
Abstract
BACKGROUND:
Video games can be used to motivate repetitive movements in paediatric rehabilitation. Most upper limb videogaming therapies do not however include haptic feedback which can limit their impact.
OBJECTIVE:
To explore the effectiveness of interactive computer play with haptic feedback for improving arm function in children with cerebral palsy (CP).
METHODS:
Eleven children with hemiplegic CP attended 12 therapist-guided sessions in which they used a gaming station composed of the Novint Falcon, custom-built handles, physical supports for the child’s arm, games, and an application to manage and calibrate therapeutic settings. Outcome measures included Quality of Upper Extremity Skills Test (QUEST) and Canadian Occupational Performance Measure (COPM). The study protocol is registered on clinicaltrials.gov (NCT04298411).
RESULTS:
Participants completed a mean of 3858 wrist extensions and 6665 elbow/shoulder movements during the therapist-guided sessions. Clinically important improvements were observed on the dissociated and grasp dimensions on the QUEST and the performance and satisfaction scales of the COPM (all
CONCLUSION:
This study suggests that computer play with haptic feedback could be a useful and playful option to help improve the hand/arm capacities of children with CP and warrants further study. The opportunities and challenges of using low-cost, mainstream gaming software and hardware for therapeutic applications are discussed.
Participant demographics
Participant demographics
Cerebral palsy (CP) is a group of disorders caused by disturbances in the development of the fetal or infant brain [1]. CP can lead to significant limitations in function, activity, and participation [2]. Hemiplegic CP, the most common form, can cause functional limitations in one of the upper limbs’ which can interfere with self-care, leisure, and participation in daily activities [3, 4]. Occupational and physical therapies for hemiplegic CP aim to improve upper limb function through strengthening, endurance building, and motor learning activities.
In recent years, there has been much interest in the use of video games to promote engagement in pediatric rehabilitation [5]. The state of evidence supporting the use of videogaming therapies for young people with CP is moderate for motor function and balance, and weak for upper limb rehabilitation [6]. Most studies for upper limb rehabilitation that use gaming systems do not incorporate significant haptic feedback, an active component of traditional therapy. Physical task parameters introduced by therapists or interactions with real-life objects can aid in motor learning and the transference of skills practiced in virtual environments to real-life [7]. Previous studies with gaming systems such as the E-link Exerciser [8]. and the HapticMaster [9]. have incorporated haptic feedback for children with hemiplegic CP. Positive findings have been reported on outcome measures associated with upper limb function, speed and dexterity, and performance of everyday activities. These systems, however, cost several thousands of dollars which limits widespread availability and use.
The Novint Falcon (Novint Technologies, Albuquerque, New Mexico, US) is a low-cost, three degree-of-freedom (3DoF) video game controller that can provide haptic feedback during game play. Two previous studies investigated the Falcon for adult stroke rehabilitation [10, 11]. While promising, major drawbacks identified were that the available mini-games did not elicit therapeutically relevant movements, and the spherical grip on the controller was difficult to grasp. In our previous work, we report on the adaptation of the Novint Falcon and creation of a therapy gaming station for children with CP [12]. The gaming station was designed and tested for usability in partnership with children with CP and clinicians. The adapted Falcon gaming station enables children to perform a large number of clinically relevant movements while receiving feedback during play. High repetition rates combined with feedback has been shown to improve motor learning in people living with CP, even when the feedback received is quite subtle [13, 14] .
In this study, we investigate the question “Is therapist-guided use of a low-cost gaming station with haptic feedback clinically acceptable and potentially effective in improving upper limb function for children with CP?” Specifically, we will: (1) describe the therapy practice achieved (e.g. number of repetitions) and the experience (e.g. engagement, enjoyment) of children participating in the intervention; and (2) measure and identify clinically important changes on outcome measures related to use of the arm and hand following the intervention.
