
Abstract
BACKGROUND:
Autism Spectrum Disorder (ASD) is characterized by difficulties in social communication, social interactions, and repetitive behaviors. The earlier the diagnosis, the sooner the intervention therapy can begin, thus, making early diagnosis an important research goal. Technological innovations have tremendous potential to assist with early diagnosis and improve intervention programs. There is a limited understanding of the Wearable Technologies (WTs) currently available for autistic individuals, and how they measure functioning in this population.
OBJECTIVE:
The aim of this review is to identify advancement in wearable technologies used to monitor behavioral and physiological responses in the intervention of children with ASD.
METHODS:
A literature search was performed for English language articles and conference papers indexed in Science direct, PubMed, Web of science, Google scholar, ERIC, ProQuest and Cochrane in last five years (2017–2021), resulting in eighteen studies being reviewed.
RESULTS:
Wearable technology present a potential solution that can support and complement existing interventions. WTs measured a range of physiological and behavioural functions to objectively measure stereotypical motor movements, social function, communication, and emotion regulation in autistic youth in the context of a range of environments and activities.
CONCLUSIONS:
Advancement in technology that include behavioral and physiological response monitoring with wearable sensors provide the opportunity to acquire new understanding of the internal components of observable behavior of children with ASD. This could lead to better individualization of treatment and greater treatment effectiveness.
Keywords
Introduction
Autism Spectrum Disorders (ASD) is a common lifelong neurodevelopmental condition, characterized by qualitative impairments in social communication and interaction, engagement in rituals and routines, and hypo- or hyper-sensory sensitivities [1]. The symptoms normally appear by the age of three. Apart from impairments in the social domain, where the autonomic nervous system seems to play an important role, other autistic characteristics include a limited range of interests combined with rigid and restricted or repetitive behaviors (stereotypes). Some of the main communication deficits may include inconsistent eye contact, being slow or failing to respond to someone, talking about a favorite subject without noticing that others are not interested, having an unusual tone of voice, and being unable to understand other people’s actions. Children with ASD very often become upset by slight changes in their routine, as well as extreme sensory input (e.g., noise, light, etc.) from the environment [2].
There is a lack of appropriate expression specifically when children with ASD need to be involved in the assessment process, intervention, therapy, and remedial sessions. It takes very long to develop rapport with them. Many a time they missed out to tell important information about their feelings and emotions. Children with ASD often have difficulties understanding and recognizing their emotions, therefore making it difficult to infer when they are experiencing stress or social anxiety [3]. Information on the physiological state is very important as the physiological state of the body is strongly related to the emotional state of the child [4, 5]. The human body has multiple physiological responses that can be measured from electrical signs to biochemical, human biosignals are possible to be extracted and be used to better understand the bodily health status and reaction to external factors [9].
The physiological state of arousal is achieved by changes within the autonomic nervous system (ANS) functioning. ANS is part of the nervous system that controls our involuntary actions. The sympathetic and parasympathetic nervous systems behave independently and sometimes cooperatively in their functions. A way to describe their functions is that the parasympathetic produces responses to promote restoration and conservation of energy while the sympathetic nervous system is concerned with making the body ready to deal with external threats or dangers. Increased activity in the sympathetic nervous system elevates heart rate, blood pressure, and sweating, as well as sending blood toward skeletal muscles, lungs, heart, and brain to help the body’s motor action. Increased understanding of these responses will revolutionize the field of affective computing by providing the tools needed in developing physiological and behavioral measures to classify symptoms of emotional states such as autism spectrum disorder (ASD), depression, anxiety disorders, and personality disorders [32].
Physiological responses could be an effective medium to provide an insight into the child during the assessment or intervention process. Advancements in health monitoring have allowed for the development of external wearable systems, capable of unobtrusively capturing behavioral and physiological data in real-time. These systems, referred to as ‘wearable technology’ (WT) are devices worn externally, with built-in electronic functions utilized during activity. Common WTs include fitness and activity trackers, smartwatches, and smart glasses, which measure a range of physiological and behavioral functions including heart rate, skin conductance, and eye gaze, among others [7]. Nuske et al. emphasized on identification and understanding of triggers to recognize stressful events and manage and minimize challenging behaviors [8]. Advancement in technologies may show promise in expanding opportunities to improve understanding of clinical conditions and through providing a means to continuously measure and monitor daily life functioning, may contribute novel individualized intervention and treatment [9].
