
Abstract
BACKGROUND:
Fractured vertebral bodies are a common and wide spread health issue.
OBJECTIVE:
The purpose of this study was to develop a standardized method to experimentally generate compression fractures in vertebral bodies. The influence of the pedicles has been investigated with regards to the fracture behavior. The correlation between bone mineral density (BMD), the cause of fractures and the fracture behavior was investigated.
METHODS:
Twenty-one fresh frozen human lumbar spines were examined for bone mineral density (BMD) by means of quantitative computed tomography (qCT). All soft tissue was removed, vertebrae were carefully separated from each other and the exposed cranial and caudal endplates were covered with a thin layer of resin to generate a plane and homogeneous surface. A total of 80 vertebral bodies were tested until fracture.
RESULTS:
A good positive correlation was found between BMD, fracture compression force and stiffness of the vertebral body. No significant differences were found between the fractures generated in vertebral bodies with and without pedicles, respectively.
CONCLUSIONS:
Our model represents a consolidation of already existing testing devices. The comparative measurement of the BMD and the fracture behavior shows validity. In contrast to other authors, the force was applied to the whole vertebral body. Furthermore the upper and lower plates were not parallelized and therefore the natural anatomic shape was imitated. Fracture behavior was not altered by removing the pedicles.
Introduction
Osteoporosis is a health issue of social and economic importance, which leads to poor life quality and to physical disability. Osteoporosis is the most frequent bone disease of elderly people and makes the bone vulnerable to fractures. Bone, especially of the axial skeleton, has to sustain various challenges. It has to provide both enough stability and elasticity in order to resist the compression and tension forces of daily life [1, 2]. Due to an aging population, the prevalence of osteoporosis-related diseases increases. There are approximately 1.4 million persons with vertebral compression fractures worldwide [3]. In the United States, there are about 750.000 persons with vertebral compression fractures; only one third receives treatment [4]. Osteoporotic compression fractures can result in progressive kyphosis and chronic pain with a consecutive loss of mobility. Besides the severe pain, the potential consequential damages are the destruction of the vertebral bodies and a progressive loss of the physiological alignment of the spine. To understand the fracture behavior of vertebral bodies in the context of bone mineral density and osteoporosis, finding and testing methods for adequate treatment, biomechanical test methods are mandatory.
Older biomechanical testing procedures in this area had been developed to investigate the effects of vertebral augmentation procedures such as vertebroplasty and kyphoplasty. Since these therapies were established, many studies related to the generation of osteoporotic compression fractures of the vertebral body have been published [5, 6, 7, 8, 9, 10, 11, 12]. The testing methods and the preparation of the vertebral bodies in these studies differ greatly and the induced fractures cannot be compared directly.
The aim of this study was the development of an in vitro model to generate compression fractures in vertebrae of the lumbar spine and the thoracolumbar spine in a standardized way. The specially designed testing jig incorporates the advantages of the existing models. To validate our in vitro model, first of all the correlation between bone mineral density and the fracture behavior was investigated. Additionally the influence of the pedicle-structures was tested.
Materials and methods
Preparation of the vertebral Bodies
For this investigation a total of 80 vertebral bodies from 21 body donors were tested. The study was approved by the Institutional Ethics Review Boards. Lumbar spines were explanted from the body donors (Table 1) in the Institute of Legal Medicine and were shipped frozen (
At first, the average bone mineral density (mg CaHA/ml – equivalent) was determined for each vertebra divided in trabecular and cortical bone by means of quantitive computed tomograph (qCT, SOMATOM Sensation 64, Siemens, Germany). First, the spines were brought to room temperature in physiological saline solution 24 hours before testing. In order to obtain the isolated vertebrae, all soft tissue, intervertebral discs, were removed. Afterwards the lumbar spines were divided into two test scenarios:
In the first scenario, the influence of resecting the pedicles including spinous processes and transverse processes were examined with 20 vertebral bodies (10 with pedicle; 10 without pedicle). To reduce the variability between the subjects, five spines were matched by bone density and vertebrae height, each of the spines has four vertebral bodies. The resection of the pedicles was done in rotation so that each spine has two vertebral bodies with and without pedicle.
In the second scenario the remaining vertebral bodies were freed from pedicle, spinous processes and transverse processes (Fig. 1). Additionally ten specimens without pedicles and processi of the first scenario were merged to that investigation (overall
Gender, means and range of age, height and weight of the 21 body donors
Gender, means and range of age, height and weight of the 21 body donors
Final prepared vertebral body without pedicles; an individual thin layer of resin level the unevenness between the specimen and the testing jig A) view from posterior; B) lateral view; scale bar in mm.