Methods
Design
In this prospective case series, participants completed a 12-session, in-clinic, therapy gaming program focused on grasp, isolated wrist extension, and motor control of upper limb movement in the presence of haptic feedback. Functional assessments were performed 1 week before the intervention and 1 week after the intervention. The study took place at Holland Bloorview Kids Rehabilitation Hospital (Holland Bloorview) in Toronto, Ontario, Canada and at the Center for Interdisciplinary Research in Rehabilitation and Social Integration (CIRRIS) in Quebec City, Quebec, Canada. Approval was granted by Research Ethics Boards at Holland Bloorview and by the sectorial rehabilitation and social integration research ethics committee of the CIUSSS-CN (Project #2015-547). All participants and caregivers gave written informed consent. The study protocol is registered on clinicaltrials.gov (NCT04298411).
The Falcon haptic feedbacktherapy gaming station. Key components include (A) the Novint Falcon, (B) three custom grips; (C) a baseplate to support interchange and rotation of the grips to accommodate varying pronation of the wrist; (D) a trigger button operated by the dominant hand; (E) an arm sling; and (F) a forearm mount to isolate wrist extension. Figure reprinted with permission.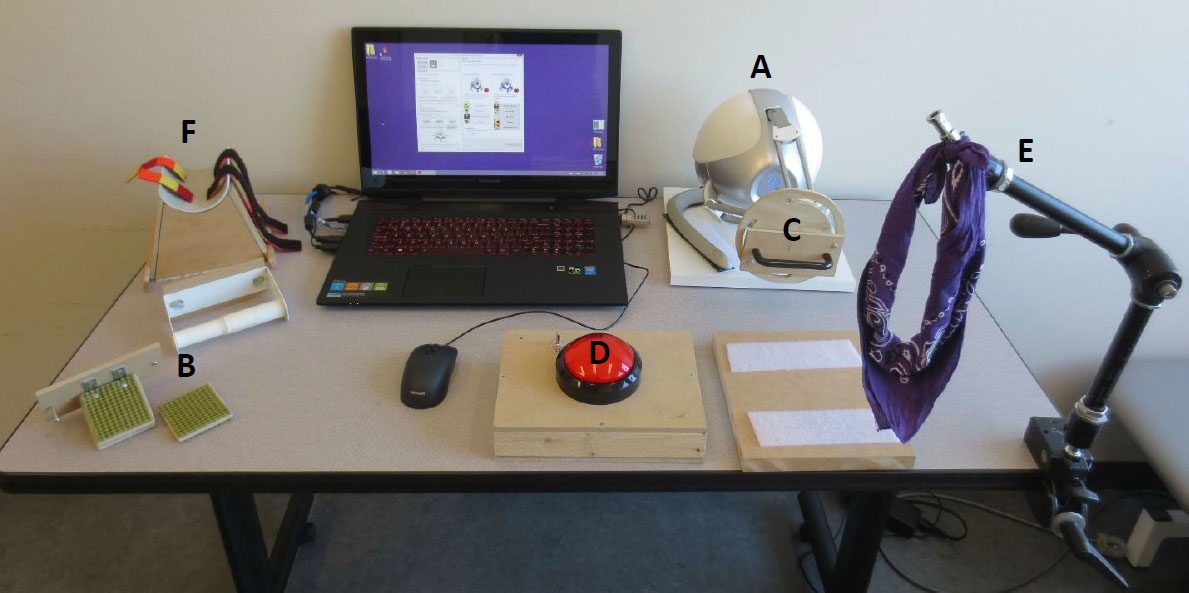
Thirteen children were recruited (mean ages 9.4 years [SD 2.6], 55% boys; Table 1). Inclusion criteria were: (i) diagnosis of hemiplegic CP, (ii) aged 7–16 years, (iii) typical or corrected to typical vision and hearing for video game play, and (iv) Level I (handles objects easily) to III (handles objects with difficulty) on the Manual Ability Classification System, MACS [3]. Of note, the MACS assesses overall ability to handle everyday objects, not the function of each hand meaning that a child assessed to be MACS Level I may still have considerable involvement of their hemiplegic limb. Exclusion criteria included: (i) Botulinum Toxin injections within 3 months, (ii) uncontrolled epilepsy, (iii) inability to answer questions in English or French. Participation in physical and occupational therapy programs that may have impacted hand/arm function was documented, but not restricted. At Holland Bloorview, potential participants were identified by occupational therapists. At CIRRIS, participants were recruited through an electronic mailing list of students and employees at Université Laval.
