
Abstract
BACKGROUND:
Kyphoplasty is a proven minimally invasive procedure for the treatment of patients with osteoporotic fractures. By augmentation of fractured vertebral body, however, a very large portion of the intervertebral structures will be destroyed. With the help of a new device (Vertect Jack Device), the erection of the vertebral body will be carried out more gentle.
OBJECTIVE:
In the present study, the new method should be clinically tested for efficacy and safety for the first time. As a comparison results of previous treatments with kyphoplasty were used.
METHODS:
For Vertect Jack Device study patients with painful vertebral fractures were selected in which conservative treatment had not yielded sufficient results. For comparison random data from the records of patients who had been treated with kyphoplasty were selected. The Vertect Jack Device was placed under the central fractures and then erected. After having restorted the vertebral height the device was removed and cement injected. Clinical and radiological examinations were carried out before and after 1,3, and 6 months.
RESULTS:
In the Vertect Jack Device Group the data of 40 patients were evaluated. For group 2 (kyphoplasty) 50 patients were selected. There was a significant difference in the duration of the surgery (Group 1: 27.4, Group 2: 45.9 minutes). A significant difference of 20 mm with regard to the reduction of VAS scores (0–100 mm pain intensity) was detected. Under the application of the Vertect Jack Device an average increase of 3.1 mm of vertebral height was achieved. In group 2, the erection averaged 0.4 mm. A correlation between the postoperative change of vertebral body height and VAS scores could not be detected in both groups.
CONCLUSIONS:
The comparative analysis of this study shows that promising results can be achieved with the augmentation of vertebral fractures with the Vertect Jack Device. When compared with kyphoplasty, advantages show in terms of targeted and thus more gentle application possibility and better pain relief over a period of 6 months after surgery. Further study results should help to demonstrate the efficacy and tolerability of the new method.
Introduction
In order to treat patients with painful osteoporotic compression fractures vertebroplasty and kyphoplasty have proven as minimally invasive procedures [1]. Both techniques can be used successfully when a conservative treatment did not lead to sufficient improvement in pain and functional limitations [2, 3]. The results of several clinical studies have demonstrated that a curative effect can be achieved through the stabilization of the vertebral body, and the restoration of vertebral height in a very high percentage of the operated patients [4, 5]. As a result of these effects the limitations of quality of life will be reduced [6, 7].
When balloon kyphoplasty (BKP) was compared with non-interventional conservative measures [8] the Physical Component Summary Score (PCS) improved in the kyphoplasty-group by 7.2 points after one month while in the group with conservative treatment an improvement of only two point was achieved. When comparing the improvement of quality of life, the kyphoplasty showed also a significant superiority in the controls after one month and after one year.
Similar results were observed in another study [9] in which the successes of radiofrequency-kyphoplasty (RFK) were compared with those of conservative treatment. The RFK (
Nevertheless, there are results of some studies showing that the endplate fracture recovery after balloon-kyphoplasty is temporary, and there is not seldom a new body collapse as soon as the balloon is deflated [11, 12].
In contrast, a new method using the Vertect Jack Device (Fig. 1) offers the possibility to restore the fractured vertebra sustainably. This method, however, differs from a similar device for enhanced restoration of vertebral height in which the devices in form of expandable implants are inserted for permanent remain. The devices are than fixed with PMMA. This procedure aims to provide anatomical restoration and stabilization of the fractured vertebra as well as endplate restoration. The clinical results of studies with this device showed a significant superiority of the new technique concerning height restoration and height maintenance [13]. The results gave also evidence for a significant reduction in pain and in analgesic intake as well as for a marked improvement in ODI scores, which could not be reached by a conservative treatment [8, 11].
These results were the reason to develop a procedure, with which the fractured vertebral body can be erected with the same mechanism [14], but without leaving implants in the vertebral body. The aim was to use and to test a more cost-effective method that would prove to be the same efficiency and safety.
The Vertect Jack Device is mechanically spread in the vertebral body, so that the height is restored. After restoration polymethylacrylate bone cement is injected to stabilize the vertebral body.
