
Abstract
BACKGROUND:
Flow recirculation occurs in eccentric coronary stenosis, which can lead to adverse outcome. The complex local geodesic patterns of eccentric stenosis are critical factors in determining the flow characteristics in post-stenotic flow.
OBJECTIVE:
The main objective of this study is to relate the relationship between the detailed morphological parameters in eccentric coronary stenosis and the post-stenotic flow characteristics.
METHODS:
Several idealized eccentric coronary stenosis models with variable morphological parameters are created to conduct a series of computational fluid dynamics analysis. The impact of four specific lesion morphological parameters, eccentricity index (EI), diameter stenosis (DS), stenosis length (SL) and shape of lesion, are investigated.
RESULTS:
When EI is small (
CONCLUSIONS:
Except DS, the detailed geometry patterns (EI, SL and shape of the stenosis) also have great impact on post-stenotic flow behaviors in eccentric coronary stenosis.
Keywords
Introduction
Atherosclerotic plaques in coronary arteries have great impact on blood flow patterns and will result in local physiological perturbances such as recirculation, which can lead to detrimental biological and clinical sequelae [1, 2, 3]. Recirculation zones will cause stasis and provide an optimal environment for procoagulant factor mixing and promoting activation of the coagulation system [4, 5]. High shear rate are also observed in severe coronary stenosis, which can result in abnormal platelet and leukocyte activation [6, 7].
Eccentric coronary stenosis models and boundary conditions. (A) Idealized models and morphological parameters: EI, DS and SL. (B) Four shape of the eccentric coronary stenosis models (for trapezoid-shaped models, the wall length of the upper base is set to be 1/3 of the stenosis length). (C) Normalized boundary velocity waveform used at the inlet.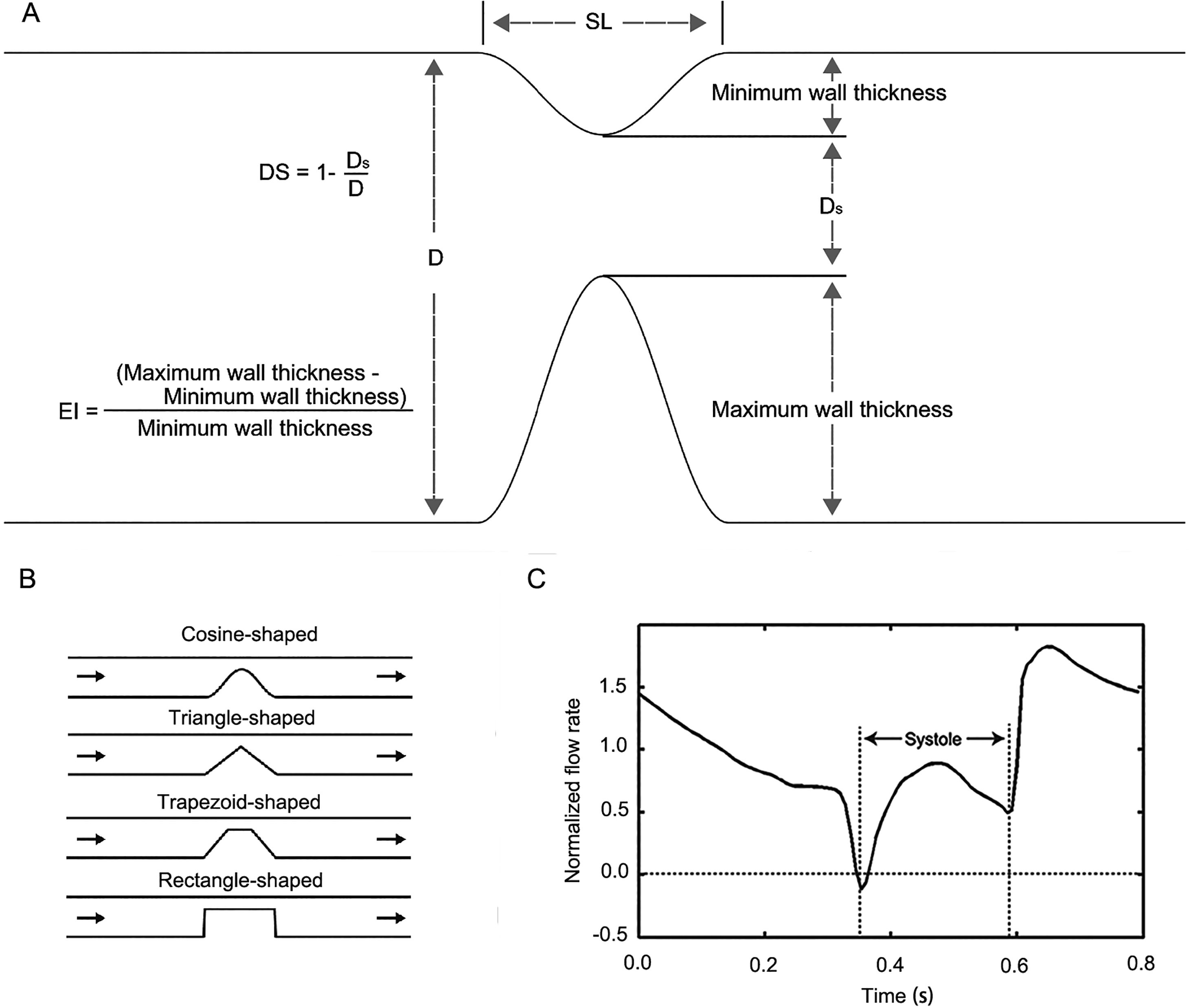
A lot of researchers have carried out their work on flow behaviors in different-shaped stenosis [8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]. Among these studies, concentric (about the center of the artery) shaped stenosis has been widely studied. However, eccentric lesions are most commonly observed in coronary stenosis [19]. Flow patterns in concentric shaped stenosis are quite different from those in eccentric ones [20, 21]. It is also reported that eccentric lesions are more likely to be observed in patients with cardiovascular symptoms [22, 23]. Mates et al. have