Procedure
Therapy gaming system
The Falcon gaming therapy station, detailed in previous work [12], consisted of the Novint Falcon haptic game controller with custom-built handles to facilitate therapeutically relevant grips (grips mainly used during activities of daily living such as lateral index to thumb lateral grip), a stand to isolate the wrist for extension exercises, a sling to relieve weight from the elbow/shoulder, a suite of commercial games, a big button that allows access to secondary actions in the games and promotes bimanual use of the hands, and a software application that allows therapists to calibrate settings (e.g. haptic feedback, range of movement) to individual therapy goals and abilities (see Fig. 1). Four games focused on wrist extension with game actions triggered when the wrist was extended past a threshold (1 – Crazy Rider, 2 – Swooop, 3 – Funky Karts, and 4 – Lil Mads and the Gold Skull; see Table 1 and Appendix 1). Five games were available for practicing elbow/shoulder movements (1 – Looney Tunes Dash, 2 – Heroes of Loot, 3 – Bird Brawl, 4 – Pac-Man and 5 – Save the Day). Participants navigated the game by moving the controller on the X and Y-axes at least 3.5 cm from the center using their hemiplegic hand (e.g. the avatar might jump when the controller was moved up on the Y-axis, crawl when the controller was moved down, or go forward when the controller was moved to the right on the X-axis). Additional game actions (e.g. throwing arrow, pushing the accelerator) were triggered by pressing the big button using the dominant hand. All games were played with a level of haptic feedback calibrated to each participants’ needs and abilities by the guiding therapist. To enhance motivation, every two sessions, one or two new games were made available until week 8 where the participant could choose to play any of the 9 available games. In order to provide a detailed record of the session activities, the system logs every game played, the number of game inputs (e.g. wrist extensions in the case of the wrist games), the duration of play and the calibration settings.
Intervention
Participants attended a 60-minute session once weekly over 12 weeks at a rehabilitation hospital or a private rehabilitation clinic. Higher frequency sessions were not possible as most participants were not available more than once a week due to school and other extracurricular commitments. During each session, participants used the therapy gaming station guided by a certified therapist or therapy assistant. Six different clinicians were involved in the intervention, three at Holland Bloorview and three at CIRRIS (2 occupational therapists, 1 physical therapist and 3 occupational/physical therapist assistants, experience level ranging from 2 to 25 years). Approximately half of the session was dedicated to games played through wrist extension with the remaining time reserved for games that required navigation of an avatar via controlled elbow/shoulder movements on a vertical plane. Clinicians began each session by securing the participant’s forearm on the wrist stand and calibrating the resistance/ haptic feedback to a level considered challenging, but not frustrating, for the participant. Maximum wrist extension was recorded and the threshold to trigger the game action was set at 75% of this value [12]. Participants then played the wrist extension games largely in line with their individual interests/preferences. In the last half of the session, the wrist stand was removed, and the elbow/shoulder support sling was positioned if needed (to support the arm and reduce compensatory movements for the most affected participants). A new calibration was performed for this second part of the session in order to adapt the games to the child’s capacities at the elbow/shoulder. The maximum displacement in each direction was recorded at elbow/shoulder level and a new threshold was set at 75% of these values. Participants then played games targeting controlled elbow/shoulder movements. During the session, if participants demonstrated fatigue (e.g. compensatory movement), frustration, and/or if the games did not elicit enough challenge, the guiding clinician was free to re-adjust the settings as needed (e.g. increase/decrease resistance/haptic feedback, switch to a different game).
Measures
The objective of this intervention was to improve upper limb function in a way that was meaningful to children by introducing physical task parameters (i.e. haptic feedback) into the virtual training [7]. Outcome measures were selected to investigate the function, activity, and participation domains of the World Health Organization’s International Framework for Disability, Functioning and Health [15]. Primary outcome measures were the Quality of Upper Extremity Skills Test (QUEST) [16], a measure of function, and the Canadian Occupational Performance Measure (COPM) [17], a measure of participation. Secondary outcome measures included: grip strength and the Children’s Hand-use Experience Questionnaire (CHEQ) [18], a measure of activity. Clinician- and self-reported feedback was collected to provide context with respect to each child’s active participation and engagement in the rehabilitation process.