Using the data of a first study, it should be examined to what extent the Vertect Jack Device without implants is also being suitable to erect fractured vertebrae and to sustain stability in order to achieve a significant decrease in back pain and a significant improvement in functionality. For comparison random data were selected from patients whose vertebral fractures were treated by kyphoplasty.
Methods
For the present study we selected patients with painful vertebral fractures (VAS
The Vertect Jack Device; closed and opened.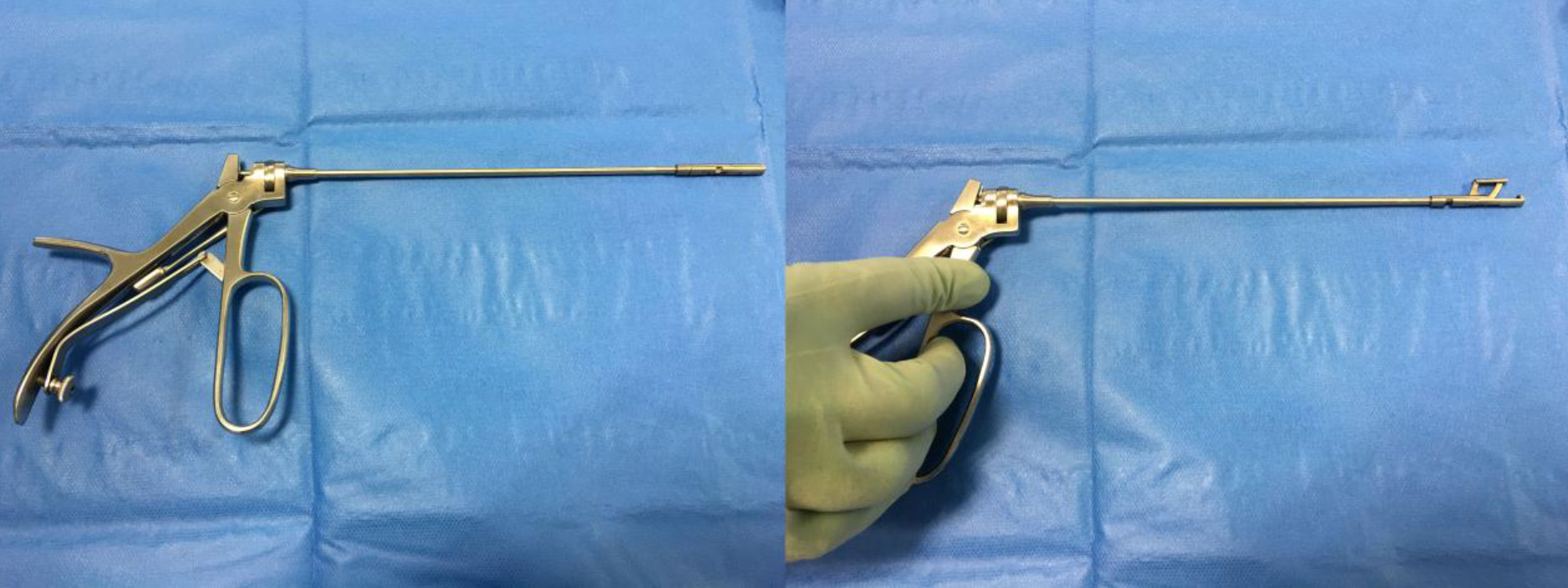
Patients confirmed in writing the willingness to participate in the study to assess efficacy and safety of the vertebral surgery with the Vertect Jack Device.
Participants were recruited for the study with the Vertect Jack Device in order of hospitalization. For the comparative evaluation data were randomly selected from a pool of patient records, containing the findings and results of patients in whom the vertebral fractures were treated by Balloon Kyphoplasty (BKP).