studied the impact of eccentric lesions on flow pressure drops [24]. Yong and Tsai have demonstrated that eccentric show strong influence on flow characteristics [20, 21]. Recently, by using the computational fluid dynamics (CFD) method, Javadzadegan et al. demonstrated that the lesion eccentricity could affect the flow recirculation and shear rate to a great extent [25]. However, the unsteady flow condition was not included in their computational model, which makes the flow behavior in stenosis section more complex. To overcome this limitation, a transient particle image velocimetry experiment was performed to relate the correlation between Reynolds number and eccentricity effect [26].
From the brief review of literature, the impact of detailed morphological parameters of eccentric coronary stenosis on post-stenotic flow characteristics has not been investigated. Therefore, the main objective of this study is to relate the relationship between the detailed morphological parameters in eccentric coronary stenosis and the flow characteristics. Since pressure drop is relatively independent of stenosis geometry (primarily dependent upon the minimum area of the stenosis) [24], here we will concentrate on blood flow patterns in recirculation zones. Several idealized coronary stenosis models with variable morphological parameters are created to conduct a series of morphological parametric studies. The impact of four specific lesion morphological parameters, eccentricity index (EI), diameter stenosis (DS), stenosis length (SL) and shape of lesion, are investigated by using the CFD approach.
Streamlines for models with different EIs at 
Eccentric coronary stenosis models
The idealized eccentric coronary stenosis sections are modeled as 3D pipes. The diameter of the arteries is set as 3 mm. The four morphological parameters are illustrated in Fig. 1A and B. EI is defined as [27]:
0 represents no eccentricity and 1 represents highest eccentricity. DS is calculated as:
where
Pulsatile flow waveform was applied as velocity inlet boundary condition. The inflow profiles were based on the work of Boutsianis et al. [28]. The cardiac period and mass flow rate were normalized to 0.8 s and 0.9 g/s, respectively. The normalized flow rate was shown in Fig. 1C. The Womersley velocity profiles based on the specific inflow profiles wave were prescribed at the inlet. A zero relative pressure condition was applied at the distal end [29]. Furthermore, a no-slip wall boundary condition was imposed on the arterial wall.