Wearable technologies can assist parents as well as children in targeting functional issues like social communication, behavior, and sensitivities and providing a path to independence. These are portable advanced devices in terms of technology, size, functionality, and real-time applications. The emergence and low cost of new mobile devices have dramatically changed how service providers deliver educational and behavioral services to individuals with ASD. Nowadays, smartwatches and other wearables have enough processing power and memory to assist children with ASD. The minimalism and comfort of these wearables (e.g., wearing on the wrist) make them accessible at any time and anywhere and protect children from losing them. Another important feature of wearables is the option of using different materials that may work best with the individual sensory needs of the child. Moreover, the collection of health data from the integrated sensors can help in monitoring and controlling the subject as needed (e.g., in stressful situations or natural environments) [2, 22]. Wearable devices increase wearers’ awareness and help manage their behaviors [24].
At present Technological advancement is evolving constantly and various technology-based applications are being used for assessment and interventions for children with ASD. This review explored the use of wearable technologies for monitoring behavioral and physiological responses in children with ASD. The present review aims to systematically gather the empirical data regarding technological advancement in monitoring behavioral and physiological responses for children with Autism Spectrum Disorder Across various contexts. This may elucidate psychological stress and social anxiety during the intervention and the importance of monitoring of physiological responses with implications for prevention, early intervention, and development of more targeted interventions. The current study reviews the literature to identify current trends, prospects, and possible gaps related to wearable technologies in children with ASD. This review sought to answer the following questions:
What wearable technology devices are available that can be used for children with ASD to monitor behavioral and physiological responses? Which behavioral and physiological parameters are detectable through wearable sensors? How are autonomic responses associated with psychological stress and emotional regulation? Does monitoring of physiological responses through wearable technology provide insight to professionals?
Design
A systematic review exploring and synthesizing the literature examining the efficacy of WTs assessing function in children with ASD during intervention was undertaken.
Search strategy
An extensive literature search was performed using keywords “Autism Spectrum Disorder”, “Physiological responses”, “Autonomic responses”, “wearable technology”, “human activity monitoring”, “wearable sensors”, “Behavior”. We searched seven databases including Science Direct, PubMed, Web of Science, Google Scholar, ERIC, ProQuest, and Cochrane for studies published in the last five years (2017–2021). Details of the database searched, and yield reports are provided in Table 1.
Searched database and yield reports
Searched database and yield reports
Inclusion criteria were: 1) English Language Articles, published in peer-reviewed journals describing empirical research; 2) studies examining the use of wearable technology to monitor physiological responses during/as intervention; 3) studies focusing on children, adolescents, or adults diagnosed with any subtype of ASD, with or without a concurrent intellectual disability (ID) and irrespective as to whether participants had or were receiving treatment at the time of research participation; 4) studies that were peer-reviewed full-text articles or detailed abstracts published within the last 5 years. We excluded 1) studies that did not include children or adolescents with Autism Spectrum Disorder (ASD); 2) studies that did not use wearable technology-based therapies for monitoring physiological parameters; 3) books or book chapters, review papers, or grey literature (except for conference proceedings); 4) studies that did not report outcomes on patients. Subsequently, a concordant list of studies meeting inclusion criteria was developed.
Studies selection flow diagram.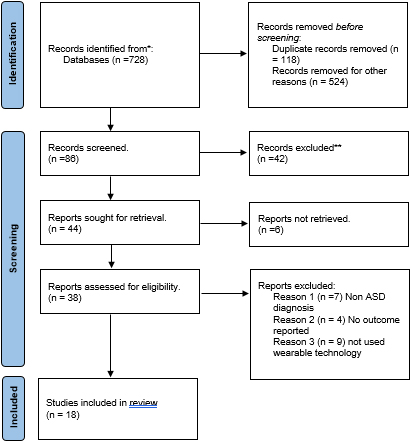
Figure 1 provides an overview of study selection. The database searches initially yielded 728 reports. Duplicates (
The first author searched the literature and reviewed the studies under the guidance of other authors. Data were verified for accuracy and completeness by the other authors. The screening process consisted of a title and abstract screening as well as a full-text screening. If a study met all predefined eligibility criteria, it was included in the review.
Data extraction
We extracted and tabulated data about the study design; sampling frame; sample size; participant demographics in clinical and comparator groups; outcome measures employed; WT and physiological parameters studied; study results; and methodological considerations.
