Exact positioning of implants and accuracy of alignment are important parameters to provide an long survivorship of endoprostheses after total knee arthroplasty. It was suggested that an alignment within 3 from centerline provides the best long-term survivorship of TKA. Therefore, computer-assisted navigation became more important in TKAs. Another tool to improve the accuracy in TKA is the preoperative planning software.
OBJECTIVE:
Main goal was to determine if advantages of an intraoperative navigation system during TKA can be reached by an exact implementation of a preoperative computer-aided planning.
METHODS:
Based on all patients ( 100) underwent primarily TKA in 2015 and 2016 two groups were declared: (1) conventionally operated TKA without navigation system and (2) operation with an optical navigation system. Data on age, sex, date, operative time, severe complications and preoperative vs. postoperative alignment were collected retrospectively.
RESULTS:
The two groups do not differ in postoperative alignment and frequency of outliers. Furthermore, there was no difference referring to complications and the length of stay in hospital, but operative time was prolonged in the navigation-assisted group.
CONCLUSIONS:
It can be stated that conventional surgical techniques in TKA are as accurate as navigated ones if an exact preoperative computer aided planning is implemented during surgery.
As a common procedure in orthopaedic departments total knee arthroplasty (TKA) is provided for patients suffering from osteoarthritis [1, 2, 3]. To produce good clinical long-term outcomes, positioning of implants and accuracy of reconstruction of the leg axis are required [4, 5]. Several authors suggested that an alignment within 3 of varus or valgus provides the best long-term survivorship of TKA [4, 6]. Therefore, common and already successful surgical techniques (conventional) use a jig-based alignment by extramedullary (EM) or intramedullary (IM) referencing [7, 8, 9]. Of course there could be a lack of accuracy in some cases like massive deformities or compromising soft tissue [10, 11, 12, 13]. EM procedures are more liable to surgical inaccuracy and IM techniques are dependent of the femoral and tibial bone canals.
For this reason, computer-assisted navigation became more important in TKAs with its height in the last decade [14, 15, 16]. Many authors have described a significant improvement due to the mechanical axis and position of implants when a navigation system was used for alignment [17, 18, 19]. Advocates of this technique suggest that navigation in TKA could be a key technology for surgical alignment subjects [4, 20]. Nevertheless, the improvement of accuracy do not lead to superior clinical results yet [21, 22, 23].
Another tool to improve the accuracy in TKA is the preoperative planning software. Main aims of these computer programs are the correct sizing of implants and prevention of problems like femoropatellar overstuffing, a flexion-extension-mismatch with instability or postoperative pain by oversizing of the components [24]. Nevertheless, reliability and accuracy of these digital templates is sobering [25]. If a preoperative planning of the entrance location into the bone canals can improve alignment results in TKA especially for the IM techniques has not considered yet.
So the main goal of this study was to determine if the advantages of using an intraoperative navigation system during TKA can be reached by utilizing and exact implementation of a preoperative computer-aided planning software.