QUEST
The QUEST is a criterion-referenced measure developed for children with CP that is composed of 34 tasks related to 4 dimensions of upper limb quality of movement: weight-bearing, protective extension, grasp and dissociated movement of the shoulder, elbow, and wrist [16]. For each domain, several movements are assessed using a dichotomous scale (yes/no). Percentage scores are calculated for each domain and a total score is calculated by summing the domain scores and dividing by the number of domains. However, it has been suggested that reporting score by domain leads to higher reliability [19]. For this study, the dissociated movement and grasp domains were of primary outcomes of interest. The dissociated movement domain looks at movement of the shoulder, elbow, wrist and fingers, as well as arm position during grasp/release. The grasp domain evaluates performance in grasping everyday objects and the posture of the head, shoulders and trunk during grasping activities. The QUEST was developed for and validated with children with CP aged 18 months to 8 years [20]. It has excellent reliability and has demonstrated responsiveness [16]. As in a previous study, a difference of 5 score points in any individual domain was considered a clinically important improvement [21]. In previous studies of neurodevelopmental therapy and casting [22], a change of 4.89 points on the QUEST total score inclusive of all 4 domains was determined to be a positive treatment outcome [20]. for children with CP.
COPM
The COPM assesses self-perceived performance and satisfaction on activities of importance to child/fam- ily [17]. Families worked with an occupational therapist to identify up to 3 meaningful goal areas (e.g. cutting food) that we might reasonably expect to be impacted by the therapy gaming intervention. Participants rated their performance and satisfaction for each goal/challenge area on a scale from 1 to 10 (low to high) pre and post-intervention. Average scores for performance and satisfaction were calculated across the goals. The COPM is extensively used with children with CP and has good validity, responsiveness, reliability, and ability to track change over time [23, 24]. A change of 2 points on either the performance or satisfaction scale is considered clinically significant [25].
Grip strength
Owing to equipment availability at the two research sites, two different systems were used to measure grip strength: at Holland Bloorview, a modified sphygmomanometer pumped to 20 mm Hg following established protocol [26, 27] and at CIRRIS, a Jamar dynamometer was used. The same system was always used for the same participant. For both, measurements were taken with the participant in a seated position, with the arm adducted, elbow flexed to 90
CHEQ
The CHEQ v 2.0. is an online questionnaire of 29 bimanual activities of daily living for children between 3 and 18 years old [18]. The questionnaire is completed by the child, parent or another primary caregiver. In this study, the CHEQ was completed by the child with the help of their parent or the primary caregiver when needed. The CHEQ provides information about the child’s level of independence by asking if the child perform the task alone (i.e. Is this something you usually do independently?) and the level of involvement of affected hand (i.e. Do you use one hand or both hands together?). Responses on the CHEQ were used to calculate the percentage of activities that could be completed independently by the child and the percentage of activities for which the child involved the hemiplegic hand (to support or grasp). The CHEQ has demonstrated high test-retest reliability and ability to detect change in previous studies [18, 29]. Values for the minimum clinically important difference have yet to be established for the CHEQ [30]. Previous studies have considered an increase of 10% in bimanual activities performed independently to be clinically meaningful [21].
Participant and therapist reports
Therapists completed a session log rating their observation of the child’s initial excitement, engagement, enjoyment, frustration, fatigue, and overall satisfaction with the therapy gaming session using a 5-point Likert scale of agreement with 1 indicating “not at all” and 5, “very much”. After the final session, participants at Holland Bloorview rated their agreement on a 5-point Likert scale with six statements pertaining to challenge and immersion (e.g. appropriateness of challenge level, fairness of scoring, fun, extent of absorption in game, desire to play frequently), and 3 statements pertaining to perceived usefulness. Additionally, a short, structured interview was conducted with the Holland Bloorview participants to explore participants’ enjoyment, perceived value, suggestions for improvement, and desirability for home use.
System logs
System logs of the games played, time spent in active therapy practice, and the number of wrist extensions and elbow/shoulder movements practiced were collected.