During the preparation, the specimens were kept hydrated and wrapped in saline-soaked tissue. The next step was the geometrical homogenization of the contact area. A negative of the superior and inferior end plate depression was molded for each specimen with a quick setting resin (RenCast FC 53, RenShape Solutions, USA). Finally the anterior height of the vertebral body was measured by caliber followed by submersion in 37
The construction and fabrication of the measurement setup is oriented towards existing test devices. Development and construction of the mechanical components was performed using the software CATIA (V5, Dassault Systemes, France). The entire construction (Fig. 2) was designed according to the geometries of the universal testing machine (Model Z010, Zwick GmbH, Germany). The lower end of the machine traverse was used to fix the upper part of the jig (Fig. 2; Point 1). A six-degree-of-freedom load measurement cell (Fig. 2; Point 2) was used to register the force and moments in each direction. The origin of the coordinate system was positioned in the center of the load cell. The maximum capacity of the load cell is 15 kN in z-direction (compression) and 5 kN in X (medio-lateral shear force) and Y-direction (anterior-posterior shear force) while the maximum measurable moment was 200 Nm in each axis. The data of the sensor was acquired with a 16 bit A/D-converter (NI PCI 6220; National Instruments; USA) in a rate of 100 samples per second and recorded with a custom made LabVIEW code (Version 2010; National Instruments, USA) triggered with the compression test. A ball joint (Fig. 2; Point 3) ensured a geometrical equilibration of the plate and the vertebral body (Fig. 2; Point 4) during the test. The adjustable table (Fig. 2; Point 5) allows for an alignment of the vertebral body in relation to the compression force.
The vertebral body was placed on the lower base plate. The position was aligned in such a way that the vector of the compression force in the sagittal plane passed 10 mm behind the anterior edge of the cortex. An upper load platen, having coarse sandpaper attached to its base, prevented any dislocation of the vertebral body. All specimens were subjected to axial compression in a displacement-controlled mode at a rate of 5 mm/min with an initial force of 100 N. Load-displacement curves were automatically recorded. The test was interrupted if either of the following criteria was met: 1) the anterior height of the vertebral bodies was decreased by 50%; 2) a compressive load of 8 kN was exceeded.
Statistics
Fracture forces and fracture displacement were defined as the first maximum in the load-displacement-plot. Stiffness was measured between 25%–75% of the fracture load. If the limits were passed without fracture generation, the stiffness was measured between 25%–75% of the maximum measured force. All results are presented with the mean value and standard deviation (SD). The Mann-Whitney test was used to compare two groups of each scenario. To show a correlation between BMD and fracture load, Spearman correlation was computed. Statistics were calculated in Prism Version 5 (GraphPad Software, La Jolla, USA) while
Mean and standard deviations in brackets of the measured parameters with and without pedicles
Mean and standard deviations in brackets of the measured parameters with and without pedicles
Set-up for axial compression testing for a single vertebral body; 1) upper fixation to the testing machine (traverse); 2) six-degrees-of-freedom load measurement cell; the origin of the coordinate system is in the center of the load cell; x-axis is the transversal axis; y-axis is the sagittal axis; z-axis is the longitudinal axis 3) ball joint in line with the z-axis; 4) vertebral body; 5) X-Y-table fixed on the bottom of the testing machine.
Influence of the pedicles
The bone mineral density and the height of the vertebral bodies were comparable in both groups (Table 2). In one specimen of the group without pedicles, a faulty attachment led to an uncontrolled translatory migration of the vertebral body within the jig during the test, which rendered the measured data unreliable. This specimen was therefore excluded from the statistical analysis. Seventeen vertebral bodies showed failure at the anterior edge, one (without pedicles) at the posterior edge. The specimen (without pedicles) with the highest cortical BMD of 374.3 mg Ca-HA/ml reached the limit of 8 kN (trabecular BMD of 163.8 mg Ca-HA/ml) without any fracture of the vertebral body. No significant different loading behavior was found until fracture was measureable between the two groups (3).
