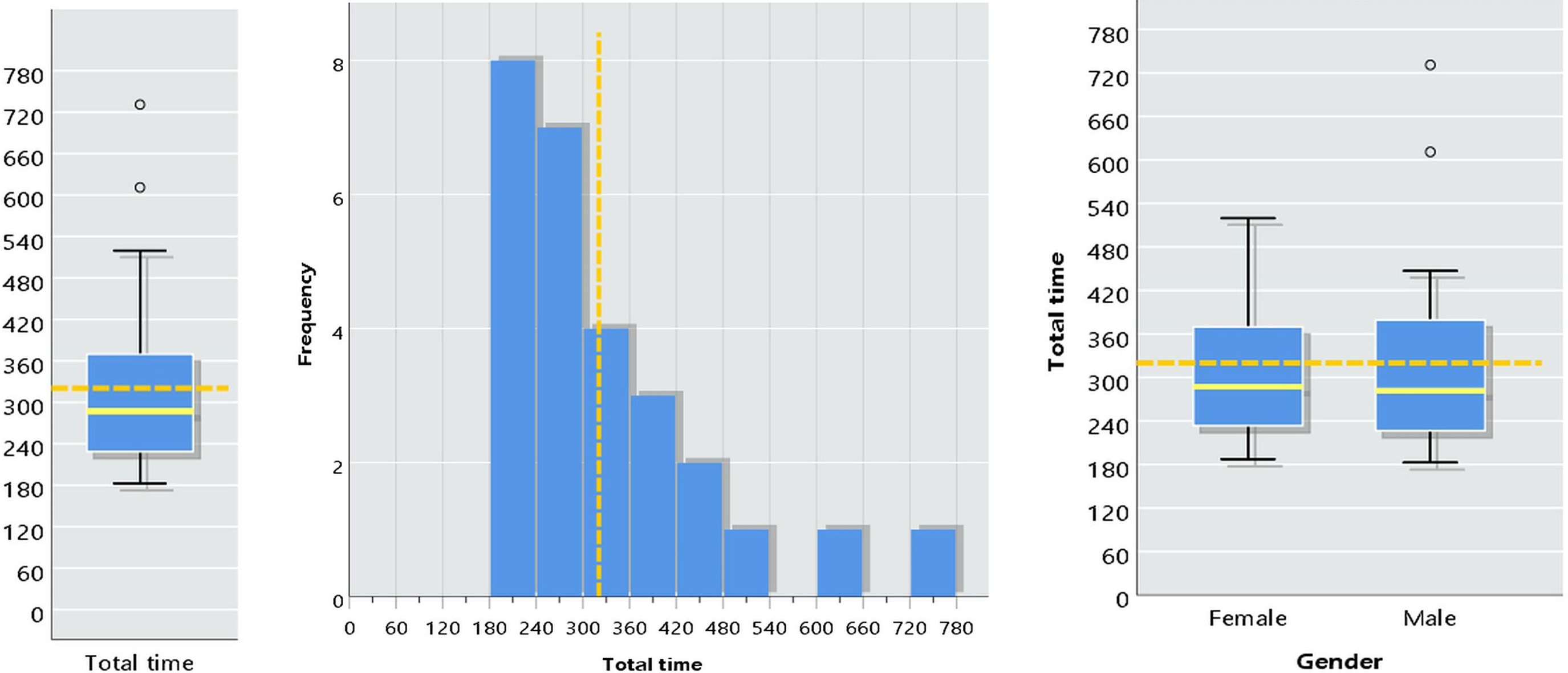
For the statistical analysis and inference regarding the collected data, we first examined their distribution. The normally distributed data variables were analyzed using
Results
After a long period of recruitment process, a total number of 30 subjects (out of the 425 screened) participated in the study. The subjects were appropriately distributed in order to have two equal groups of participants: 15 with cognitive impairment (MMSE
Sample description
The study did not focus on pathologies rather on the functional status of the participants as described in the inclusion criteria. The sample basic descriptive characteristics are presented in Table 2.
