
Abstract
BACKGROUND:
Poor postural control constitutes a major impairment in children with cerebral palsy (CP), compromising everyday activities such as sitting- and standing-position.
PURPOSE:
In this study, we measured trunk sway during sitting- and standing-position. Additionally, we assessed trunk control ability using the trunk impairment scale (TIS), trunk control measurement scale (TCMS), and sitting assessment test for children with neuromotor dysfunction (SACND), in children with CP.
METHODS:
Fifteen children (10 boys and 5 girls) were recruited for this study. Trunk sway was measured using a triaxial accelerometer that recorded variation in movement acceleration during quiet sitting- and standing-position.
RESULTS:
Anterior-posterior (AP) acceleration was significantly greater in the standing position than the sitting position (
CONCLUSION:
Measurement of trunk sway using a triaxial accelerometer revealed a moderate correlation with trunk control test data and excellent reliability. Our findings suggest that measurement of trunk sway using a triaxial accelerometer is not time-consuming, and is simple and easy. Our approach can be applied in clinical settings to gain information on trunk control in children with CP.
Introduction
Postural control is achieved by subconscious coordinated muscle activity in space to stabilize the body position or optimize postural alignment [1]. Stability refers to the ability to maintain the center of mass (COM) within the base of support (BOS) throughout static or dynamic actions [2]. Generally, the size of the BOS influences the ability to control trunk posture regardless of the severity of a disability [3]. Postural control plays a primary role during functional movements and the activities of daily living such as sitting, standing, and reaching [4, 5]. Poor postural control constitutes a major impairment in children with cerebral palsy (CP), negatively influencing everyday activities [6]. In addition, most children with CP spend much of their time sitting- and standing-position. Therefore, it is necessary to evaluate trunk control ability in these positions.
Trunk sway is correlated with functional activities in children with CP [5]. In addition, it is thought to be an indicator of balance control ability [7]. Generally, trunk sway is based on excursions of the COM and the center of pressure (COP), which is defined as the sum of the ground reaction forces required to restore equilibrium between the feet and a supporting surface, and is derived using a force plate [8]. Analysis of COM acceleration and COP displacement is considered the gold standard when studying human postural control [9]. However, the experimental system is bulky, and the work is complicated, time-consuming, and expensive. Recently, trunk sway assessment using a triaxial accelerometer has been suggested, as the devices are portable, simple, and inexpensive [10]. Hence, accelerometers can be used in real-world clinical settings, and a laboratory is not necessary [11].
Several investigators have used triaxial accelerometers to assess trunk sway in the elderly [12], ataxic patients [13], and typical children [14]. However, no study has used triaxial accelerometers to measure trunk sway in children with CP. Therefore, the primary purpose of this study was to measure trunk sway during sitting- and standing-position; to assess trunk control ability using the trunk impairment scale (TIS), trunk control measurement scale (TCMS), and the sitting assessment test for children with neuromotor dysfunction (SACND), in children with CP. The secondary purpose was to calculate correlations between the trunk sway measured with a triaxial accelerometer and the results of the trunk control tests (TIS, TCMS, and SACND) during both sitting- and standing-position. Clinically, this measurement technique provides the important information on trunk control for clinicians in children with CP and thus enables clinicians to make better clinical decisions.
Methods
Subjects
This study was approved by the Faculty of Health Science Human Ethics Committee of Inje University (Approval No. 2017-01-012) and conducted in accordance with all of the relevant dictates of the Declaration of Helsinki. Prior to the study, all of the caregivers provided written informed consent. A power analyses were performed to calculate sample size using G-Power 3.1 version software (University of Dusseldorf, Dusseldorf, Germany). A target sample size of 10 children was defined based on the results of a pilot test on 5 children. We estimated an effect size of 1.14, a power of 80%, and an alpha probability of 0.05 using the two-tailed test. As the estimated sample size was 10, we recruited 15 children (10 boys and 5 girls) in this study, to allow for dropout. The inclusion criteria were: diagnosis of CP by computed tomography (CT) or magnetic resonance imaging, age between 7 and 13 years, an ability to understand instructions of the researchers, and gross motor function classification system (GMFCS) levels of I to III [15]. Demographic and clinical characteristics of the children with CP are listed in Table 1.