Methods
The Medical Ethics Committee of the Medical Council Westphalia-Lippe approved this study (number of ethical approval: 2016-593-f-S). Informed consent was waived due to the retrospective and observational nature of the study.
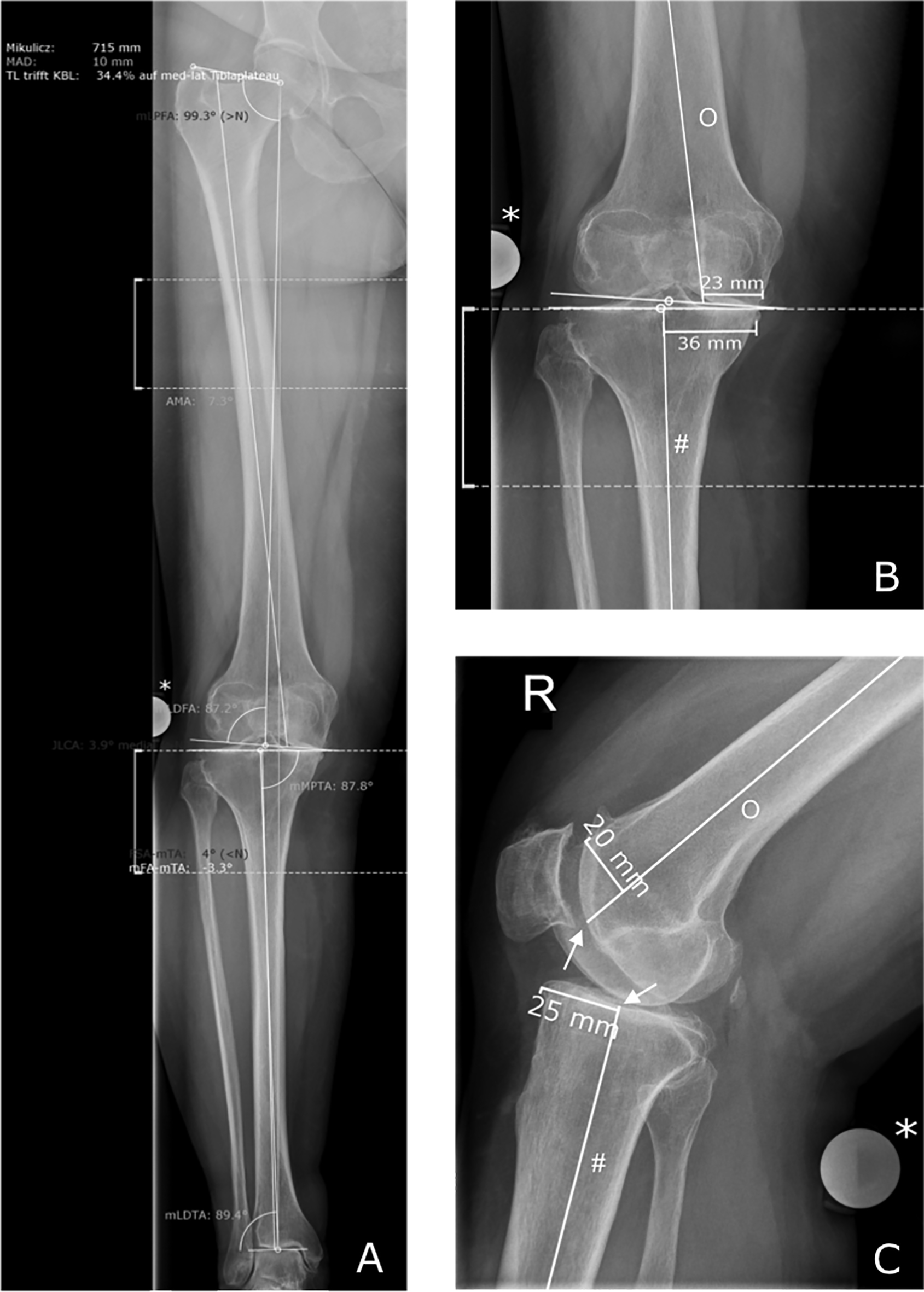
Radiographic images during the preoperative planning process (MediCAD). (A) Complete alignment measurements in the sagittal view (* Reference ball). (B) Sagittal view with measurement of the anatomical axes ( Reference ball, # tibial anatomical axis, O femoral anatomical axis). (C) Coronal view of the same joint (* Reference ball, # tibial anatomical axis, O femoral anatomical axis, arrows mark the important entrance points in the bone canals).
Between January 1 2015 and December 31 2016 167 patients underwent primarily TKA in a German academic teaching. During enrollment 67 patients were excluded due to the following criteria: missing pre- or postoperative leg axis measurement radiographs or missing computer added planning, malrotation of the leg axis measurement radiographs, flexion bearing of the operated knee joint during radiography, implantation of a semi-constrained or a constrained TKA. To reflect results of the power analysis a target dimension of 50 patients for each study arm was defined and data were collected continuously. Concerning this the study is based on all patients ( 100) hospital inclusion criteria with an equal distribution referring to the two study arms. A team of two senior surgeons, certified members of the German Knee Society performed all operations. Patient records in the operation room were kept electronically with a Patient Data Management System (MCC Meierhofer, Meierhofer AG, Munich, Germany). Data on age, sex, date, operative time, severe complications and preoperative vs. postoperative leg axis including data from the navigation system were collected retrospectively. As perioperative complications deep vein thrombosis, pulmonary embolism, cardiac infarction, deep wound infection, and death were defined.
All patients intended for TKA get a preoperative leg axis measurement by anteroposterior and lateral hip-to-ankle radiographs while standing with full weight-bearing. To transfer image data into a computer-aided planning software (MediCAD, HecTec GmbH, Altdorf, Germany) at a ratio of 1:1 a reference metal ball (25 mm diameter) was placed beside the knee joint center lateral or medial of the knee. During the planning process two important values were collected among others: the preoperative leg axis and the exact entrance positions for the intramedullary alignment devices in tow planes (sagittal and coronal) shown in Fig. 1. Measurements were analyzed and recorded blinded to technique allocation by a research associate who was not part of the operative team. Furthermore, two patient groups were identified: (1) conventionally operated TKA without navigation system and (2) operation with an optical navigation system (OrthoPilot, B.Braun Aesculap AG, Tuttlingen, Germany). The Orthopilot collects data via an infrared-camera-system that detects reflecting markers and uses anatomical landmarks which have to declare by the surgeon with a mobile marker. Additionally two reflecting markers were fixed at the diaphysis of the femoral and tibial bone through mini incisions. The complete navigation procedure can be assessed at the manufacture’s homepage [26].