Computational method
CFD analysis was performed using the commercial CFD software ANSYS FLUENT V13 (ANSYS Inc.). The numerical scheme in ANSYS FLUENT V13 was based on the finite-volume method. Blood was modeled as an incompressible Newtonian fluid. Dynamic viscosity was set to 3.5 cP and density
Axial velocity profiles for models with different EIs at 1, 2, and 3 diameters downstream of the stenosis section (indicated by plane 1, plane 2 and plane 3). The profiles at three different phases of the cardiac cycle (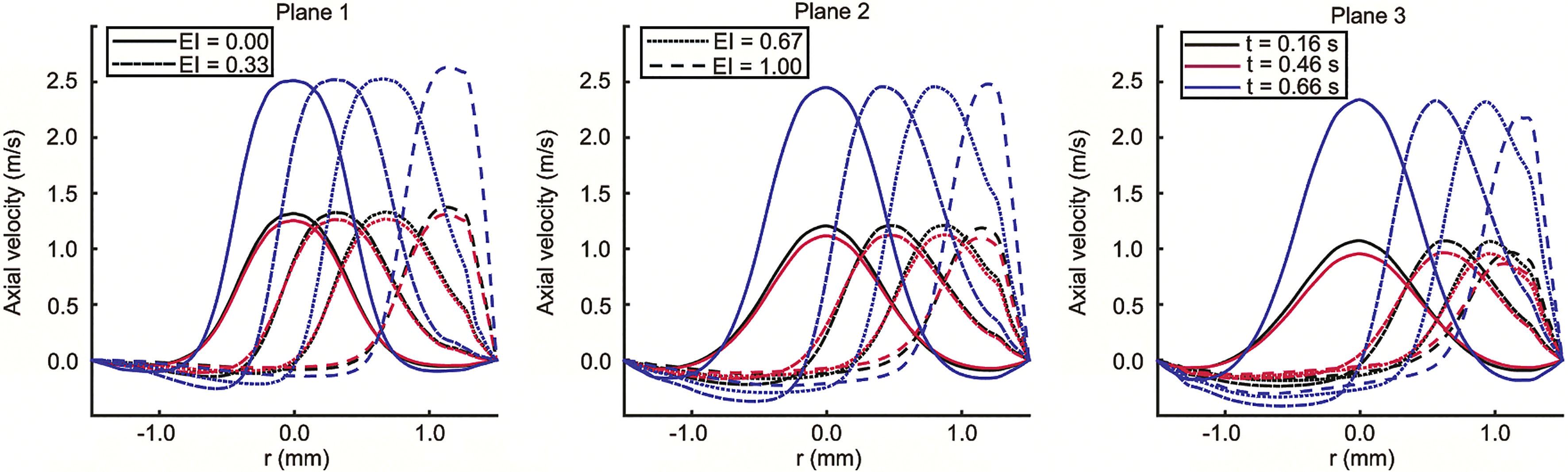
Streamlines for models with different DSs at 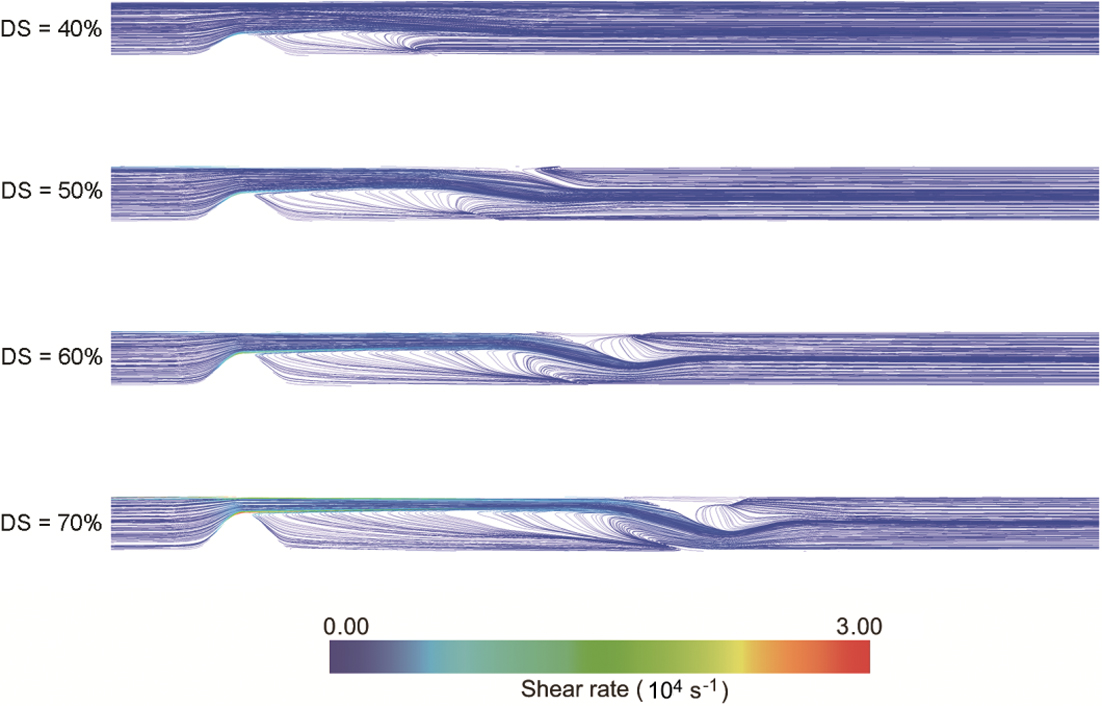
Models with different EIs
Blood flow in four models with different EIs are simulated and the streamlines at early diastole (0.66 s) for four different EIs are shown in Fig. 2. Shear rates are also labeled at the streamlines. The DS, SL and shape of the stenosis are kept constant for the four models (DS
