
Abstract
BACKGROUND:
People with severe to profound intellectual disabilities and visual or motor impairment tend to be detached and sedentary.
OBJECTIVE:
The present study assessed a technology-aided intervention to promote ambulation in four people with severe to profound intellectual disability combined with blindness or deafness and spasticity.
METHOD:
The intervention was introduced according to a non-concurrent multiple baseline design across participants. The participants wore a smartphone fitted with the MacroDroid application at their right or left ankle. This application served to (a) detect and record smartphone’s shake events (i.e., events related to the step responses the participant performed with the leg to which the smartphone was fixed) throughout the study, and (b) automatically deliver stimulation and encouragements/prompts (i.e., in relation to step responses and lack of responding, respectively) during the intervention.
RESULTS:
Data showed that during the baseline (i.e., prior to the intervention) the participants’ mean frequency of step responses were between 26 and 61 per 5-min session. During the intervention the mean session frequency increased to between 100 and 157. The increase was statistically significant for all participants.
CONCLUSION:
The aforementioned technology-aided intervention may be a useful tool for promoting ambulation in people like those involved in this study.
Introduction
People with severe or profound intellectual disabilities often present with serious communication and occupational problems, which limit their opportunities of interaction with their caregivers and other possible communication partners and also prevent them from developing an active and functional role within their daily context [1, 2, 3, 4]. The possible presence of blindness or motor impairment complicates the situation of these people further and can lead them to a very detached and sedentary life [5, 6]. In effect, they may fail to engage in activities and/or simple ambulation unless prompted and guided by staff or caregivers [7, 8].
This situation is undoubtedly deleterious and needs to be addressed for the psychological, social, and physical well-being of the people [9, 10, 11]. Accordingly, programs have been developed to promote their activity engagement through the support of various technology aids [12, 13, 14].
Programs have also been developed to promote ambulation. For example, Lancioni et al. [15, 16] and Stasolla et al. [17] reported programs aimed at fostering ambulation with physical support in people with multiple disabilities (i.e., intellectual disabilities and motor or sensory-motor impairments). Their programs were based on the use of (a) walkers to ensure the physical support the participants required as well as (b) microswitches (sensors) to monitor the participants’ step responses and trigger a computer or other electronic device to providing stimulation in relation to those responses.
Lancioni et al. [18, 19, 20] reported programs aimed at promoting basic forms of independent ambulation (i.e., ambulation free of walkers or other support devices) through the use of automatically regulated stimulation events. In particular, optic sensors linked to an electronic control device could be used (a) at specific distances from one another (e.g., 0.5 or 1.0 m) on the wall of a corridor/room along which the participant was to walk or (b) on the participant’s shoes. In the first case, a sensor was activated as soon as the participant passed by the area where the sensor was located. In the second case, a sensor was activated as soon as the participant performed a step response. Activating a sensor led to the occurrence of stimulation events of different lengths that the participants were known to enjoy.
The aforementioned intervention programs aimed at fostering supported and independent ambulation provided fairly encouraging data (with the participants increasing the number of step responses performed during the intervention sessions and/or reducing the time required to walk preset distances). Notwithstanding the encouraging data, no definite statements can be made about the programs, as only few participants were included in the evaluations. This study was aimed at extending the evidence available in the area by (a) exposing new participants with intellectual and sensory or sensory-motor disabilities to intervention and (b) setting up an intervention program based on the use of everyday technology. Specifically, a smartphone with the MacroDroid application was used in combination with mini speakers or a tablet (see below) for monitoring the participants’ step responses and providing them with preferred stimulation and possibly encouragements/prompts.
Method
Participants
Four adult participants were included in the study. Table 1 lists them by their pseudonyms, and provides their chronological ages, sensory and motor impairments, and age equivalents for their daily living skills (i.e., personal subdomain) as measured via the second edition of the Vineland Adaptive Behavior Scales [21, 22]. Three participants presented with intellectual disability, blindness, and typical hearing (i.e., Casper, Logan, and Gavin). The fourth participant (Karin) had typical vision, but presented with intellectual disability, deafness, and spasticity, which made her require the support of a walker to ambulate. They attended rehabilitation and care centers. The psychological services of those centers had estimated their level of intellectual disability to be in the severe to profound range. Yet, no formal testing had been carried out with them given their conditions. The Vineland age equivalents for their daily living skills (personal subdomain) varied between below 1 year (Karin) and 2 years (Logan).