Data analysis
Descriptive statistics are provided for all outcome measures. Following confirmation of normal data distribution, paired
Results
One participant at Holland Bloorview attended three sessions and then withdrew after multiple cancellations owing to difficulties commuting to the hospital. One participant at CIRRIS attended 5 sessions prior to a hardware failure which required several weeks to resolve. Only data on the 11 participants who completed the trial are reported. None of the participants were engaged in concurrent therapies that targeted the upper extremities. Most participants had an intrinsic interest in video game play as a leisure pastime and spent on average 77 min/day [SD 37.4 min/day] in video game play for entertainment. Over the course of the intervention, participants received on average 453 minutes [SD 57] of active therapy time and completed 3858 [SD 2118] wrist extensions and 6665 [SD 3985] repetitions associated with elbow/shoulder movements (Table 2).
Summary of intervention dose by participant
Summary of intervention dose by participant
*Impacted by technical difficulties with the system.
A clinically important improvement (i.e.
COPM
Targeted goals largely involved activities requiring a power grip (e.g. cutting meat, maintaining grip on park equipment; see Supplementary file). For all participants, a clinically important improvement (
Grip strength
A clinically important improvement (
CHEQ
A clinically meaningful increase in activities performed independently (i.e.
Therapist and participant perspectives on the gaming intervention
Table 4 presents therapists’ reports of participant’s in-session engagement which was generally positive. While moments of frustration were observed, overall, frustration was considered quite low (median
Summary of pre- and post-assessments of grip strength, quality of upper extremity skills (QUEST) and children’s hand-use experience questionnaire (CHEQ)
Summary of pre- and post-assessments of grip strength, quality of upper extremity skills (QUEST) and children’s hand-use experience questionnaire (CHEQ)
*indicates a change at a level considered to be clinically meaningful; ns: not significant, descriptive analysis are displayed only for significant results.
Therapist ratings of participant behavioural engagement (5-point Likert Scale of agreement where 1 indicates Not at all and 5 indicates Very much)
more enjoyable than regular therapy exercises (Table 5). Participants agreed strongly that the games could help improve physical abilities sharing views such as “I was moving my hand more and I was using muscles in my hand that I usually don’t, so I think that helped me improve”[P1] and “I learned how to grasp better. My wrist extension also improved” [P2]. These qualitative perspectives were largely concurrent with participants’ QUEST scores. All participants except P4 confirmed their desire to have the therapy gaming station for home use. When asked how often they would anticipate playing it at home, responses ranged from 3 times a week to every day, except for P4 who said “only if I had to”.
Participant ratings of the gaming therapy experience
This pilot study provides preliminary data on the effectiveness of therapist-guided use of a low-cost gaming station with haptic feedback for hand/arm motor rehabilitation of children with CP. There are numerous studies where mainstream gaming systems (e.g. the Nintendo Wii, MS Kinect) have been used for upper limb rehabilitation with limited success [6]. To our knowledge, this is the first study to integrate haptic feedback into the therapy gaming activity using mainstream gaming components for children with CP. Key findings are: (1) participants overall enjoyed the therapy gaming intervention and achieved a high intensity of wrist extensions and controlled arm movements; (2) Clinically important and statistically significant improvements were observed on the grasp and dissociated movement dimensions of the QUEST and on the COPM, indicating potential transfer to everyday life. The following discusses these key findings in greater detail.
High intensity practice and positive patient experience
On average, a therapy session scheduled for one hour yielded 37 minutes of active practice time with the system which compares favourably to a previous study using a haptic robot which documented an average 24 minutes of active practice per hour [9]. This perhaps attest to the relative ease of set-up of the Falcon gaming station. Participants achieved on average more than 300 wrist extensions and 550 arm movements per session. Interestingly,
Participants appeared to enjoy the gaming therapy
Interestingly, the two participants (P10, P11) who exhibited lower levels of enthusiasm also had greater hand involvement (MACS Levels II/III and III). Practice sessions for these participants were associated with significantly lower repetition rates, also likely related to their higher level of hand involvement. Of note, in this proof-of-concept system, we could not optimize the difficulty of the mainstream gaming software (e.g. timing of game events). For individuals with higher levels of hand involvement, games designed specifically for therapy with customizable game speed and/or required timing of movements would allow for a more optimally adjusted challenge point. Lastly, with the exception of P5, participants agreed that playing the games was helping to improve their physical abilities, indicating a high level of perceived value or cognitive engagement in the rehabilitation process. For P5, the game was appreciated for its entertainment rather than its therapeutic value. Interestingly, P5 was the only participant who did not show clinically meaningful improvements on any of the objective clinical outcome measures.