Models with different DSs
To demonstrate the effect of DS in eccentric stenosis, the streamlines of four models with different DSs at early diastole (0.66 s) are shown in Fig. 4. The EI, SL and shape of the stenosis are kept constant for the simulated models (EI
Axial velocity profiles for models with different DSs at 1, 2, and 3 diameters downstream of the stenosis section (indicated by Plane 1, Plane 2 and Plane 3). The profiles at three different phases of the cardiac cycle (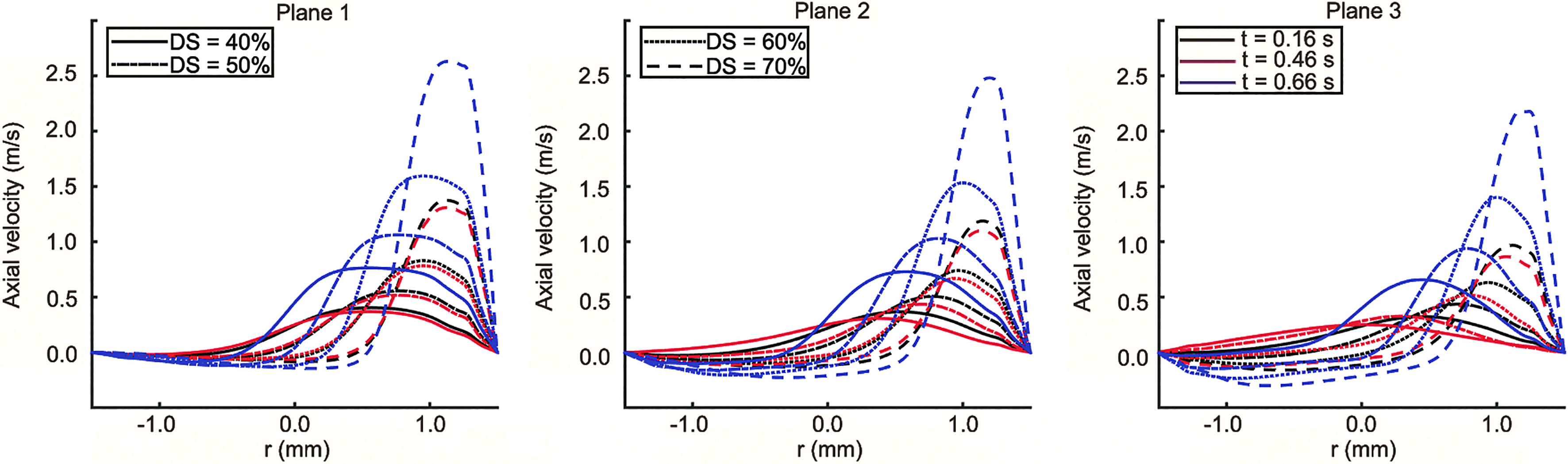
Streamlines for models with different SLs at 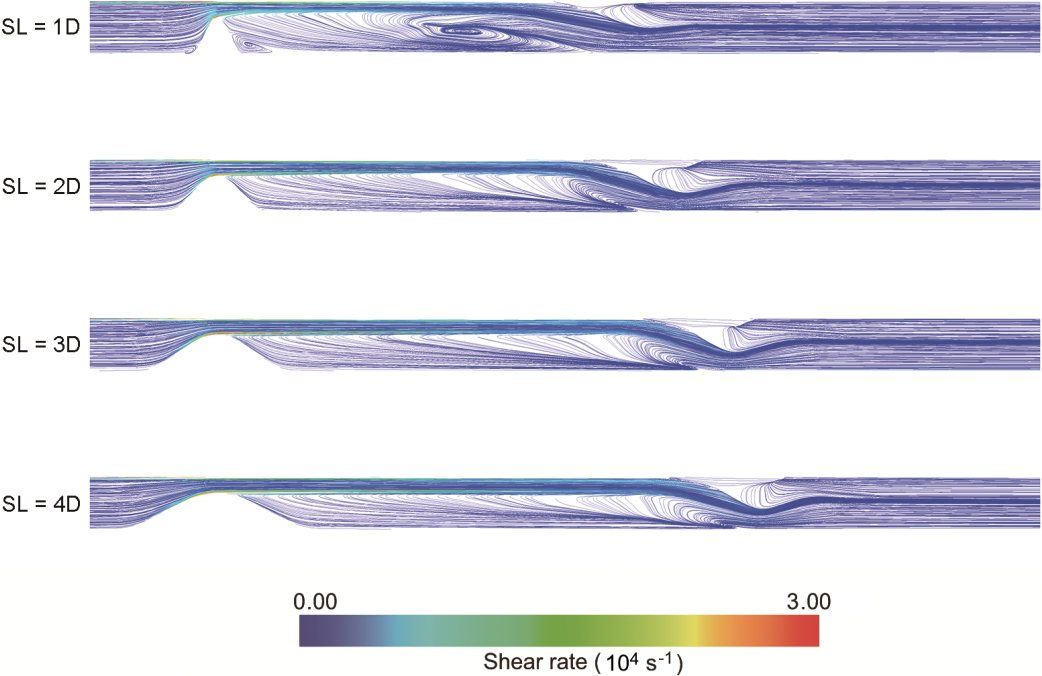
To demonstrate the impact of SL in eccentric stenosis, the streamlines at early diastole (0.66 s) for models with different SLs are shown in Fig. 6. The EI, DS and shape of the stenosis are kept constant for the four models (EI
Models with different shapes
Streamlines for models with different stenosis shapes at early diastole (0.66 s) are shown in Fig. 8. The EI, DS and SL are kept constant for the four models (EI
Axial velocity profiles for models with different SLs at 1, 2, and 3 diameters downstream of the stenosis section (indicated by Plane 1, Plane 2 and Plane 3). The profiles at three different phases of the cardiac cycle (
In this study, a CFD simulation was conducted to relate the impact of specific geodesic patterns of eccentric stenosis on the flow characteristics of the recirculation zones in coronary arteries. From the results, the geometry patterns have great impact on the velocity profiles at the stenosis section, and these changes in velocity profiles would further lead to changes in post stenotic flow behaviors.