Participants’ pseudonyms, chronological age, sensory and motor impairments, and Vineland age equivalents for Daily Living Skills:
Personal Sub-domain (DLSP)
Participants’ pseudonyms, chronological age, sensory and motor impairments, and Vineland age equivalents for Daily Living Skills: Personal Sub-domain (DLSP)
The participants were included in the study based on the following criteria, which had been verified through preliminary staff interviews. First, ambulation (which required the help of a walker for Karin) was considered to be beneficial for all participants. Second, the participants were known to be largely sedentary and to ambulate for only short distances and with recurrent interruptions (i.e., when staff personnel asked them to do it by following a wall or using a walker). Third, the participants were known to enjoy forms of environmental stimulation such as music and verbal attention/praise from staff (first three participants) and videos of comedy sketches or of staff and family (fourth participant). Thus, it was thought that these forms of stimulation could serve as motivating events for their ambulation. Fourth, staff personnel, who were informed about the technology-aided intervention set up for this study, had expressed their support for it.
Given their conditions, the participants could not read and sign consent forms for the study. Thus, their legal representatives fulfilled such a requirement on their behalf. They were however informed about the study procedure and asked for their informal consent before the study took place. Informal consent was collected by the staff personell of the rehabilitation and care centers attended by the participants. The study complied with the 1964 Helsinki Declaration and its later amendments and was approved by an institutional Ethics Committee.
The participants used hallways within the centers that they attended as the setting for the baseline and intervention sessions. All sessions lasted 5 min. For each of the first three participants, the sessions began with the research assistant (a) accompanying the participant to the start area of a hallway (and for two of the three, giving the participant an object to transport), (b) placing the participant’s hand on the corridor’s wall or on the rail fixed to the wall, and (c) verbally and physically prompting the participant to walk. For the fourth participant, the sessions began with the research assistant (a) placing the participant in the walker at the start of the hallway, and (b) physically prompting her to walk. Research assistants, who were responsible for implementing the sessions and recording part of the data (see below), were familiar with people with intellectual and multiple disabilities and the use of technology-aided programs.
Measures and stimuli
The measures recorded during the sessions involved the (a) number of step responses, (b) number of smartphone’s verbal encouragements/prompts (i.e., only for the first three participants), and (c) number of verbal and physical prompts from the research assistant. The first two measures were recorded automatically via the MacroDroid application of the smartphone that the participants wore at the ankle of the right or left leg (see below). Regarding the first measure, MacroDroid recorded the number of smartphone’s shake events (i.e., events reflecting the step responses the participant performed with the leg to which the smartphone was fixed). Such number was then multiplied by 2 to (a) also include the step responses performed with the other leg and thus (b) determine the total frequency of responses occurred in the session. The third measure was recorded by the research assistants. To check interrater agreement on this measure, a reliability observer watched videos of more than 20% of the sessions of the single participants. The percentage of agreement was computed by dividing the number of sessions, in which the same number of prompts (which could also be zero) was reported by the research assistant and reliability observer, by the total number of sessions in which the two joined in recording the data, and multiplying by 100%. The percentages were above 95 for all participants.
The stimuli selected for the first three participants involved music, songs, chimes, and verbal attention/praise. The stimuli selected for the fourth participant involved videos containing film segments, comedy sketches, and staff/family scenes. The stimuli, which had been recommended by staff, were exposed to a preference screening procedure. The screening consisted of presenting at least 10 nonconsecutive times each of two 5- to 10-s segments of (a) the single pieces of music, chimes, and songs possibly combined with praise expressions (first three participants) or (b) the single videos (fourth participant). Stimuli were selected for the study if the research assistant and staff member carrying out the screening agreed that the participants had positive reactions (e.g., alerting, orienting or smiling) during 50% or more of their presentations.
Technology
The technology used for the first three participants included a Samsung Galaxy A10 smartphone with Android 10.0 operating system. The smartphone was fixed to the participant’s right or left leg (i.e., at the ankle level; see Fig. 1), and was (a) fitted with the MacroDroid application, (b) provided with a variety of audio files, and (c) linked via Bluetooth to mini speakers. The audio files involved (a) the stimuli selected as preferred for the single participants (e.g., songs and other melodies combined with praise recordings), and (b) verbal encouragements/prompts. During baseline sessions, the MacroDroid was set up to monitor and record the smartphone’s shake events (i.e., events connected to the participant’s step responses performed with the leg to which the smartphone was fixed). During the intervention sessions, the MacroDroid also ensured the delivery of (a) 3 or 4 s of preferred stimulation in relation to each of the shake events (i.e., step responses recorded) and (b) encouragements/prompts (i.e., one- to three-word expressions typically used by regular staff) after 20 s without step responses. The stimulation and encouragements/prompts were delivered via the mini speakers located in different positions of the hallway (see below).