Exemplary load-displacement curves in each direction of 3 vertebral bodies of each with and without pedicles. The same color defines vertebral body of the same spine while the cross shows the fracture detection.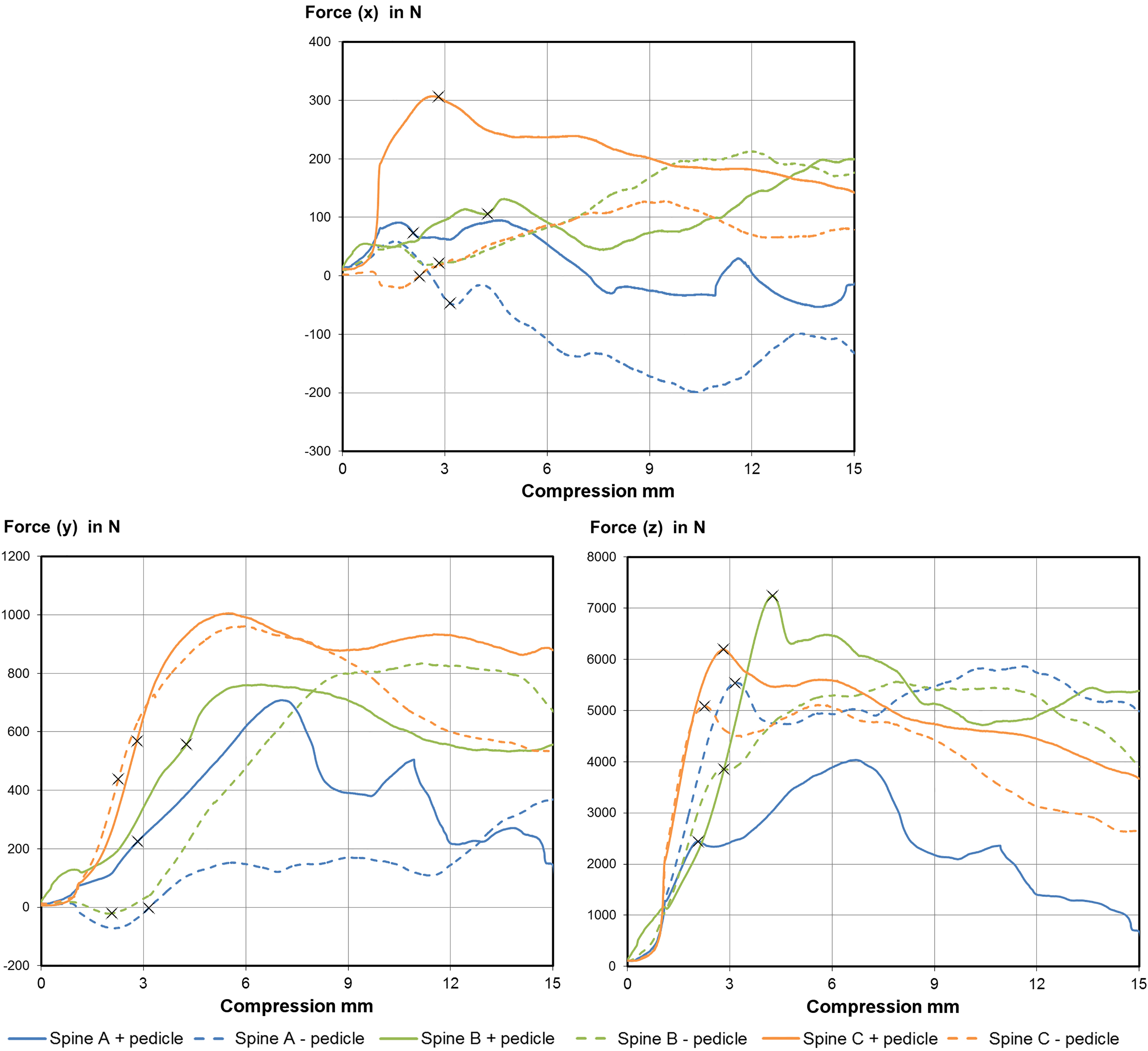
Two specimens were excluded from the statistical analysis due to slippage of the vertebral body in the jig while testing.
The force limit was reached with two other specimens in the high BMD group (cortical BMD of 374.3 mg Ca-HA/ml and 460.1 mg Ca-HA/ml). 63 of 66 specimens showed a failure on the anterior cortex while the remaining three specimens (all with a BMD smaller than 100 mg Ca-HA/ml) failed at the posterior side.
The mean stiffness of the vertebral bodies during compression was 2054 N/mm (SD: 930 N/mm) and the fracture was measured at a load of 3935 N (SD: 1532 N). The mean shear forces were 10.4 N (SD: 136.2 N) in x-direction and 317 N (SD: 264 N) in y-direction while the bending moment around the x-direction (flexion) was 15.6 Nm (SD: 15.3 Nm) and 0.08 Nm (SD: 8.15 Nm) around the y-direction (lateral bend).