Surgical technique was carried out through a medial parapatellar arthrotomy. All patients were treated with the cruciate ligament sacrifying nonconstrained Columbus knee system (B.Braun Aesculap AG, Tuttlingen, Germany). Components were fixed with bone cement (Palacos, Heraeus Medical, Wehrheim, Germany) after pulsed lavage and blended with a vacuum system. A straight limb axis (0) and a balanced extension and flexion gap was intended in both groups. To improve the alignment in the conventional treated group, bone canal entrance points from the preoperative planning (Fig. 1) were implemented with a ruler. Femoral component rotation was determined by the transepicondylar axis and 3 of external rotation relative to the posterior condyles. Tibial component was placed with 0 slope because Columbus knee provides 3 slope by itself using the ultra-congruent polyethylene inlay.
In summary axis values were taken from the Orthopilot data storage and from the planning software MediCAD pre- and postoperatively. Results are expressed in absolute numbers and frequencies or median and standard error of the median (SE) unless indicated otherwise. In a first step a statistical power analysis was conducted with the software package G*Power to compute the a priori required sample size. Study results are calculated with statistical software package SPSS Version 25 (IBM, Armonk, North Castle, New York, USA). Median differences were tested with the Mann-Whitney-U-test. For the categorical data Chi-Square test and Fisher’s exact test were used.
Results
All patients ( 100) underwent primarily TKA between January 1 2015 and December 31 2016 were included. Fifty percent ( 50) were treated by conventional techniques and 50% ( 50) by navigation-assisted surgery. A balanced median age was found in the both groups with 65 (IQR: 41–80, SE 1.49) in the conventional group and 67 (IQR: 44–82, SE 1.25) in the navigated group ( 0.909). We observe 17 males and 33 females in the manual group and 10 males and 40 females in the navigated group. We compared the gender distribution of the two groups with the chi-square test and get no statistical difference between the manual and navigated group ( 0.176). To exclude a bias the preoperative alignment was compared between each group to ensure that both groups have the same preconditions. There is no statistically significant difference in the preoperative alignment between the groups ( 0.372). While there was no difference referring to the length of stay between the two groups (11d, IQR: 8–17, SE 0.37 conventional vs. 12d, IQR: 7–27, SE 0.57 navigated, 0.175), conventional TKAs could have been performed faster (80 minutes IQR: 55–154, SE 4.14 conventional vs. 119 minutes IQR: 83–166, SE 3.25 navigated, 0.000).
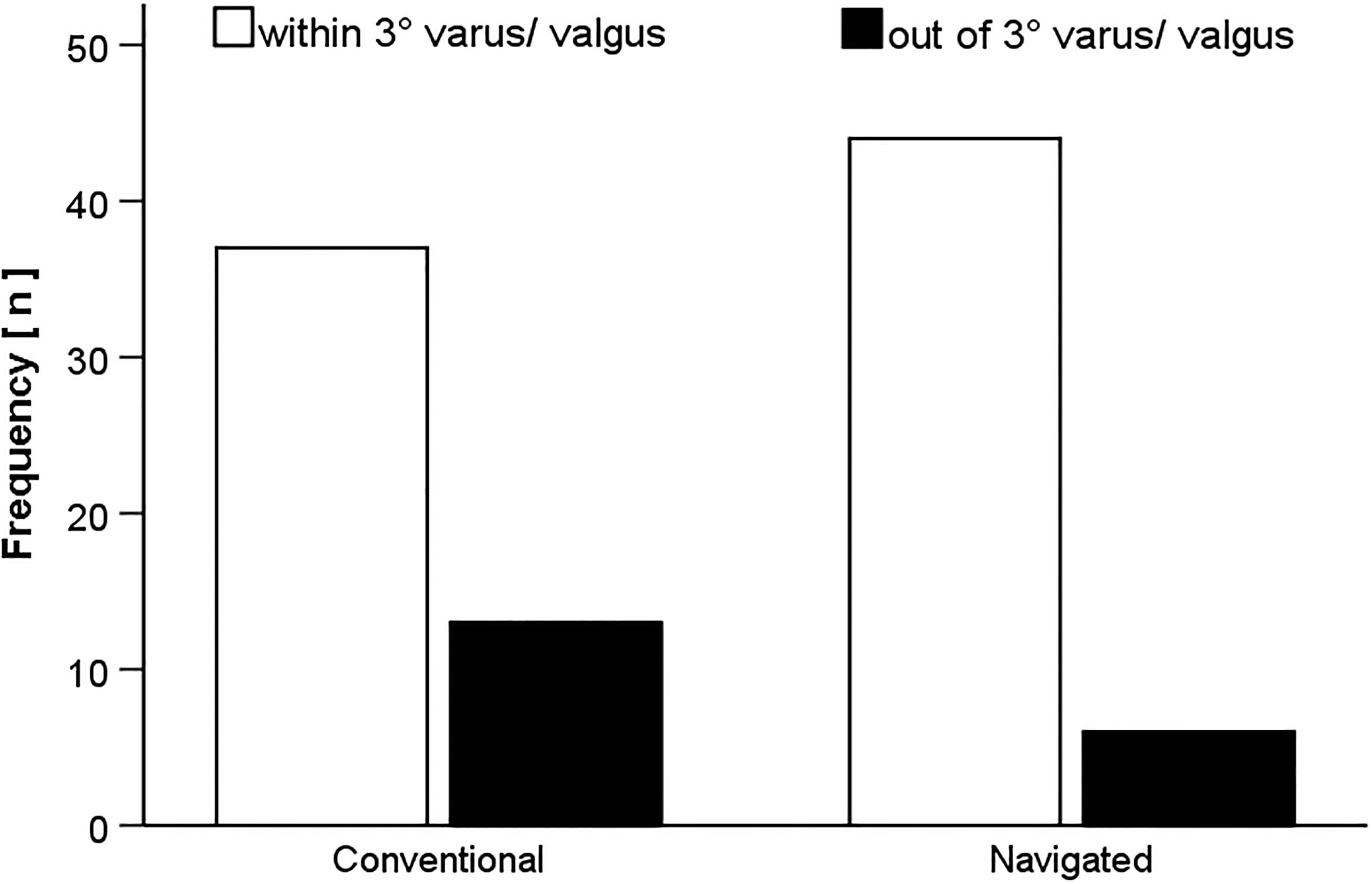
Influence of surgical technique on alignment. Frequency of patients within and out of an alignment within 3 varus or valgus in the conventional and the navigated group.
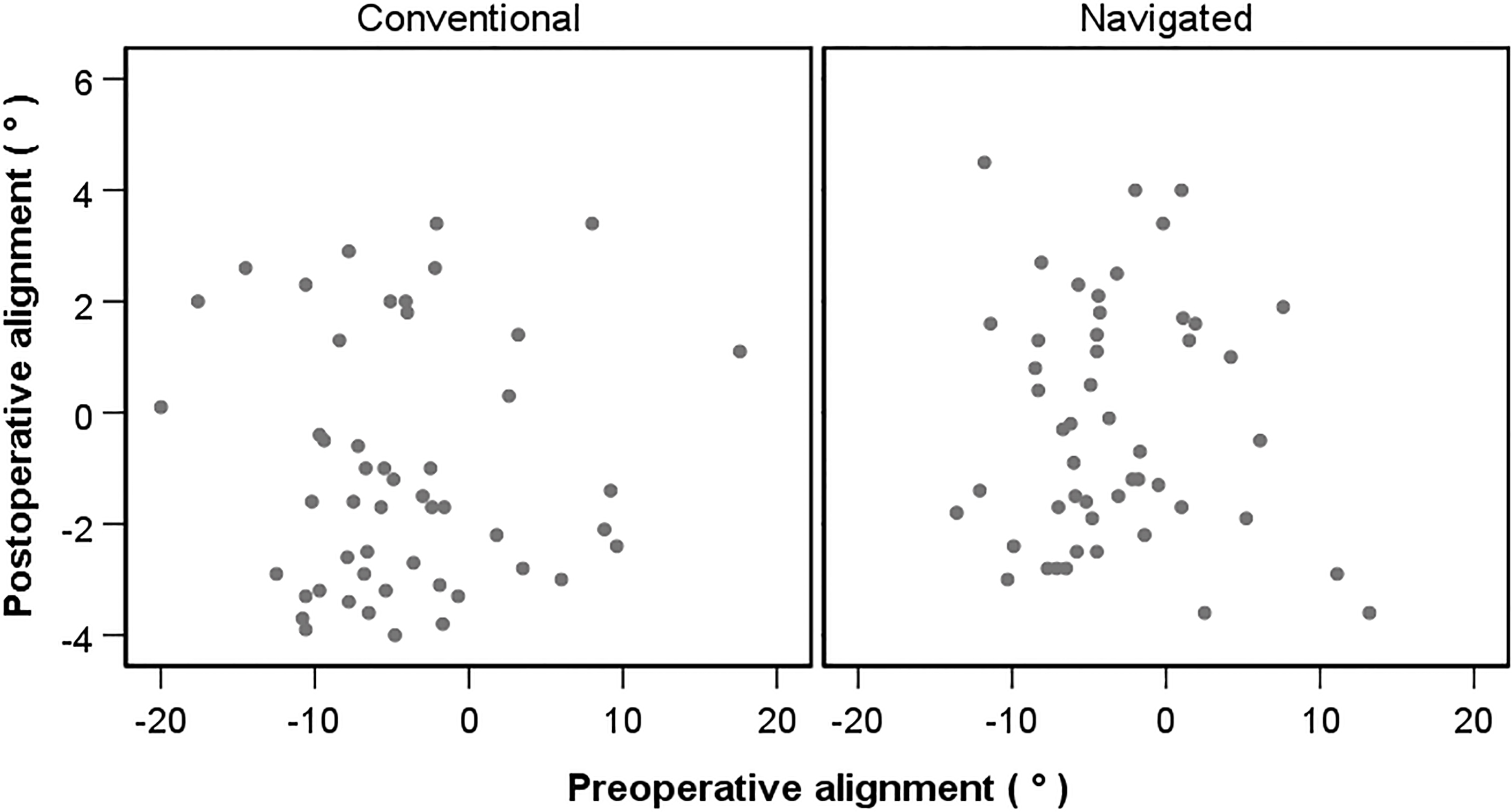
Main aim of this study was an analysis of the accuracy of postoperative alignment after TKA with a conventional surgical technique compared to a navigation-assisted procedure. Figure 2 shows the frequency between a resulting alignment within 3 of varus or valgus (44 in the navigated group vs. 37 in the conventional group) and out of this range (6 in the navigated group vs. 13 in the conventional group). There was no difference found between the two groups and the postoperative alignment ( 0.074). The distribution of the postoperative alignment of both study groups is illustrated in Fig. 3.
Alignment distribution the both groups. Preoperative and postoperative alignment was interrelated for the conventional and the navigated group.
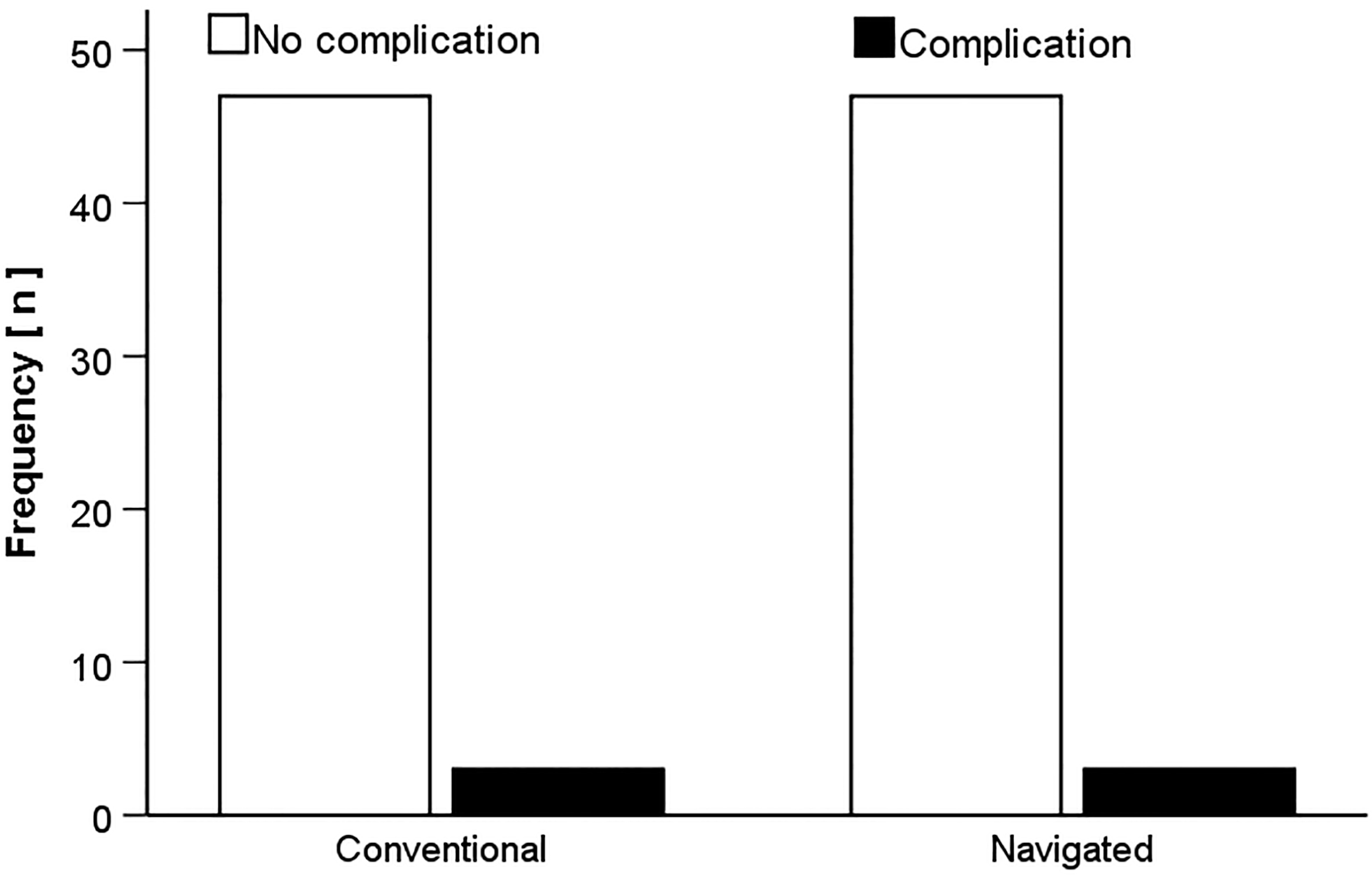