Clinically important outcomes
Across the group, statistically significant improvements were observed on the QUEST and on the COPM following the intervention. Medium effect sizes were observed for the grasp and dissociated movement dimensions of the QUEST and large effect sizes for the COPM. At the observed effect size of 0.6 for the grasp dimension of the QUEST, a sample size of 90 (45 in each group) would be required for a definitive randomized controlled trial assuming alpha significance set to 0.05 and a desired power
Seven of 11 participants showed clinically important improvements in grasp and/or dissociated movements as measured on the QUEST and all participants reported clinically important increases in performance and/or satisfaction on self-selected goal areas on the COPM. This suggests that there may have been a transfer of skills acquired through the intervention to activities of daily living considered meaningful to the participant and family. Changes on the CHEQ, also a self- or parent-reported measure, were less conclusive and mixed in outcome. While the COPM assesses activities in goal areas that are selected by the child/family, the CHEQ assesses a mix of tasks generally performed in activities of daily life with the validity of its change scores still under investigation [30]. Of note, none of the participants were involved in other therapies that may have impacted upper limb function, but P10 did start a handball program that very likely contributed to improvements on the QUEST and grip strength.
The above-described clinical outcomes compare well to previous studies using more costly haptic robotics. Following 9 hours of training with a haptic robot, Fluet et al. reported that 3 of the 9 children showed improvements in upper limb function beyond the minimal detectable change on the Melbourne Assessment of Unilateral Upper Limb Function [9]. Rostami et al. reported positive clinical outcomes in a study of 8 children with CP using the E-link exerciser for 18 hours over 4 weeks [8]. Direct comparisons are difficult given the different outcome measures and reporting used.
Challenges and opportunities
Research into gaming systems for upper limb rehabilitation is widespread, but most do not support haptic feedback and other task parameters that might improve motor learning and transference of skills practiced in a virtual environment to real-world function [7]. Systems that can provide variable haptic feedback tend to be prohibitively expensive which limits widespread clinical use and home applications. This study provides preliminary data showing that positive clinical outcomes can be achieved through interactive computer play with haptic feedback in a clinic setting by adapting relatively low-cost (
Studies such as this may serve an important purpose in spreading awareness among industry players of the potential value of their products outside of the entertainment gaming sphere. Engaging industry players to consider rehabilitation applications in the design of and distribution of their devices is one potential avenue to making these systems more cost-effective and available. This study also emphasizes the potential importance and value of including haptic feedback in addition to movement-tracking into the design of therapeutic gaming technologies for rehabilitation of the upper limb/hand.
Limitations
This case series represents an initial step in examining the clinical acceptability and effectiveness of a low-cost therapy gaming station with haptic feedback. While the results are promising, our sample size is small. Our sample is however quite diverse level of manual ability, age, and gender, making the sample representative of our target population. We acknowledge that it is possible that additional activities outside of the intervention may have impacted functional outcomes. However, we believe the extent of practice achieved with the Falcon gaming station had an important role in building skills that may have translated to improvements in everyday function. Finally, the amount of movements performed at the elbow and shoulder was restricted as the Novint Falcon only allowed movements on the X and Y-axes of 3.5 cm from the center. While the range of motion required was limited, the elbow/shoulder games required significant motor control and the weight-bearing and variable resistance associated with the activity was observed to challenge children’s endurance. Moreover, as children living with CP have less movement dissociation [32], therapists encouraged children to focus on dissociating shoulder and elbow movements during game play.
Author contributions
CONCEPTION: Elaine Biddiss and Jean-Sébastien Roy
PERFORMANCE OF WORK: Hamilton Hernandez, Isabelle Poitras, Linda Fay and Ajmal Khan
INTERPRETATION OR ANALYSIS OF DATA: Hamilton Hernandez, Isabelle Poitras and Ajmal Khan
PREPARATION OF THE MANUSCRIPT: Hamilton Hernandez, Isabelle Poitras, Jean-Sébastien Roy and Elaine Biddiss
SUPERVISION: Elaine Biddiss and Jean-Sébastien Roy
Ethical considerations
Approval was granted by Research Ethics Boards at Holland Bloorview and by the sectorial rehabilitation and social integration research ethics committee of the CIUSSS-CN (Project #2015-547). All participants and caregivers gave written informed consent. The study protocol is registered on clinicaltrials.gov (NCT04298411).