The average patient is 78.6 years of age and this value reflects the whole population since the age of patients is normally distributed (
Total time of the walk and age.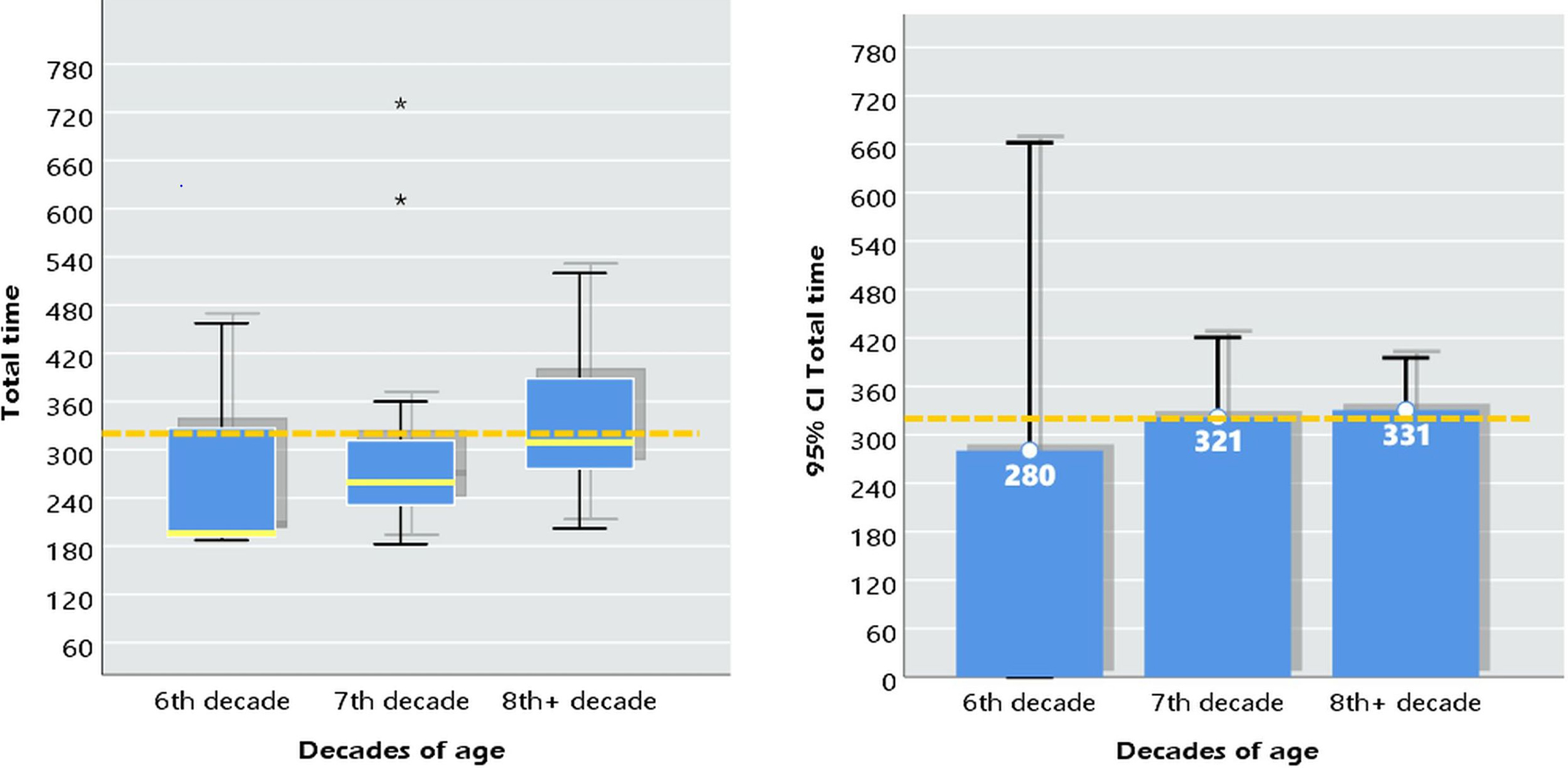
The mean MMSE score was 24.8
The accomplishment time (total time) for each participant was measured by adding the times spent in each point (Point 1 to 12) along with the ones spent while walking between the points until reaching the final target (Point 12). The total time is illustrated in the left boxplot and histogram of Fig. 4, with mean value 320.5 s and median 287.3 s. In a 95% confidence interval, their mean times range from 267 s (4.5 min) to 373 s (6.2 min). Note that the mean value is higher than the median since two patients were a lot slower than the rest (over 600 s), which is also confirmed by the aforementioned boxplot, and hence the median is more informative about the central tendency of the total time.