Analysis plan
Although there was some overlap in outcome measures used, studies were methodologically heterogeneous and clinically heterogeneous (including participants across the lifespan). Data were therefore analyzed using a narrative rather than a meta-analytic approach.
Results
All included studies were scientific studies analyzing the effect of wearable technology devices as an intervention or a monitoring device to improve and measure different outcomes in children and adolescents with ASD. They were published in English between 2017–2021.
In total, 18 studies were included in this review (see Table 2). Ten of the included studies were conducted in a Clinical/Laboratory setting, while six studies were conducted in a school/classroom setting. Home settings were used in three studies and only one study used classroom and outside classroom context considering the data collection in a natural setting.
There is a great variation in the ages of children with autism involved in the studies. Three studies involved children from 3 months old high risk infants to 5 years. Seven studies involved children within the age range of 6–12 years. Six studies focused on the age group of 13–19 years and two studies involved college-going youth from age 19–22 years.
Studies selected for the review used varied study designs. Eight were randomized control trials. Six of them were case series. Two studies were single-subject studies. One study was a longitudinal study and one was a clinical assessment study. Most of the studies include both the gender (M/F) of children with ASD. One study included one girl with ASD, and one study included only male participants.
Summary of information for all studies included in the review (
18)
Summary of information for all studies included in the review (
The wearable technology (WTs) used were grouped in two categories: 1) head-mounted devices, 2) accessory or body-worn devices.
Head-mounted devices
A variety of head-mounted devices were described, including glasses or devices worn in the form of a headband. These WTs were used to gather data such as head orientation, gaze patterns, facial engagement, emotion recognition, and direct interaction.
Smart or assistive reality glasses were discussed by six studies (see Table 1). These features of glasses were, an outward-facing camera capturing the faces of others, and an inward-facing tracker monitoring the wearer’s eye gaze patterns and was capable of providing youth with real-time feedback on their social function through providing audio or visual feedback. Several systems utilizing smart glass technology were presented to support and improve social communication and interaction in children with ASD.
A study used superpower glass intervention, a wearable social learning aid for children with ASD to encourage facial engagement and provide feedback to the child during social interactions at home. A computer vision system runs on Google Glass that is wirelessly connected to a smartphone app to provide the intervention to the child wearing the glasses [13]. Another pilot study evaluated the potential of the Superpower Glass prototype as a wearable therapy intervention that increases social skills, facial affect recognition, and eye contact for children with autism between the ages of 3 and 17 years [10]. Daniels J et al created software capable of running on Google Glass and designed to give preprogrammed emotion-feedback cues to the wearer [11]. A study introduced the wearable device with infrared (IR) communication, called FaceLooks, which quantifies face-to-face behavior. This smart sensor device was worn on the forehead like a headband and emits light to visually represent real-time face-to-face behavior [28]. A similar concept was employed by Hurwitz S. et al. by using Video Recording Glasses. During the conversations, both conversational partners (i.e., participants and interventionists) wore special glasses that contained a small camera in the bridge. These glasses captured video and audio using direct first-person point-of-view (PoV) wearable and wireless video cameras (Pivothead, Denver, CO). During conversations, the glasses recorded what each person saw and said from the viewpoint of the person wearing the glasses (i.e., two videos were recorded during each conversation, one from the perspective of the participant and one from the interventionist) [27]. Another study used the Empowered Brain, an assistive technology tool designed to help improve social communication in children and adults with ASD. The user wore the smart glasses and participates in a semi-structured interaction with a facilitator. Smart glasses provide users with pro-social cues and guidance by visual and auditory feedback delivered through the optical display and speaker [20].
Overall, studies investigating smart glasses suggested that they were generally tolerated by autistic youth, and were perceived as useable [10, 11, 13] and enjoyable [20, 28]. Some studies, however, reported that smart glasses may become uncomfortable if worn for long periods, or become too warm [27]. When examining the potential for negative effects, evidence was found suggesting that a small number of participants experienced mild adverse effects including dizziness, nose-bridge discomfort, and eye strain [27].
Accessory or body-worn devices
Accessory included wrist-worn devices [12, 15, 16, 17, 21, 23] and sensorised clothes [25]. Wrist-worn devices were examined in six studies (Table 1). These devices measured physiological signals and functional parameters including touch [23], heart rate [12, 23], and electrodermal activity (EDA) [16, 17].