Footnotes
Acknowledgments
The authors would like to thank all the children and therapists that participated in the research study. We would like to acknowledge summer student Rhianne Lopez for helping build the custom grips for the Falcon and additional supports, and Tara Joy Knibbe and Maritza Basaran for helping with the logistics of the study. This work was funded through the Ward Family Summer Student Research Program 2015, the 2014 Bloorview Research Institute–Université Laval Research Collaborative Catalyst Grant, and the Université Laval Research Chair in Cerebral Palsy–Bloorview Research Institute Collaborative Fellowship Award 2012 Postdoctoral Fellowship Award in Cerebral Palsy Competition, a Discovery Grant from the Natural Sciences and Engineering Council of Canada (371828–11), and the Early Researcher Award from The Ontario Ministry of Economic Development and Innovation and the Kimel Family Opportunities Fund through the Holland Bloorview Kids Rehabilitation Hospital Foundation. We would also like to acknowledge the support of the Canadian Institutes of Health Research and the Natural Sciences and Engineering Research Council of Canada through a Collaborative Health and Research Project (FRN: 140195).
Conflict of interest
No conflict of interest exists.
Appendix
Game descriptions
Wrist extension games
Crazy Rider (MoPower, Google Play)
Goal: to reach the end of the level avoiding obstacles (trees, rocks, birds) and cliffs.
To play: Press and hold the red button to accelerate, and move the Falcon’s handle up and down to jump.
Lil Mads and the Gold Skull (Haus, R., Chrome Store)
Goal: to reach the end of the level avoiding obstacles (boxes) and cliffs.
To play: Move the Falcon’s handle up and down to jump.
Swoop (PlayCanvas, Google Play)
Goal: to keep the plane flying for as long as possible. Catch as many diamonds as possible to refill the plane’s fuel and avoid obstacles in the air.
To play: Move the Falcon’s handle up to elevate the plane and move it down to let it fall.
Funky Karts (Games, Y. Google Play)
Goal: to reach the end of the level collecting as many coins as possible and avoiding falling on spikes and cliffs.
To play: The kart always accelerates on its own. It can climb walls and the ceiling when it has momentum. Move the Falcon’s handle up and down to jump off the ground, the walls or the ceiling.
Elbow/shoulder games
Heroes of the Loot (Orange Pixel, Chrome Store)
Goal: to navigate a dungeon collecting as many treasures as possible while keeping monsters at bay. Some doors in the dungeon require a key that can be found in other rooms of the dungeon.
To play: Move the Falcon’s handle up, down, left or right to navigate the dungeon with the character. And press and hold the red button to attack surrounding monsters without a need to aim at them.
Save the Day (Ekaterischerbakova, Chrome Store)
Goal: to save as many people from the disaster zone as possible.
To play: Move the Falcon’s handle up, down, left or right to move the helicopter in the desired direction. Touch the characters calling for help with the helicopter to rescue them. Once you have loaded 10 passengers, you have to unload them in one of the safe platforms.
Position the helicopter in front of a fire and press and hold the red button to throw water and turn off the fire which will leave additional treasures to collect. Some areas unlock when the player has saved a determined number of people.
Bird Brawl (BattleSmart Studios)
Goal: to gather as many eggs as possible. To play: Move the Falcon’s handle up, down, left or right to move the character in the desired direction. Press and hold the red button to attack enemies in front of the character and find hidden eggs.
Pacman (BANDAI NAMCO Entertainment America, Google Play)
Goal: to clear up as many levels as possible.
To play: Move the Falcon’s handle up, down, left or right to move the character in the desired direction, running away from the ghosts and eating all the dots in the level. Eat the big dots to make the ghost edible for a short time.
Looney Tunes Dash (Softonic)
Goal: to escape from Angry Sam and get home avoiding obstacles in the track.
To play: Move the Falcon’s handle left or right to change lanes, up to jump a hole or an obstacle, and down to slide down and avoid being hit on the head.