Male and female patients show no difference in their average time of the walk (
In relation to their age, there is no difference in their average walk time (
Total time of the walk with respect to age
Total time of the walk with respect to age
a. Kruskal Wallis Test. b. Grouping Variable: Decades of age.
Section completion times of the trail
a. Friedman test.
Section completion times of the trail.
Considering the three sections of the trail, they exhibit different patterns; see boxplot and means bar plot in Fig. 6. This pattern of mean times can be (statistically) confirmed for the whole population (
Only one participant failed to complete the first section (Point 1 to Point 4) of the trail, and one more failed at the second section (Point 4 to Point 6). All other participants completed the task.
Walk time in relation to institutionalized patients
a. Lilliefors Significance Correction.
a. Grouping Variable: Institutionalized. b. Not corrected for ties.
a. Grouping Variable: Fear of falling. b. Not corrected for ties.
Institutionalized patients may seem to vary their total walk time in our sample (Fig. 7), however we infer that the population of the institutionalized or not patients (using the MOBOT device) have on average the same total walk time (
Walk time and MMSE
a. Grouping Variable: Mental status (MMSE categories). b. Not corrected for ties.
Walk time in relation to institutionalization.
Walk time and MMSE.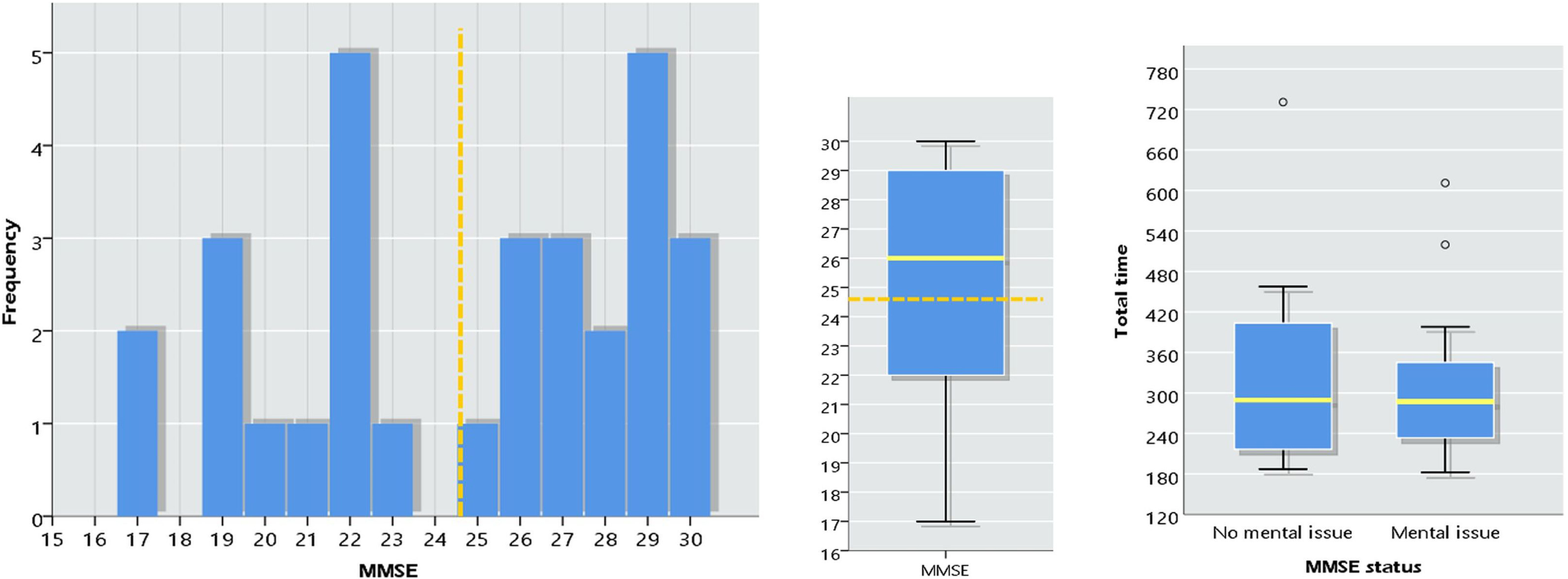
Total time of the walk and functional independence (BARTHEL).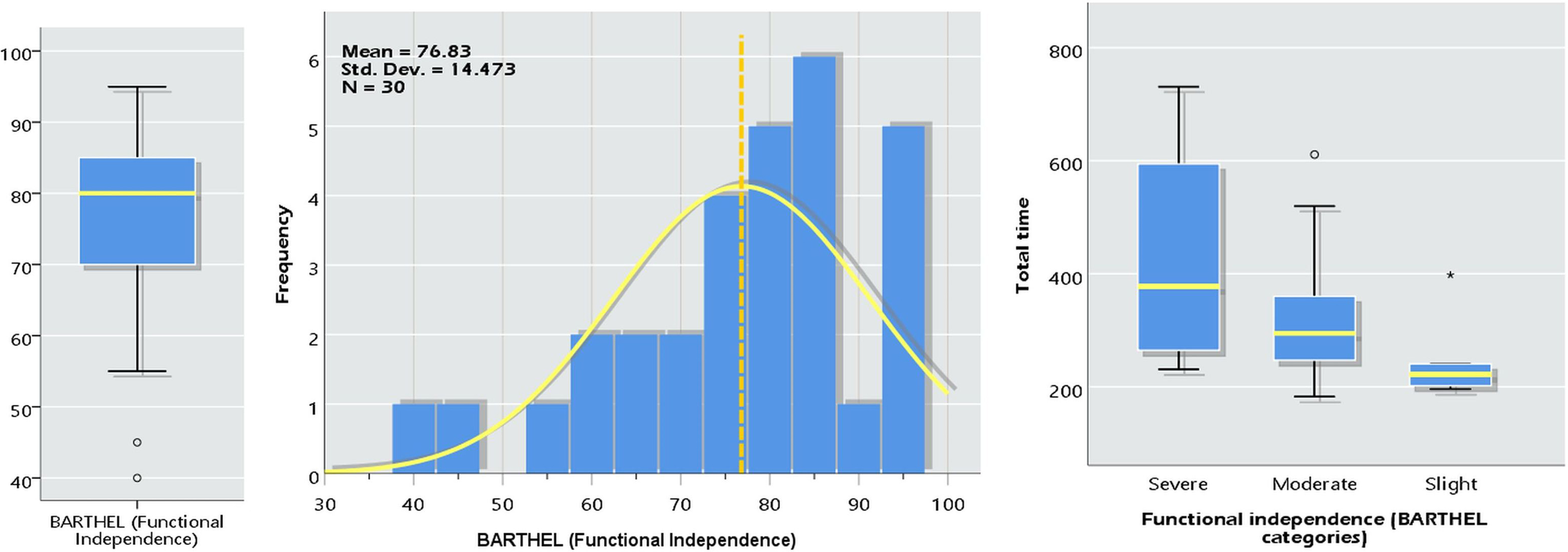