As demonstrated, larger DS was associated with larger regions of recirculation in eccentric stenosis. Low shear rates was observed in the recirculation zone, providing a favorable environment for stasis-related thrombosis. As DS increase, high shear rates occurred at the throat section, which might lead to abnormal platelet activation. However, an important finding in our evaluation was that except DS, the detailed geometry patterns (EI, SL and shape of the stenosis) also had great impact on post-stenotic flow behaviors.
Streamlines for models with different shapes at 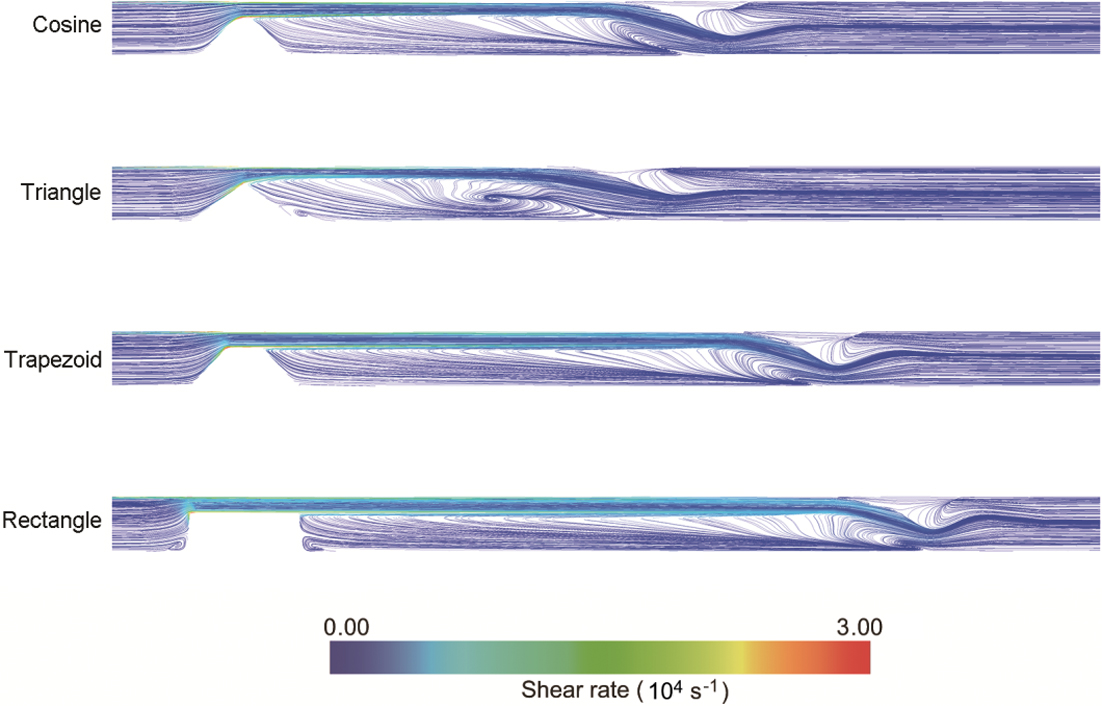
Axial velocity profiles for models with different shapes at 1, 2, and 3 diameters downstream of the stenosis section (indicated by Plane 1, Plane 2 and Plane 3). The profiles at three different phases of the cardiac cycle (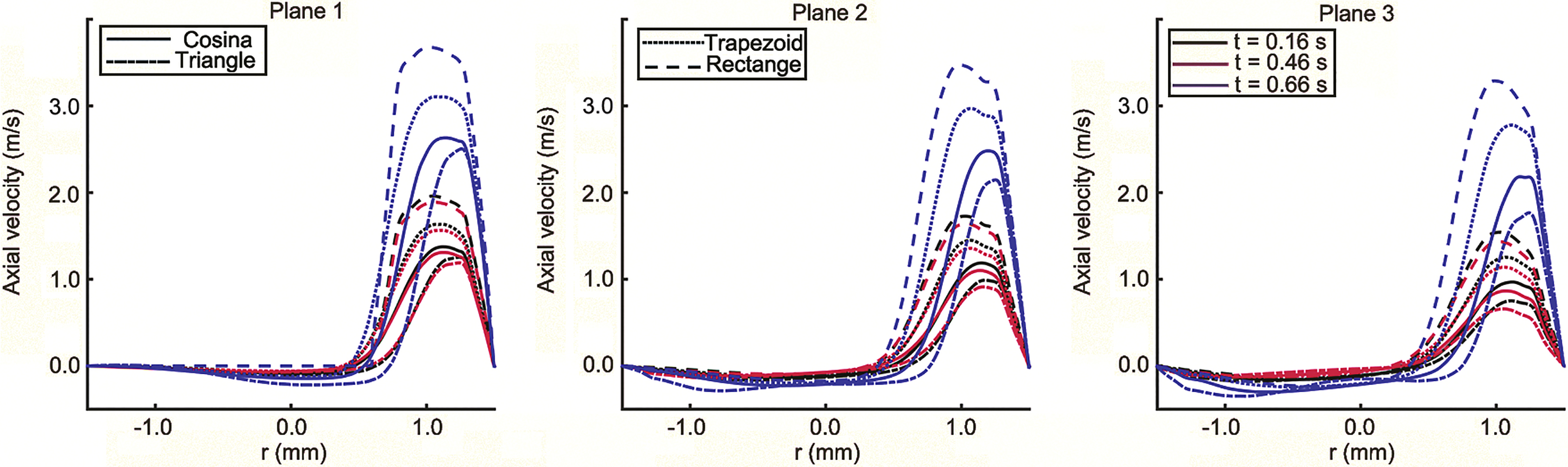
EI is the most popular index to quantify eccentric stenosis. Previous study reported that eccentricity had minor impact on the shear rate at the throat wall, while as eccentricity increase, a significant decrease in shear rate at the opposite wall was observed [30]. Here, similar results were obtained in this work. Javadzadegan et al. reported a positive correlation between EI and recirculation zone length, and a PIV experiment was implemented to further validate their conclusion (positive correlation between EI and recirculation zone length) in transient condition [25, 26]. However, the other lesion morphological parameters (except EI), which played an important role in determining the recirculation zone length, were not kept the same among models with different EIs. From our results, the relationship between EI and post-stenotic flow behaviors are complex. When EI is small (