One study used a smart watch for directive-following and anticipatory directive-following responses during the intervention [23]. Another study used a smartwatch to evaluate the heart rate as high values of heart rate in these children with ASD are more likely to be caused by a stress or temper episode. Moreover, as these episodes are emotional, changes in heart rate are remarkable quantitatively [12]. A study by Goodwin in 2019 recorded peripheral physiological (cardiovascular and electrodermal activity) and motion (accelerometry) signals from a biosensor worn on the wrist [17]. Participants wore a bracelet for wireless EDA recording for the measurement of anxiety levels [16]. Another study utilized wearable sensors for leg movement data collection from five high-risk infants at 3, 6, 9, and 12 months of age. The protocol included visitation of infants each morning in their home environment intending to collect full-day movement data. The wearable sensors were placed on the infants’ ankles and were attached using legwarmers. Each ankle legwarmer contains a pocket to hold the wearable sensor in place [25].
Another study by Suarez used electrodermal activity data collection during laboratory food presentation protocol using Biopac System software. Electrodes were placed on the thenar, and hypothenar eminences of the participant’s non-dominant hand and data was collected with a wireless transmitter using a constant voltage (0.5V) technique [18]. Another study by Sasikumar also used photoplethysmography (PPG) and the galvanic skin response (GSR) signals during mental tasks through clue cards with visuals like alphabets, numbers, fruits, colors, and animals. Physiological signals processed, and dicrotic notch, heart rate, and EDA response feature were extracted from the acquired signals [30].
Body-worn technologies included sensors placed on the body, such as accelerometers, electromyography sensors, and chest belts or sensors. Four articles (Table 1) investigated the use of accelerometers to measure and classify stereotypical motor movements such as body rocking and flapping [14, 15, 17, 21] with two studies also investigating accelerometers to detect emotional self-regulation behavior [12, 21]. Few studies also used accelerometers to detect stereotypical movement and motion during the task [14, 15].
Wearable sensors to record ECG signals and to provide markers for ANS response were used by three studies [14, 19, 29]. Electrocardiography (ECG) signals were recorded during an eye-tracking joint attention task in toddlers and attention to the stimuli was assured by the simultaneous acquisition of eye-tracking and ECG data. The ECG sensor was modified by adding two pins to allow its interfacing with the common PolarTM cardio-fitness chest strap, featuring two dry electrodes in the inner side of the strap, interfaced to the skin surface of the subject for a single-lead acquisition [29]. Another wearable sensor device used was a low-cost system that integrated a three-lead electrocardiograph (ECG) sensor for cardiac activity monitoring and feasibility testing suggested that the use of chest-belt to measure ECG in a semi naturalistic context may enable real-time tracking of engagement and autonomic nervous system activity [14, 19]. Despite some limitations, including children’s tolerability of the device and comfort, the device effectively measured proximity, was useable in everyday life, and resulted in autistic children modifying their proximity to others appropriately [14, 29].
Behavioral and autonomic responses detectable through wearable sensors
Since autism is a disorder on a wide spectrum, a variety of traits have been found to characterize the condition, and hence the same variety can be found in its sensing devices as well. These devices vary largely not just in size, but also in appearance, design, purpose, and the parameters they measure [6]. The physiological and behavioral parameters notices in this review are as follows:
Eye trackers
Individuals diagnosed with ASD have been observed to exhibit different gaze patterns that are evident as they look at socially salient stimuli such as faces [10, 11, 13, 29]. This is a consequence of impaired social communication and interactive skills, where making eye contact is particularly challenging. It must be noted that the studies reported in this section were conducted in a naturalistic classroom or home setting [10, 13, 28] and clinical settings [11, 20, 27] which tends to provide more obvious results. Most of these studies were designed for early ASD screening, while some were aimed to facilitate intervention and improvement in social and emotional behaviors. Driven by the availability of general use eye gaze trackers either head-mounted or eye-tracking smart glasses, there are more contributions in this category as compared to others [6].
Motion detectors
Children with ASD are known to engage in stereotypical behaviors, which inhibit the development of appropriate social and adaptive behaviors and can turn into self-injurious activities [6]. A mechanism for detecting such behavior gives caregivers the opportunity for timely intervention. In most of the studies, the movement was tracked through an accelerometer [14, 15, 17, 25]. Accelerometers are devices that measure the acceleration of motion of a structure. With acceleration data being collected in the x, y, and z coordinates, these can be processed further to obtain velocity and displacement for time. Furthermore, the raw signals can be converted into machine learning methods to extract meaningful measures. As wearable devices, the sensors are required to be in physical contact with the subjects’ bodies either worn in a bodysuit or as a smart watch.