Furthermore, influence upon the complication rate was analyzed for both groups which is shown in Fig. 4. There was no difference ( 0.661).
Influence of surgical technique on complication rate. Frequency of patients suffered from a surgery associated complication in the conventional and the navigated group.
Discussion
Exact positioning of implants and accuracy of alignment are important parameters to provide an long survivorship of endoprostheses after total knee arthroplasty [4, 5]. Therefore it was suggested that a alignment within 3 of varus or valgus provides the best long-term survivorship of TKA [4, 6]. The main aim of this study was to determine, if the advantages of an intraoperative navigation system can be reached by utilizing and exact implementation of a preoperative computer-aided planning software.
Here presented findings suggest that the use of preoperative planning software and an accurate transfer into surgical procedures can provide a postoperative alignment as good as navigation-assisted surgery in TKA. It has been claimed that using a navigation system can improve accurateness of the alignment [16, 27, 28, 29, 30, 31]. In particular some authors suggest that a navigation-assisted technique could prevent higher rates of outliers [28, 29]. Nevertheless study designs (including reviews) are often heterogeneous with a lack of comparability and there is no literature that documents a clinical or functional improvement based on intraoperative navigation [27, 32]. By contrast, in the current and other studies there could not found any advantage by using a navigation system referring to an accurate alignment within 3 of varus/valgus after TKA [32, 33, 34]. Our findings suggest that a better control of the conventional alignment by preoperative computer aided planning and as exact as possible implementation of the findings into the surgical technique, in particular by find the bone canal entrance points, could be an important tool to reach results like navigated procedures.