The histogram (top left sub-figure) and the boxplot next to it in Fig. 8 illustrate the MMSE values of the patients’ sample with mean 24.67. In our sample, 56.7% of the patients have mental issues (MMSE
Similar to the results for the MMSE, the BARTHEL values do not have a statistically significant association with the total time of the walk (
Total time of the walk and functional independence (BARTHEL)
a. Kruskal Wallis Test. b. Grouping Variable: Functional independence (BARTHEL categories).
Satisfaction ratings for MOBOT
a. Grouping Variable: Gender. b. Not corrected for ties.
Satisfaction ratings for MOBOT.
Scree plot for the PCA.
Regarding the overall subjective satisfaction form the use of the MOBOT Rollator, Fig. 10 demonstrates the corresponding histogram and boxplot of the PYTHEIA values with mean 3.98 measuring the overall satisfaction of the users with MOBOT. When responding to Part B of the PYTHEIA questionnaire, subjects assessed the cognitive assistance functionality with 4.46 and the audio-gestural interaction functionality with 4.30, indicating their high level of satisfaction from the experience of using these features [43, 51, 52]. These ratings are not statistically correlated with their total time of the walk, nor their MMSE and BARTHEL values (
Principal component analysis
Extraction Method: Principal Component Analysis. a. When components are correlated, sums of squared loadings cannot be added to obtain a total variance.
Extraction Method: Principal Component Analysis. Rotation Method: Promax with Kaiser Normalization. a. Rotation converged in 13 iterations.