The patient is poisoned in prone position. The minimally invasive surgical procedure is performed in general or regional anesthesia. A trocar is used under fluoroscopic control to determine the path to the vertebral body. Fluoroscopic control is used at every step of vertebral body access. While moving forward in the pedicle tunnel and reaching the posterior wall of the vertebral body, the tip of the trocar is inside the pedicular ring. The trocar is inserted through the pedicle to the posterior part of the vertebral body. The Vertect Jack Device is placed central under the fracture (cranial or caudal endplate) and is erected by manual force. When the vertebral height is restored by or a cavity is performed (in elderly fracture) the Vertect Jack Device is removed and cement is injected through cement fillers. After cement augmentation the working channel is removed (Fig. 2). Before the study, after surgery and after 1, 3 and 6 months clinical and radiological follow-up examinations were performed. Clinical success was determined by the decrease in pain intensity (Visual Analogue Scale; VAS 0–100 mm) and by reduction of functional limitations (Oswestry scores, ODI %) Moreover, the height of the vertebral body was measured comparatively in postoperative plain radiographs (Fig. 3).
a–b) Preoperative MRI scans; c–n) Vertect Jack Device procedure including preparation, vertebral body erection and cement augmentation.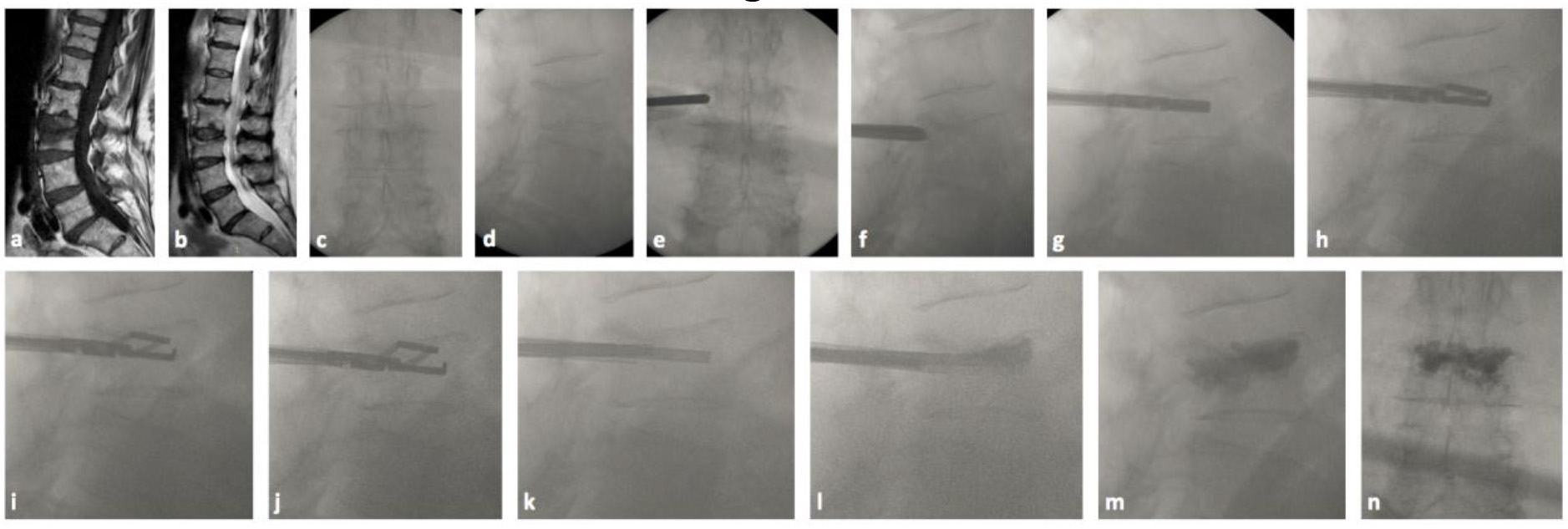
Postoperative plain radiographs a.p. and lateral.