Biasca and colleagues describe a reduction of the length of stay in hospital for navigated procedures and no difference in the operative time [33]. Both findings cannot be confirmed by data of the presented study. A longer operative time was recognized in the navigation group, while there was no difference referring to the length of stay. Other study groups confirmed our findings referring to the operative time [5, 31]. Presented results of the current study referring to severe perioperative complications do not show differences between the two study groups. These findings correlate to others in the actual literature [31, 34]. In summary, conventional and navigated procedures during TKA do not differ in their impact on the length of stay in hospital and severe complications like deep wound infection instead of a prolonged operative time for navigated techniques.
Limitations of the current study have to mentioned. Coronal plane as a parameter for alignment could not guarantee an accurate implant position over the full range of motion. Notably, like others this study cannot show differences referring to the rotational alignment [17, 26, 27]. Furthermore, a limitation of outliers could has been aroused by the fact that a skilled senior surgeon has performed all arthroplasties.
In summary, it can be stated that conventional surgical techniques in TKA are as accurate as navigated ones if an exact preoperative computer aided planning is implemented during surgery. Probably, an important tool to reach this accurateness is the femoral and tibial intramedullary alignment, which is able to reproduce planning parameters easier than during extramedullary procedures. Advantages of conventional surgery like faster surgery duration, no investment and maintenance costs for the navigation system, and no additional incisions or drill holes should be mentioned, too.