A study Utilized the wearable sensors, leg movement data collected from five HR infants at 3, 6, 9, and 12 months of age. The protocol included visitation of infants each morning in their home environment to collect full-day movement data. The wearable sensors were placed on the infants’ ankles and were attached using legwarmers. Each ankle legwarmer contains a pocket to hold the wearable sensor in place. Using the full-day movement data derived from the sensor, a novel motion complexity measure was constructed. A minimally complex movement pattern is one fully described by a singular periodic function [25].
Heart rate (HR) and Heart rate variability (HRV)
Heart rate (HR) is a measure of the number of beats per minute and can be used for monitoring the cardiovascular activity of the heart. However, heart rate gives limited information about heart activity. A more useful measure is called heart rate variability (HRV) which calculates the time intervals between two consecutive R peaks in the ECG signal is measured from an ECG sensor. The gold standard for measuring and calculating HRV is typically used is which is widely recognized and used by physiology researchers and clinicians [34]. However, in the recent developments of wearable devices, a new class of devices that measure heart rate and heart rate variability has emerged, using a photoplethysmography (PPG) sensor on wristbands. PPG sensor relies on a different principle the measurement of Blood Volume Pulse (BVP) to estimate the heart rate and approximated heart rate variability value. Although this seems to provide fairly accurate heart rate measurements, its heart rate variability recording is not as accurate as an ECG sensor and the decision to trust HRV analysis using PPG depends on the parameter one intends to use [30].
The increased HR found in ASD children seems to confirm that they experience stress during all interactive activities, with a low capability to modulate the emotional response process. HR was more elevated and less modulated in children with ASD as compared to typically developing children [19].
Respiratory sinus arrhythmia
Another parameter that is closely related to Heart Rate Variability is Respiratory Sinus Arrhythmia (RSA). RSA can be defined as the heart rate variability in synchrony with respiration, by which the R-R interval on an ECG signal is reduced during inhalation and increased during exhalation [35]. RSA reacts to stress or other emotional experiences and thus can be used to characterize anxiety disorder, by revealing information pertinent to the emotion regulation process. In addition, RSA changes as a function of the stressor. For instance, it has been reported that high resting RSA amplitude is associated with a greater withdrawal of stressors and subsequent recovery could represent a flexible and adaptive physiological response system to a challenge [29]. On the other hand, low resting RSA accompanied by an inadequate reactivity to stress could indicate an inappropriate regulatory mechanism. Along with this Respiratory rate can also be a stress indicator.
Electrodermal activity (EDA)
Electrodermal activity (EDA) is also called Galvanic Skin Response (GSR) measures the conductance of the skin. The utility of wearable devices is now extending beyond the goal to detect and assess complex behaviors in the autistic population. Wearable, unobtrusive sensors allow the measurement of physiological data over extended periods for continuous health monitoring. Electrodermal activity monitors may be able to estimate a child’s internal state through physiological signals that are related to sweat rates, blood volume pulse, heart rate, and skin temperature in real-time. It took the form of a chest strap, wristband, ankle band, and baby sock. The sensor data was made available across devices with a wireless communication network [6].
EDA is used as a measure of stress levels in humans. When a person experiences stress, moisture collects under the skin as a sympathetic nervous system response [12, 16, 18, 30]. The increased moisture level increases the electrical conductivity of the skin, which the skin conductance sensors utilize to determine the stress levels in a subject. The same EDA results may be obtained when a person experiences excitement, highlighting the need for context evaluation. These sensors allow others to get an insight into the internal states of subjects with ASD, who might otherwise find it difficult to communicate their feelings. Skin temperature measurement allows the elimination of environmental factors that may cause an increase in body temperature, which can improve the integrity of the result. Tracking the motion of a subject can be used to detect, analyze and preempt repetitive, stereotypical behaviors, allowing the therapist to reinforce functional replacement behaviors. This can prevent the child from engaging in these behaviors to the exclusion of more adaptive behaviors and decreases the likelihood that certain behaviors escalate to self-injury [6].
Blood volume pulse
Blood Volume Pulse (BVP) is measured using photoplethysmography (PPG) and indicates dynamic changes in blood volume underneath the sensor. The BVP signal indicates relative changes in the vascular bed due to vasodilation or vasoconstriction (increase or decrease in blood flow) as well as to changes in the elasticity of the vascular walls. BVP is commonly used to detect heart rate, heart rate variability, and relative blood volume. In the context of stress detection, research has shown features extracted from blood volume pulse can be used to detect stress [17, 33].