Clinical characteristics of the 15 children with cerebral palsy
Clinical characteristics of the 15 children with cerebral palsy
A triaxial accelerometer (Fitmeter, Fit.Life Inc., Suwon, Korea) was used to evaluate trunk sway by calculating variation in trunk movement acceleration. The accelerometer is a box 35
Trunk impairment scale
The TIS was used to assess trunk control including static- and dynamic-sitting balance, and upper and lower trunk coordination during trunk rotation while sitting [18]. The static balance tests were organized as follows: maintaining a sitting position for 10 s with the feet supported but without back or arm support, maintaining a sitting position while the legs were held crossed by a therapist, and maintaining a sitting position during active crossing of the legs. The dynamic balance items were contacting the treatment table with the elbow and returning to the starting position; and lifting the hip from the treatment table, and then setting it down again. The coordination of dynamic balance items were rotating the upper trunk six times, and turning the lower trunk six times. Each item was graded on a 2–4-point ordinal scale. The highest possible scores for the static- and dynamic-sitting balance tests, and the trunk coordination test, were 7, 10, and 6, and the total TIS score ranged from 0 to 23. Each item of the TIS was tested three times and the highest score counted. No practice was allowed [19]. The validity of the TIS has already been proven. Saether et al. [20] found that the TIS total score significantly correlated with the gross motor function measure (GMFM), which was between 0.62 and 0.82 in children with CP. Intra-and inter-rater reliability of the TIS were excellent [ICC (1, 1)
Trunk control measurement scale
The TCMS was developed to test trunk control in the sitting position. The subscales evaluate static- and dynamic-sitting balance and dynamic reaching (equilibrium reactions). The static-sitting balance subscale measures trunk control in five positions. The dynamic-sitting balance subscale evaluates selective trunk movement control during forward, backward, and sideward leaning; and rotation. The dynamic reaching subscale assesses forward-, sideward-, and cross-midline-reaching. The total scale includes 15 items and the test was repeated three times. The best score was used for analysis. All of the items were graded using 2 to 4-point ordinal scales. The overall score of the TCMS varies between 0 and 58, and a higher score reflects better trunk control during all tests. The intra-and inter-rater reliability of the TCMS are excellent [ICC (1, 1)
The sitting assessment test for children with neuromotor dysfunction
The SACND was utilized to evaluate trunk ability during sitting [22]. The SACND includes rest and reach modules. Each module measures the quality of sitting skill in terms of postural tone, proximal stability, postural alignment, and balance. Each test is graded on a 4-point ordinal scale. Therefore, the best scores for the rest and reach modules were both 4, indicating that the subject is normal. The total SACND score ranged from 8 to 32. Several studies have evaluated SACND validity and reliability. An inter-rater reliability study showed that the Kappa statistic was excellent, ranging from 0.91 to 1.00. Furthermore, the intra-rater reliability was good (Kappa statistic 0.87 to 1.00) [23].