The diagram shows the position of the smartphone on the participant’s leg.
The technology used for the fourth participant (Karin) included (a) the aforementioned smartphone and a tablet (i.e., Samsung Galaxy Table S2 with Android 10.0 operating system) both fitted with MacroDroid. The smartphone’s position and the MacroDroid’s functioning were the same as for the other participants during the baseline phase. During the intervention, the MacroDroid also served to trigger the tablet to display 3 or 4 s of preferred visual stimulation for each of the smartphone’s shake events (i.e., step responses recorded). No smartphone’s encouragements/prompts were available for her, as she was deaf.
A non-concurrent multiple baseline design across participants [23] was used to assess the effects of the intervention. The length of the baseline changed across participants (as required by the design). The baseline phase of a participant would not end if the participant’s frequency of step responses during the last session exceeded the values of previous sessions. To ensure procedural fidelity, a study coordinator supervised the work of the research assistants using video recordings of the sessions [24].
The baseline and intervention ambulation data (i.e., frequencies of step responses) of every participant were reported in graphic form. In order to simplify the graphic display, the data were summarized into blocks of sessions (i.e., each data point reported in the graphs represents a mean frequency value over a block of sessions). The Kolmogorov-Smirnov test [25] was used for each participant to determine whether the differences between the baseline and intervention step-response frequencies were statistically significant.
Baseline
Four to eight baseline sessions were carried out in the hallways of the centers that the participants attended. The participants wore the smartphone with the MacroDroid. The MacroDroid recorded smartphone’s shake events (i.e., step responses), but (a) did not provide stimulation or encouragements/prompts for the first three participants, and (b) did not trigger the tablet’s stimulation for the fourth participant. To start a session, the research assistant proceeded as described in the Setting, ambulation sessions, and research assistants section. The research assistant intervened with verbal and physical prompting if the participant performed no step responses for 30–40 s.
The four panels report the participants’ data for the baseline and intervention phases. The black squares represent mean frequencies of step responses per session computed over blocks of two sessions during the baseline and four sessions during the intervention. Blocks with different numbers of sessions (i.e., at the end of the intervention phase) are marked with a numeral that indicates how many sessions they include.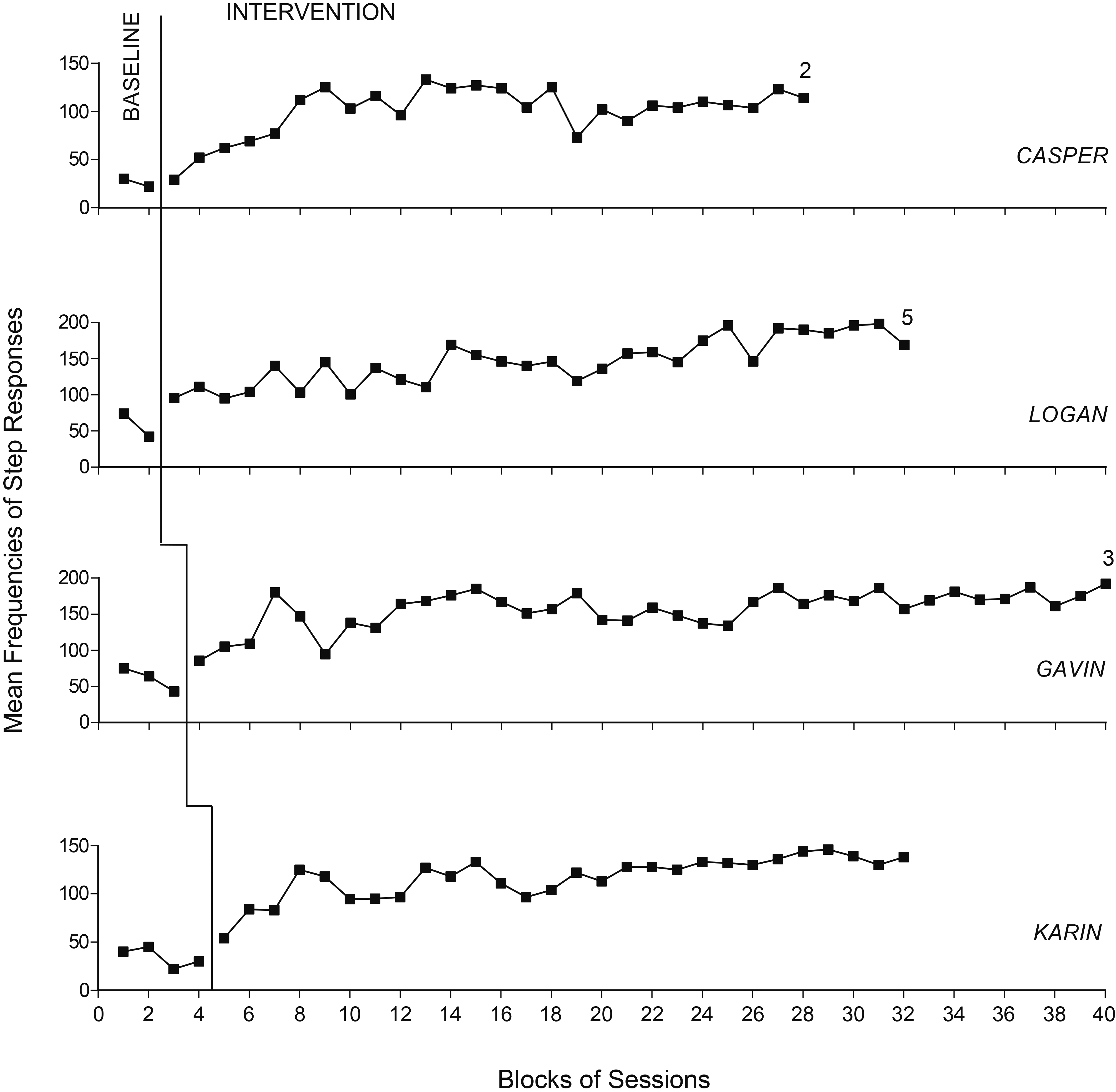
The 102 to 147 intervention sessions were carried out in the same hallways, which had been used during the baseline sessions. Conditions were as in baseline except that the technology was set up to provide stimulation contingent on the participant’s step responses performed with the leg to which the smartphone was fixed (all participants) and encouragements/prompts (first three participants). The auditory stimulation available for the first three participants was delivered via the two mini speakers linked