Association of autonomic responses with psychological stress and emotions regulation
Children with ASD have problems knowing and understand the emotions of people around them and have difficulty in trying to put across their feelings and emotions to people around them [32]. The physiological change gives several results related to the stress response that can be measured invasive method [14]. Physiological signal monitoring is one of the methods to predict the emotional status of autistic children; sometimes the collected information may not be apparent. It is exceptionally well in cases of children with autism because they are socially inept. For example, autistic children might sometimes smile when they underwent from pain. Children with autism might show no facial expression or a disinterested during the activity with peers [32]. ANS will play a major role in controls all activities of the 86 physiological and sympathetic and parasympathetic branches, adaptively respond to the situation [17]. The ANS is a typical response to anxiety and is associated with ASD consistently with overarousal [14]. The stress faced by the autism children is due to the failure to respond, understand and communicate with others of their peers makes them stressed their inability to express their emotions and needs given higher rates of the pulse. When a mental ability task is given to autistic children, due to the abnormality in the brain, they tend to drift from the task given to them, and they are unable to concentrate on one thing at a time. They tend to get tensed and stressed out as compared to control children, which shows the increase in the ANS activity more predominantly, the Sympathetic Nervous System, and hen the heart rate increases [30].
Furthermore, Nuske et al. reported that HR may predict challenging behavior in children with ASD and support difficulties in communication [1]. The HR measurement device is a non-invasive and painless objective measure of stress in preschoolers with ASD. This device seems to be particularly useful since most subjects with ASD cannot recognize and express external and internal symptoms of stress. Furthermore, HR monitoring appears to be a reliable method to test ANS functionality in children with other neurodevelopmental disorders and psychiatric conditions (such as anxiety or depressive disorders) [19].
Heart rate variability, as an important physiological biomarker, provides deep insights for the clarification of the relationship between psychological and physiological processes [34]. People with ASD exhibit heightened cardiovascular arousal even without the apparent presence of a stressor [17].
Emotional dysregulation entails a meaningful impact on the long-term quality of life of people with ASD. Anxiety, depression, explosive behaviors, and inadaptability are common effects on these individuals if untreated. Inability to manage and recognize their own emotions is what leads to these difficulties. It is called alexithymia, and recent technology products in the literature are meant to address this characteristic of individuals with ASD, in as much as their inner state can be read in alternative ways (physiological signals, facial expressions) and proper intervention might be provided [12].
A study finding included the differences in tonic EDA during food presentation in children with ASD compared to children who were typically developing and the relationship between tonic EDA. It provided some possible insight into the arousal level of the children during this eating activity [18].
Wearable therapy interventions like google glass, head-mounted smart bands, and smartwatches for children with autism showed significant improvement in social skills, facial affect recognition, facial engagement, and eye contact, directly associated with self-emotional regulation and self-monitoring, social responsiveness, and communication skills. Wearable technology is also used in many studies for the detection of stress, anger, anxiety, emotion, arousal, and social engagement.
A study compared the motion complexity scores of five infants. The difference in motion complexity scores between the infants was noted as early as three months of age and was observed for all the motor time points. Positive correlations between higher motion complexity scores and higher cognitive ability and adaptive skills were noted at 36-month outcome assessments, but this was not consistent across all time points [25]. Acquiring a child’s internal state could prove useful especially to some of the children with ASD who are nonverbal. Like the movement-based trackers, the commercially available electrodermal activity monitors are wearable and lightweight.
Insight to professionals
People with ASD can exhibit different physiological response patterns compared with typically developing peers. The collection of physiological signals collected can aid in the process of medical diagnosis. However, many times the sensors used to collect physiological data are expensive and immobile with patients enduring some discomfort because of the intrusiveness of the sensors [32]. Self-monitoring has been used to address various problem behaviors in children with ASD.
The physiological signals will help not only the autistic children but also people around them to know for sure what they are going through or feeling at a point in time. Hence, there is a need to combine social stimuli and technology to create a system that can help individuals with ASD to lead a normal life. The physiological signals might be the input to the clinicians and choose the best therapeutic method that is effective towards the autistic children society [30].