Footnotes
Conflict of interest
All authors declare that there is no potential conflict of interest and no specific funding.
References
1.
GandhiRDhotarHRazakFTsoPDaveyJRMahomedNN. Predicting the longer term outcomes of total knee arthroplasty. Knee2010; 17(1): 15-8. doi: 10.1016/j.knee.2009.06.003.
2.
FooteJASmithHKJonasSCGreenwoodRWealeAE. Return to work following knee arthroplasty. Knee2010; 17(1): 19-22. doi: 10.1016/j.knee.2009.06.001.
3.
JulinJJämsenEPuolakkaTKonttinenYTMoilanenT. Younger age increases the risk of early prosthesis failure following primary total knee replacement for osteoarthritis. A follow-up study of 32,019 total knee replacements in the Finnish Arthroplasty Register. Acta Orthop2010; 81(4): 413-9. doi: 10.3109/17453674.2010.501747.
4.
RosenbergerREHoserCQuirbachSAttalRHennerbichlerAFinkC. Improved accuracy of component alignment with the implementation of image-free navigation in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc2008; 16(3): 249-57.
5.
KimYHParkJWKimJS. Computer-navigated versus conventional total knee arthroplasty a prospective randomized trial. J Bone Joint Surg Am2012; 94(22): 2017-24.
6.
BolognesiMHofmannA. Computer navigation versus standard instrumentation for TKA: a single-surgeon experience. Clin Orthop Relat Res2012; 440: 162-9.
7.
RobertssonOBizjajevaSFenstadAMFurnesOLidgrenLMehnertFOdgaardAPedersenABHavelinLI. Knee arthroplasty in Denmark, Norway and Sweden. A pilot study from the Nordic Arthroplasty Register Association. Acta Orthop2010; 81(1): 82-9. doi: 10.3109/17453671003685442.
8.
LygreSHEspehaugBHavelinLIVollsetSEFurnesO. Failure of total knee arthroplasty with or without patella resurfacing. Acta Orthop2011; 82(3): 282-92. doi: 10.3109/17453674.2011.570672.
9.
GillamMHRyanPGravesSEMillerLNde SteigerRNSalterA. Competing risks survival analysis applied to data from the Australian Orthopaedic Association National Joint Replacement Registry. Acta Orthop2010; 81(5): 548-55. doi: 10.3109/17453674.2010.524594.
10.
BrinYSNikolaouVSJosephLZukorDJAntoniouJ. Imageless computer assisted versus conventional total knee replacement. A Bayesian meta-analysis of 23 comparative studies. Int Orthop2011; 35(3): 331-9. doi: 10.1007/s00264-010-1008-6.
11.
MahaluxmivalaJBankesMJNicolaiPAldamCHAllenPW. The effect of surgeon experience on component positioning in 673 Press Fit Condylar posterior cruciate-sacrificing total knee arthroplasties. J Arthroplasty2001; 16(5): 635-40.
12.
LustigSFleuryCGoyDNeyretPDonellST. The accuracy of acquisition of an imageless computer-assisted system and its implication for knee arthroplasty. Knee2011; 18(1): 15-20. doi: 10.1016/j.knee.2009.12.010.
13.
ChengTZhaoSPengXZhangX. Does computer-assisted surgery improve postoperative leg alignment and implant positioning following total knee arthroplasty? A meta-analysis of randomized controlled trials? Knee Surg Sports Traumatol Arthrosc2012; 20(7): 1307-22. doi: 10.1007/s00167-011-1588-8.
14.
LehnenKGiesingerKWarschkowRPorterMKochEKusterMS. Clinical outcome using a ligament referencing technique in CAS versus conventional technique. Knee Surg Sports Traumatol Arthrosc2011; 19(6): 887-92. doi: 10.1007/s00167-010-1264-4.
15.
HasegawaMYoshidaKWakabayashiHSudoA. Minimally invasive total knee arthroplasty: comparison of jig-based technique versus computer navigation for clinical and alignment outcome. Knee Surg Sports Traumatol Arthrosc2011; 19(6): 904-10. doi: 10.1007/s00167-010-1253-7.
16.
ChengTPanXYMaoXZhangGYZhangXL. Little clinical advantage of computer-assisted navigation over conventional instrumentation in primary total knee arthroplasty at early follow-up. Knee2012; 19(4): 237-45. doi: 10.1016/j.knee.2011.10.001.
17.
BäthisHPerlickLTingartMLüringCZurakowskiDGrifkaJ. Alignment in total knee arthroplasty. A comparison of computer-assisted surgery with the conventional technique. J Bone Joint Surg Br2004; 86(5): 682-7.