The BIAS program (H. Ackermann, Univ. Frankfurt/M) was used for all statistical analyses. Following test methods were applied:
Calculation of the estimated values of mean and SD, medians plus quartiles Calculations of the confidence intervals for the mean One-sample t test for the comparison of parametric values before–postoperative Wilcoxon matched pairs test for the comparison of nonparametric values before and after surgery Welch test for group comparisons of parametric values with heterogeneous variances Wilcoxon Mann–Whitney U test for the group comparison of nonparametric values Calculation of the simple linear Pearson’s correlation with graphical representation or Spearman’s and Kendall’s rank correlation
For the graphical representations, box plots with the medians and the individual quartiles were calculated. An upper threshold of 95% was specified for the probability of differences (
In group 1 (Vertect Jack Device), the data of 40 patients (w: 23 m: 17) were evaluated. The average age of patients was 70.6
Localization and numbers of treated vertebrae
Localization and numbers of treated vertebrae
The average operating time was in group 1: 27.4
Visual analogue scale (VAS: 0–100 mm) before and after surgery
The average baseline of pain intensity in Group 1 was 82 mm on the VAS 0–100 mm. One month after the surgery a decrease by an average of more than 75% could be achieved; after 6 months the pain reduction showed an overall decrease of 85%, and there was none of the patients with an increase in painful symptoms in comparison to the baseline (Table 2). The VAS scores in Group 2 were prior to study entry only slightly less than in group 1; the decline was 66%, and no deterioration as compared to baseline could be shown. The statistical analysis of VAS scores showed a significant decline with a high effect size (Table 3, Fig. 4). The difference in the VAS reduction was 20.5 mm in favor of Vertect Jack Device procedure, which corresponds to an effect size of
Differences (
Oswestry Disability Index (ODI) before and after surgery
VAS differences before and after surgery.
The Oswestry values (%) showed a significant decline for all patients registered (Table 4). There were improvements by about two-thirds percentage points compared to the values before the surgery in both groups (Table 5). The difference of the decrease in the Oswestry-values (Table 5) between the two groups was 6 percentage points, which means an average effect size (0:28;
Differences (
Figure 5 shows the mean changes of vertebral height after the surgery. In the first vertebrae of group 1, an increase could be achieved in 35 (88%) cases; in 5 patients the vertebral heights remained the same after the surgery.
Changes in vertebral height.
The mean value of the increase was after one month 3.1
Correlation VAS vs. ODI – changes after surgery in group 1.
The present study results allow a first evaluation of the new method for minimally invasive treatment of patients with vertebral fractures. It turns out that with the Vertect Jack Device an impressive erection of the fractured vertebral body can be achieved. The study showed that height restoration was significantly better in the Group 1 compared with the kyphoplasty group. The clinical implications include a better restoration of the sagittal balance of the spine and a reduction of the kyphotic deformity, which may relate to clinical outcome.
It proves to be an advantage that the small instrument can be very specifically targeted in the vertebral body. In vertebral fractures it is possible to reduce the amount of cement when the Vertect Jack Device is used without compromising the reposition height after reduction, in contrast to kyphoplasty that needs some more cement volume. In this way, less structure is destroyed in the vertebrae than by using the balloon kyphoplasty [14]. Furthermore surgical time was significantly lower in group 1 because no complicated manual positioning maneuvers were needed to restore wertebral height prior to kyphoplasty. This procedure leads to a good stability. However, the data of this study does not yet allow sufficient conclusions about the risks for subsequent fractures in adjacent vertebrae.
The erection of the fractured vertebral body is associated with significant reductions in pain intensity and functional limitations. Based on the data from this study, however, it cannot determined whether these improvements of clinical findings correlate with the extent of the erection of the vertebral bodies.
In order to assess the results of this new procedure, selected data were used at random, who belonged to previous series of studies in which the patients treatment with kyphoplasty had undergone. This is therefore not a comparison test in the sense of a pre-planned controlled trial, but a pilot study whose results will make it possible to carry out further clinical trials, in which hypotheses will be prospectively set and verified. With this in mind, it seems important that the results of this study have indicated a clinical superiority of the new method.
Conclusion
The comparative analysis of this study shows that promising results can be achieved with the augmentation of vertebral fractures with the Vertect Jack Device. When compared with kyphoplasty, advantages show in terms of targeted and thus more gentle application possibility and better pain relief over a period of 6 months after surgery. Further study results should help to demonstrate the efficacy and tolerability of the new method.
Conflict of interest
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.