Spearman correlation coefficients of the BMD (95% confidence interval in brackets) versus the parameter measured during fracture generation; p-value smaller 0.05 defines a significant correlation
Spearman correlation coefficients of the BMD (95% confidence interval in brackets) versus the parameter measured during fracture generation; p-value smaller 0.05 defines a significant correlation
The Influence of trabecular BMD on the stiffness and fracture force in each direction; lines showed linear fitting curve with 90% confidence interval; Stiffness, fracture force in z- and y-direction showed good correlation while the fracture force in x-direction showed no correlation.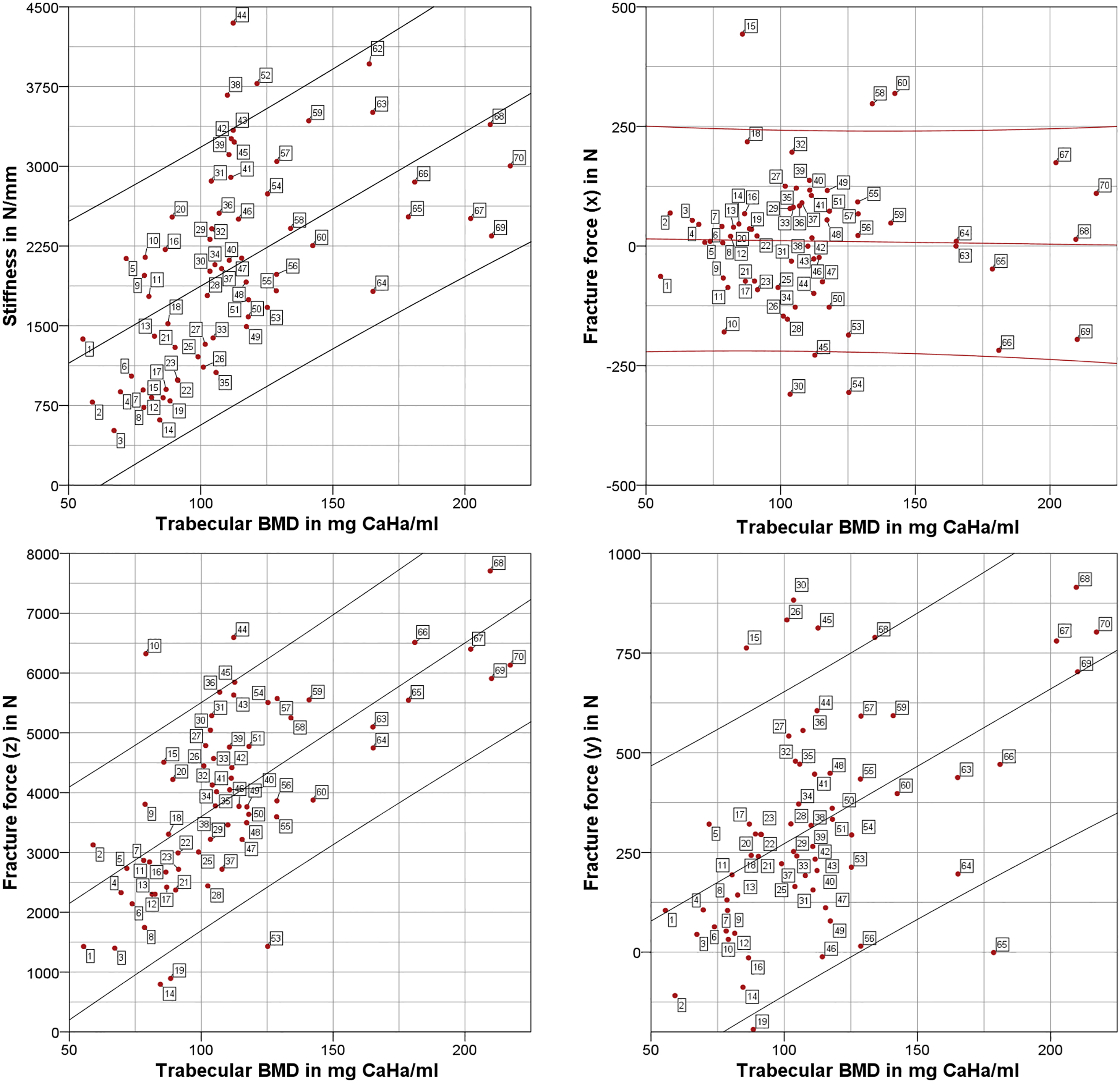
Fracture force in y- and z-direction as well as stiffness showed a positive correlation to BMD measurements (Fig. 4). Another positive correlation was found between the height of the specimens and the cortical BMD while the trabecular BMD showed no correlation (Table 3). The shear force in the transversal axis (x) showed no correlation to the BMD.