Increase of SL would lead to increase of recirculation zone length in eccentric stenosis. Similar phenomena were reported in bell-shaped concentric stenosis [31]. It is very interesting to note that flow patterns in recirculation zone became more complex when SL decreased to 1 diameter. This might be caused by a sharper inlet shape in model with a 1 diameter SL. The impact of sharpness of inlet shape on flow patterns could also be demonstrated by comparing different shapes of stenosis. Rectangle stenosis had a sharpest shape, leading to a largest recirculation zone length. While, triangle stenosis had a modest shape and led to a smallest recirculation zone length.
We have to clarify that there are still some limitations. In this work, blood is modeled as Newtonian fluid and vessel wall is modeled as rigid wall. However, previous studies showed that these assumptions had minor impact on flow distributions in stenosis coronary arteries. Our work focused on the morphological parameters that fully characterize the geodesic patterns of eccentric coronary stenosis. Thus, idealized models were preferred to minimize the effect of patient-specific geometric variability. However, curvature and bifurcations, which often co-exist with eccentric stenosis, were ignored by using this approach. Nevertheless, the general concepts addressed from this work would still be applicable to the realistic eccentric coronary stenosis.
Footnotes
Acknowledgments
This work was supported in part by the National Science Fund of China under Grant 61601368, 61273250, the Natural Science Basic Research Plan in Shaanxi Province of China (2017JQ6012) and the Fundamental Research Funds for the Central Universities (No. 3102017jc11002).
Conflict of interest
None to report.