to the smartphone via Bluetooth. They were placed at the opposite ends of the hallway (10–12 m apart) for Logan and Gavin and at halfway and near the end of the hallway (about 7 m apart) for Casper. At the start of the session, Logan and Gavin received stimulation from the speaker in front of them (i.e., located at the end section of the hallway that they were to reach). After a preset time, the MacroDroid triggered the smartphone to deactivate that speaker and activate the one located at the opposite end of the hallway (where the ambulation had started), so the participants would turn toward the stimulation and ambulate back. Eventually, it could revert the speaker activation so the participants turned again and walked in the same direction as at the start of the session. For Casper, the speakers worked as for the other two participants. Yet, the stimulation was initially delivered from the speaker halfway the hallway and then from the speaker near the end of the hallway. Smartphone’s encouragements/prompts occurred after 20 s had elapsed with no steps being recorded. Prompts from the research assistants would occur if the participants did not respond to the smartphone’s encouragements/prompts for about 20 s.
Karin received visual stimulation for her step responses through a tablet, which was mounted on the walker in front of her. No smartphone’ encouragements/prompts were available for her, as she was deaf. Research assistant’s prompts were available after about 30 s had elapsed with no steps being recorded.
Results
Figure 2 reports the participants’ ambulation data during the baseline and intervention phases. The black squares represent mean frequencies of step responses per session computed over blocks of two sessions during the baseline and four sessions during the intervention. Blocks with a different number of sessions (i.e., at the end of the intervention phase) are marked with a numeral that indicates how many sessions they include.
During the baseline phase, the participants’ mean frequency of step responses varied between 26 (Casper) and 61 (Gavin) per session. The mean frequency of prompts from the research assistants varied between slightly over 3 (Gavin) and about 7 (Casper) per session. During the intervention phase, the participants’ mean frequency of step responses varied between 100 (Casper) and 157 (Gavin) per session. After the initial 25 intervention sessions, the participants’ response frequency per session ranged between 58 (Casper) and 224 (Logan). The mean frequency of smartphone’s encouragements/prompts (i.e., for the first three participants) was around 0.5 per session. Prompts from the research assistants were fairly sporadic. The Kolmogorov-Smirnov test indicated that the difference between the baseline and intervention step-response frequencies was statistically significant (
Discussion
The data reported indicate that the intervention conditions were effective in increasing the ambulation behavior of all four participants. These results (a) extend the evidence available about the effectiveness of technology-based interventions for fostering ambulation in people with intellectual and multiple disabilities [17, 18, 20] and (b) add new evidence about the usability and effectiveness of everyday technology devices for supporting such interventions. In light of these results, a few considerations may be forwarded.