The high interest in these wearable systems arises from the technology that makes this possible as well as the interest in research and medical monitoring for the need of monitoring patients over extended periods. Many researchers, as well as physicians, need to monitor individuals through personalized therapies, where the treatment can adapt to a person’s affective state. This observation would need to be done with sensors that can measure changes within the physiological states of arousal and at the same time be unobtrusive, low cost, and comfortable enough for continuous wear [32].
These wearable interventions may result in improved independence through remote support and the acquisition of anticipatory responses as well as improved independence as perceived by professionals and peers [23]. Using proximate visual and auditory feedback has the potential to support continued development, including generalization to other contexts [27]. HR measurement as a measure of stress in children with ASD could also provide insight for stress prevention and tailored treatment [19].
Wearable sensors provide an unprecedented opportunity to capture a child’s full movement repertoire in a more naturalistic environmental setting. Quantitative measures can aid in the ability to evaluate subtle motor differences in early infancy. Furthermore, it allows for the measurement of motor activity that plays an intrinsic role in the development of motor skills. It has also been proposed that ASD is a disorder of synaptic plasticity that results in imbalances of excitation and inhibition in the developing brain so, motion complexity has the potential to track early infant motor development and to discriminate high-risk infants that go on to develop ASD [25]. Successful monitoring of repetitive behaviors can significantly contribute to critical life-quality-improvement tasks, such as evaluation of responsiveness to therapies and prediction of disruption autism actions [15].
Discussion
A range of WTs for autistic youth, measuring and targeting a variety of functions was identified in this review. The need for careful and methodological evaluation of such emerging technologies becomes important to assist not only the therapists and clinicians in their selection of suitable tools for assessment and intervention but to also guide the parents and caregivers for interventions at home [6]. Technology-based assistive tools are increasingly important tools to address the educational and therapeutic needs of students with ASD. Similarly, these technologies can empower educators and Professionals to improve the intervention regime and to decrease stress and burnout. However, it is important to critically study the feasibility and efficacy of these technology-based interventions [20]. Detection of emotional states based on one’s physiology has been an active topic of research in the biomedical space. Awareness of anxiety symptoms, such as arousal, is a significant clinical concern in ASD. Wearable tools that can provide a real-time and objective measure of these symptoms have the potential to improve the management of these symptoms [14].
Nonetheless, including technology in the daily life of a person with ASD, as for individuals with cognitive impairment, is a sensitive issue. Long-term acceptance of assistive devices is unlikely if they result in stigmatization, cumbersome management, or low customization possibilities [12]. The advantages of biologically based tools to identify processes that underlie behavioral dysregulation as it unfolds during moments of escalation are numerous and have great translational potential, especially for those unable to provide reliable self-reports on their arousal states [17].
About half of the surveyed individuals prefer to use wearable technology which can monitor body signals such as heartbeat and respiration and those are related to difficulties with monitoring or being aware of their emotional state. More interestingly, they asked for devices that give them alerts when signs of negative emotions are detected (e.g., the user is stressed) [33].
According to the survey of Koo et al. [2], parents or caregivers of individuals with ASD report that they prefer functions related to wearable technology that aid awareness and management. For instance, parents would like to be able to monitor the vital body signals of care receivers to understand their emotions and anxiety level so they can help them to relieve stress. Specifically, they reported that one of the most common challenges for individuals with ASD is regulating their own emotions and managing their anxiety, and having control over sources of stress. Based on those findings, the type of wearable technology and device form factor should be carefully selected.
Conclusion
Wearable physiological and emotion monitoring devices are becoming popular and can perform multiple functions. In addition to the usefulness of those devices for the general population, they have the potential to help people with ASD, their parents, and caregivers. Advancements in technology that include behavioral and physiological response monitoring with wearable sensors provide the opportunity to acquire a new understanding of the internal components of observable behavior of children with ASD. Professionals working with the autistic population may be able to gain insight into the internal states of clients who cannot share this information verbally through technology. Clinicians may be able to quantify differences in response to the sensation that is currently captured with observational or subjective report measures. This could lead to better individualization of treatment and greater treatment effectiveness.
Author contributions
All the authors agreed to be accountable for all aspects of the work in ensuring integrity of review article.
CONCEPTION: All authors.
WRITING: Deepti Ahuja.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Dr. Aparna Sarkar, Dr. Sushil Chandra and Dr. Prakash.
Ethical considerations
This study, as a literature review, is exempt from Institutional Review Board approval.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare no conflict of interest.