The aim of this study was to design and to construct a testing device that is able to simulate standardized compression fractures. The set-up is simple to handle and yields reproducible results in a short period of time. For example, one component of the model is an X-Y-table for the exact position of the vertebrae in relation to the compression force. The configuration of the upper adapter with a ball joint causes the typical compression fracture in the anterior area of the vertebral body. Furthermore a six-degrees-of-freedom load cell was used to detect the maximal fracture-causing force. Consequently, our model includes the advantages of existing testing devices [6, 7, 8, 9, 10]. In contrast to the fracture model of Alkalay et al. [5, 6], the force was applied to the whole vertebral body. Because of the leveling of the surfaces of the superior and the inferior end plate with epoxide resin, the applied force did not only load the cortical layer, but also the trabecular core of the vertebral body via the entire endplate surface. In contrast to Heini et al. [9] and Chevalier et al. [13], the upper and lower plates were not parallelized and therefore the natural anatomic shape was maintained. The increase of fracture force related to BMD observed in our study corresponds well with the results of Hansson et al. [14] and Maquer et al. [15]. As a consequence, the more frequent occurrence of vertebral fractures could be connected to this fact.
Some workgroups remove the pedicles as well as the transverse and spinous processes before testing [9, 13]. This is based on the assumption, that these processes might hinder the proper alignment of the vertebral body in relation to the compression load. According to our findings, the pedicles of the vertebral body seem to have only a minor influence on vertebral stiffness and fracture behavior in compression. Out of 70 vertebral bodies, three failed at the posterior side. These three vertebrae had their pedicles removed in combination with a low BMD. It is conceivable, that despite a very careful preparation, a small fissure acting as a stress raiser may have been generated in the posterior cortex during pedicle preparation. Therefore in our opinion, the pedicles should be removed very carefully, ideally with a minimal remaining stump, before simulating a compression fracture.
Our model is a simplified simulation of an overload situation of the human lumbar spine. The function of the intervertebral disc with its Nucleus pulposus is being replaced successfully by an artificial joint. Furthermore the tests were carried out without the dampening effect of the intervertebral disc.
Alkalay et al. and Belkoff et al. reported a stiffness of 536 N/mm and 756 N/mm for osteopenic vertebrae. In this study, a mean stiffness of 2054 N/mm (SD: 930 N/mm) was measured with heterogeneous BMD. In general, the stiffness of the osteopenic vertebrae was less than of those with normal BMD. In contrast, Heini et al. measured a higher stiffness between 2000 N/mm for osteoporotic and 9667 N/mm for normal BMD. They embedded and parallelized the endplates which might be an explanation of the higher stiffness they observed. The measured fracture force (mean 3935 N) was higher than that observed in other studies (1661 N [6]; 2019 N [9] and 2274 N [16]). The loading behavior of those studies was either on the cortical edge of the vertebral body [6] or the endplates were embedded and parallelized [16, 9]. In this study, the endplates were only leveled with a resin, which leads to a wider load distribution on the endplate. The measured shear forces (F(x): 10
Conclusion
We developed an advanced testing device, which generates standardized and reproducible vertebral body compression fractures. The main difference to existing models is the homogeneous force transmission, which was realized by the epoxide resin plates on the top and bottom and the ball joint. This enables an even force distribution on the whole endplate of the vertebral body. Our results showed that this testing set-up successfully generates data, which is comparable to other published studies. In the first test we found a good correlation between the bone mineral density and the stiffness respectively the fracture force of the vertebral bodies. The pedicles seem to have only a small influence on the fracture behavior. However, the investigator has to take care not to produce a stress raiser in the posterior edge while removing the pedicles. This set-up should prove very useful in future research concerning vertebral body compression fractures and their therapies.
Footnotes
Acknowledgments
We express our gratitude to the Friedrich-Baur Foundation for funding this project. Finally, we would like to express our acknowledgement to the people and their families who decided to donate their bodies for research.
Conflict of interest
The authors declare no conflicts of interest related to this research.