Applying the Principal Component Analysis (PCA with Promax Rotation Method), we obtained four components that explain 70.4% of the total variance in our sample (
The present study focused on the assessment of the cognitive assistance provided by a robotic rollator utilizing navigation functionalities. The target group was frail seniors with and without cognitive impairment. The study design was based on the findings of previous research activities [28] in order to follow an appropriate methodological approach. Clinical measurements and observations were the base for selecting an adequate number and sample of participants. The subjects, following the inclusion criteria, are the targeted end-users of the evaluated robotic assistive device. Their physical health condition was also taken into account in the navigation trail design in order to avoid dropouts of the participants due to the effort, tiredness and other related factors. According to the results, almost all participants reached the final target following the navigation trail. Only two subjects didn’t make it to achieve the final target (point 12 of the trail). The first one failed from the beginning and the second one finished only the first section of the trail.
As indicated by the current research, a major outcome is that their cognitive status did not influence the results of the two different groups (cognitive impaired and not). As a common ground, all participants had no previous knowledge of the places where the navigation took place. Their only help was by the MOBOT system (using the audio cues presented in Table 1, which were triggered automatically when they stopped in a position for some time or when they were lost). The results reveal that even cognitive impaired people can achieve results similar to normal groups when using innovative technologies like the one provided by the MOBOT robotic rollator. The functionality offered (navigation assistance) is really helpful when navigating in unknown spaces where no signs may appear or when orientation problems appear.
The short completion time of the cognitive impaired group was apparently achieved based on the navigation assistance given by the system. Participant’s disorientation in several points was immediately improved by the given assistance, resulting in the achieved completion time which was comparable with the one of the not cognitive impaired group (MMSE
In this study we have chosen to provide audio cues to convey navigation assistance messages, which was made possible because all of the subjects included in the study had no major hearing impairment. To cope with mild to moderate impairments, the volume/loudness of the audio cues was adjusted to the needs of each participant, which proved to be a helpful personalization feature of the MOBOT navigation assistance system. The use of headphones is of course another available and easy to install option, which could provide an additional solution also coping with environment regulations regarding loudness and noise level (e.g. in hospital settings where it would not be proper to use very loud audio cues). In future research work, it is envisioned to further explore other features related to online personalization of the system, such as automatically adjusting the volume of audial cues in different areas depending on the anticipated (or detected) background noise level (e.g. large crowded hallways etc.), in order to improve the user-friendliness of such a navigation assistance modality. We also plan to further explore and compare the use of other feedback modalities including combinations of audio-visual navigation cues.
Such a technology can be proved helpful in several environments. For example, a MOBOT-like device can help carers, physiotherapists, occupational therapists and nurses in rehabilitation hospitals, since they will no longer be required to accompany their patients at every step. The decongestion of paramedical staff is considered an extremely important issue in hospitals that also affects their economics. The hospital’s staff can focus on more important tasks in their daily routine. However, safety issues should always be taken into account and a more in-depth research study is needed before deciding to leave a patient totally unsupervised by a carer using any such device. Moreover, the integration of navigation assistance in a rollator could reduce the fear of getting lost or falling in the targeted group. This could also lead to improved physical and social activities. The same device could also be used in a non-controlled environment after some modifications. Even though the initial designed MOBOT robotic rollator was used in a constrained environment (hospital setting), it is envisioned that after appropriate mapping of other places, using for example predefined guard points, would allow its use in less controlled places for more typical use. Current and future research work in follow-up projects include extending the use-case scenarios to address a larger scope of application environments, as well as integrating the technologies on a more commercial-oriented prototype with improved functionalities, much smaller size and more elegant than the original MOBOT prototype used in this study.
In the early years of many technical fields, the research community often utilizes a wide range of metrics that are not comparable due to a bias towards application specific measures. The primary difficulty in defining common metrics is the incredibly diverse range of human-robot applications. Thus, although metrics from other fields (HCI, human factors, etc.) can be applied to satisfy specific needs, identifying metrics that can accommodate the entire application space may not be feasible [55]. Attempts to categorize both objective and subjective metrics have been made. In our study, we combined both objective and subjective measurements in order to conclude on the usefulness and acceptance of the provided service/product. However, as reported in the Introduction section, the subjective measurement of user satisfaction is not an easy task. As reported in [28] most of the studies are utilizing either custom-made questionnaires or interviews that are neither valid nor reliable instruments to represent the subjective opinion and perception of the end users. The absence of standard scales/questionnaires for the subjective assessment of robot-based devices makes it difficult to design products that meet exactly the needs of the intended end users, to further improve prototypes, or to compare the results from different researchers. A great advantage of our study was the fact that all three questionnaires used (PYTHEIA, ATDPA, QUEST 2.0) were already tested for their reliability and validity in the Greek population [42, 43, 44, 45], thus claiming valid results. Moreover, PYTHEIA’s capability to capture the satisfaction of the end users with assistive and robotic technologies, while being able to evaluate any individual features/functionalities implemented was proved to be valuable. This is not present in any other scale.