First, ambulation increase can be considered a valuable objective to pursue with people with intellectual and multiple disabilities, who tend to be sedentary and passive [26, 27]. Pursuing such an objective through an intervention approach largely based on technology support, and thus requiring only minimal staff supervision, can be viewed as practically and socially relevant. In fact, staff resources in rehabilitation and care centers are often limited and consequently staff could hardly afford to provide extensive supervision on a regular basis. Moreover, extensive staff supervision would emphasize the participants’ dependence and harm their social image [28, 29].
Second, an intervention approach based on the use of preferred stimulation contingent on step responses may be viewed as largely positive/motivating for the participants and easily acceptable for the context. Accordingly, the participants would be expected to have an increase in their frequency of step responses based on the pleasure connected to performing those responses (and the willingness to extend such an experience) more than on any other environmental variable [30, 31]. Although this enjoyment/satisfaction aspect was not documented, an indirect sign of its existence seemed to be the participants’ convincing ambulation performance throughout the intervention phase (i.e., a performance that required only few smartphone’s encouragements/prompts and rare prompting from the research assistants).
Third, while the positive stimulation may have been critical to determine the participants’ intervention data, the fact that the stimulation was delivered from specific spatial areas may have contributed to facilitate the orientation and sense of security of the first three participants [32, 33]. For Logan and Gavin, the alternating presentation of the stimulation at the two ends of the hallway after prearranged time intervals was apparently instrumental to allow them to walk in one direction and then in the other without difficulties, thus avoiding the need to use a very long hallway or to rely on staff guidance to turn (change direction).
Fourth, the technology used to support the participants’ ambulation was particularly simple, easy to access, and largely affordable [34, 35]. In reality, the first three participants only used a relatively inexpensive smartphone (Samsung Galaxi A10), which was fitted with MacroDroid and combined with two mini speakers. The fourth participant used a smartphone and a tablet both fitted with MacroDroid. While the technology is easily accessible, some attention is required to set it up for the study. Setting it up implies (a) storing auditory files in the smartphone and visual files in the tablet, and (b) programming the MacroDroid application. Such programming serves to make the MacroDroid (a) record the smartphone’s shake events (i.e., the participant’s step responses), (b) trigger the smartphone’s delivery of auditory stimulation or the tablet’s delivery of visual stimulation in relation to the step responses recorded, and (c) trigger the smartphone’s presentation of encouragements/prompts in case of no responding for a preset period of time.
Study limitations and conclusion
One limitation of the study is the small number of participants included. Moreover, the last participant presented clear differences compared to the first three. New research with additional participants (some comparable to the first three participants and others to the last participant) would be needed to determine the robustness of the technology and appropriateness of its arrangement during the intervention phase [36, 37]. A second limitation concerns the fact that the participants’ enjoyment/satisfaction during the intervention sessions was not assessed. This assessment could be important to ascertain whether the stimulation available for the step responses was the critical variable motivating the participants’ responding by making them satisfied of (happy about) the intervention conditions [38]. A third limitation is that no check was made of whether the smartphone could be placed in a position other than the participant’s ankle so as to ensure that even people not tolerating the smartphone at their ankle could be involved in the intervention process. Conceivably, smartphone’s shake events can be produced by step responses even if the smartphone is placed in a pocket attached to the side of the participants’ pants at the calf or knee level. A fourth limitation is the absence of a social validation of the technology used. A social validation involving staff personnel as well as family members as raters would be crucial to find out their opinion about the technology’s potential as well as about the technology’s acceptability within daily contexts [39, 40].
In conclusion, the results obtained in this study suggest that everyday technology could be successfully used to increase the participants’ ambulation level and thus might represent a practical tool within contexts for people with intellectual and multiple disabilities. Notwithstanding the positive results reported, caution is required in drawing conclusions given the limitations of the study mentioned above. New research will have to address those limitations and possibly upgrade the technology to improve its usability with participants with different needs and characteristics.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors report no conflicts of interest.
Ethical considerations
The study was approved by an institutional Ethics Committee. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The participants’ legal representatives provided written informed consent for the participants’ involvement in the study.