18.
ChoongPFDowseyMMStoneyJD. Does accurate anatomical alignment result in better function and quality of life? Comparing conventional and computer-assisted total knee arthroplasty. J Arthroplasty2009; 24(4): 560-9. doi: 10.1016/j.arth.2008.02.018.
19.
Hernández-VaqueroDSuarez-VazquezASandoval-GarciaMANoriega-FernandezA. Computer assistance increases precision of component placement in total knee arthroplasty with articular deformity. Clin Orthop Relat Res2010; 468(5): 1237-41. doi: 10.1007/s11999-009-1175-1.
20.
InsallJNScuderiGRKomistekRDMathKDennisDAAndersonDT. Correlation between condylar lift-off and femoral component alignment. Clin Orthop Relat Res2002; 403: 143-52.
21.
SchmittJHaukCKienapfelHPfeifferMEfeTFuchs-WinkelmannSHeyseTJ. Navigation of total knee arthroplasty: rotation of components and clinical results in a prospectively randomized study. BMC Musculoskelet Disord2011; 12: 16. doi: 10.1186/1471-2474-12-16.
22.
HiscoxCMBohmERTurgeonTRHeddenDRBurnellCD. Randomized trial of computer-assisted knee arthroplasty: impact on clinical and radiographic outcomes. J Arthroplasty2011; 26(8): 1259-64. doi: 10.1016/j.arth.2011.02.012.
23.
YangJHYoonJRPandherDSOhKJ. Clinical and radiologic outcomes of contemporary 3 techniques of TKA. Orthopedics2010; 33(10 Suppl): 76-81. doi: 10.3928/01477447-20100510-59.
24.
TrickettRWHodgsonPForsterMCRobertsonA. The reliability and accuracy of digital templating in total knee replacement. J Bone Joint Surg Br2009; 91(7): 903-6. doi: 10.1302/0301-620X.91B7.21476.
25.
VaninNKenawayMPanzicaMJagodzinskiMMellerRKrettekCHankemeierS. Accuracy of digital preoperative planning for total knee arthroplasty. Technol Health Care2010; 18(4–5): 335-40. doi: 10.3233/THC-2010-0598.
26.
BraunBAesculapAG. Orthopilot TKA Suite. http://www.bbraun.com/en/products-and-therapies/orthopaedic-joint-replacement/orthopilot/kneesuite/tka.html. Accessed October 30th 2017.
27.
HetaimishBMKhanMMSimunovicNAl-HarbiHHBhandariMZalzalPK. Meta-analysis of navigation vs conventional total knee arthroplasty. J Arthroplasty2012; 27(6): 1177-82. doi: 10.1016/j.arth.2011.12.028.
28.
PangCHChanWLYenCHChengSCWooSBChoiSTHuiWKMakKH. Comparison of total knee arthroplasty using computer-assisted navigation versus conventional guiding systems: a prospective study. J Orthop Surg (Hong Kong)2009; 17(2): 170-3.
29.
ChengTZhangGZhangX. Imageless navigation system does not improve component rotational alignment in total knee arthroplasty. J Surg Res2011; 171(2): 590-600. doi: 10.1016/j.jss.2010.05.006.
30.
FuYWangMLiuYFuQ. Alignment outcomes in navigated total knee arthroplasty: a meta-analysis. Knee Surg Sports Traumatol Arthrosc2012; 20(6): 1075-82. doi: 10.1007/s00167-011-1695-6.
31.
AlcelikIABlomfieldMIDianaGGibbonAJCarringtonNBurrS. A Comparison of Short-Term Outcomes of Minimally Invasive Computer-Assisted vs Minimally Invasive Conventional Instrumentation for Primary Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. J Arthroplasty2016; 31(2): 410-8. doi: 10.1016/j.arth.2015.09.013.
32.
KimYHParkJWKimJS. Computer-navigated versus conventional total knee arthroplasty a prospective randomized trial. J Bone Joint Surg Am2012; 21; 94(22): 2017-24.
33.
BiascaNWirthSBungartzM. Mechanical accuracy of navigated minimally invasive total knee arthroplasty (MIS TKA). Knee2009; 16(1): 22-9. doi: 10.1016/j.knee.2008.09.010.
34.
KimYHParkJWKimJS. The Clinical Outcome of Computer-Navigated Compared with Conventional Knee Arthroplasty in the Same Patients: A Prospective, Randomized, Double-Blind, Long-Term Study. J Bone Joint Surg Am2017; 99(12): 989-996. doi: 10.2106/JBJS.16.00791.