The early abandonment of assistive devices is also a major issue. Certain studies show that a big number of patients don’t use (or abandon early) their gait assistive device, when other studies speak of patients using more than one mobility aid. Two of the most common limitations or dissatisfaction reasons while using the mobility aid are: handling the rollator, social stigmatizing. According to the results of the presented study, the users not only enjoyed using the robotic rollator, but also were feeling more safe and secure, while thinking of it as a hi-tech gadget. Thus, they wanted and really enjoyed to participate in the study even without any other incentives given. Social stigmatizing seemed not to be concern due to the innovative characteristics of the robotic rollator.
The collected results on objective performance metrics of the cognitive assistance scenario are quite promising, indicating that cognitively impaired participants achieved comparable performance (i.e. task completion time) with non-cognitive impaired subjects, using the MOBOT’s cognitive assistance system when completing a navigation task in a complex real-world application scenario. Results on the subjective user satisfaction are also very positive and suggest that the use of this cognitive assistance functionality provides a benefit for the users, do not cause feelings of insecurity, is an interesting challenge for the users, and may have a positive effect on the user’s quality of life. These results indicate the potential added value of such a robotic functionality for cognitively impaired, frail older people. Of course, regarding the positive results obtained in relation to the feeling of safety when using the device, we should point out the following. Though there has been a lot of research conducted in the frames of the MOBOT project focusing on topics such as human gait tracking, analysis, and characterization of pathological and stability features (using data provided by multiple on-board sensors), there was in fact no specific “fall-prevention” functionality integrated on the MOBOT rollator platform, which constitutes actually an important topic for future research. Therefore, we could attribute the feeling of safety perceived by MOBOT users as partly related to the apparent mechanical properties (mass, inertia) of the device, which have been actively controlled by means of an adaptive admittance controller (exploiting data provided by force/torque sensors mounted on the rollator handles); thus, apparently providing a reassuring feeling of safety when handling and maneuvering the device, assessed in the context of the subjective evaluation procedures of this study.
We should also point out here that, as it has been assessed by early experimental studies conducted in the frames of the MOBOT project, the use of the MOBOT rollator (with actively controlled admittance) does not have by itself any significant effect in the walking speed of the user as compared to a typical rollator. We can thus argue that the MOBOT device does not seem to constitute a limiting factor to the walking performance of rollator users, meaning that the results achieved by the non-cognitively impaired group can indeed be considered to constitute a measure of comparison, for assessing the effect of the navigation assistance functionality to the cognitively impaired group. Previous studies [56] have also confirmed that the performance achieved by cognitively impaired users, without any navigation assistance provided, is indeed significantly inferior compared to non-cognitively impaired users, a finding which also adds value to the results obtained by the study presented in this paper.
As far as the limitations of the study are concerned, we can refer the limited number of participants and the complexity of the navigation trail. Moreover, the hi-tech nature and novelty of the device with the natural tendency of the users to want to give positive responses to please the research team conducting the tests may also have bias the results to give more favourable results in the context of a subjective evaluation without the possibility of comparison with an alternative system. In a future research, we plan to test MOBOT taking into account the above parameters so as to have more accurate and generalized results. A new research effort has already begun in order to build a more elegant and smaller in size system able to be adopted in more typical environments outside a hospital.
Conclusions
The current research presents the integration of navigation assistance in rollator type devices. According to the results presented, this can effectively support orientation and navigation of cognitive impaired users.
Footnotes
Acknowledgments
We would like to thank the Diaplasis Rehabilitation center, the physiatrist A. Karavasili and her team, for helping us in the recruitment process and in collecting all the relevant data from the patients participating in the study. The work leading to the presented results has received funding from the European Union under grant agreement no. 600796.
Conflict of interest
None to report.