Statistical analysis
All of the results are expressed as means with standard deviations (SDs). The Wilcoxon signed-rank test was used to compare triaxial accelerometer data between the sitting- and standing-position. To evaluate test-retest reliability, we estimated intraclass correlation coefficients (ICCs 3,1). Pearson’s rank correlation coefficients were calculated to estimate correlations between trunk control test results and triaxial accelerometer data. All of the statistical analyses were performed with the aid of PASW Statistics software (ver. 20; Norusis/SPSS Inc., Chicago, IL, USA). The level of statistical significance was set at a two-tailed
Results
AP trunk acceleration was significantly greater in the standing position (57.27
Main outcomes of parameters expressing trunk control
Main outcomes of parameters expressing trunk control
TIS
Trunk acceleration in sitting and standing.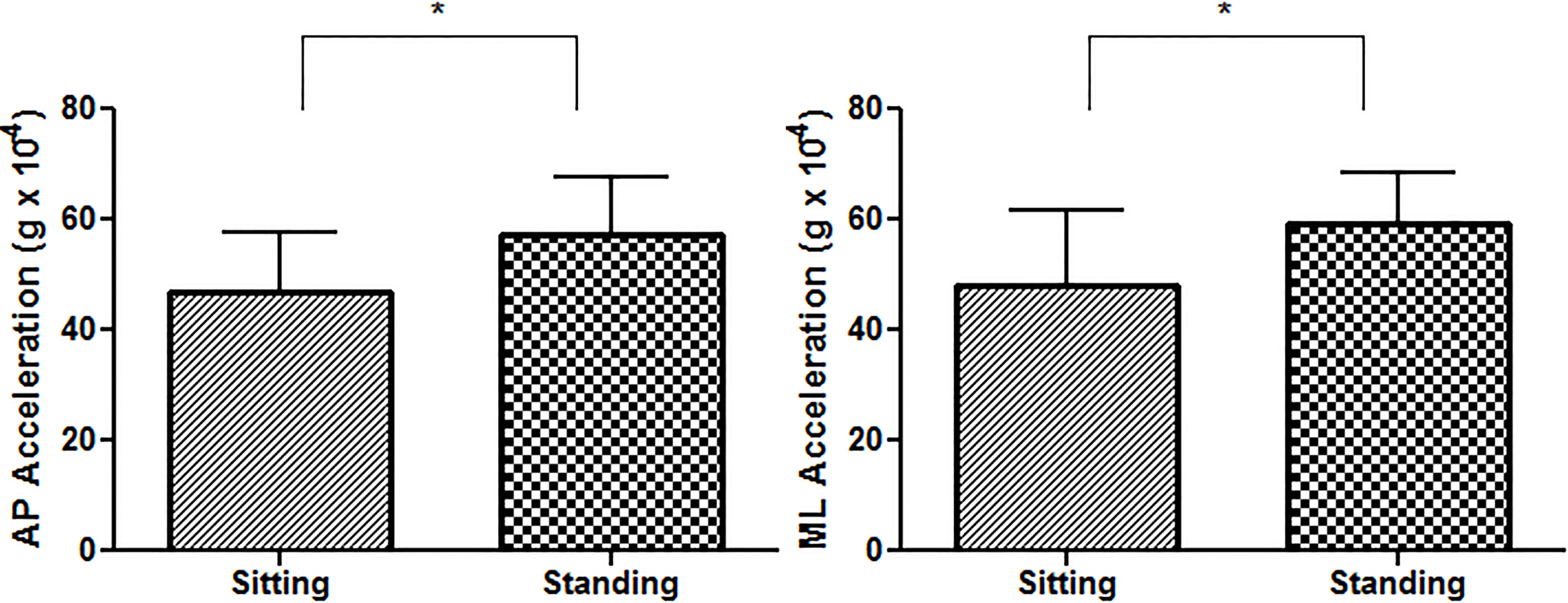
We measured trunk sway using a triaxial accelerometer during sitting- and standing-position; assessed trunk control ability using the TIS, TCMS, and SACND tests, in children with CP. To the best of our knowledge, this is the first clinical study comparing trunk acceleration between the sitting- and standing-position and calculating correlations between trunk control test results and triaxial accelerometer data. We found that trunk acceleration in the standing position was significantly greater than in the sitting position. Moreover, trunk acceleration correlated moderately with the TIS, TCMS, and SACND results.
Triaxial accelerometer data revealed that the AP and ML acceleration were 23% and 22% greater in the standing position than the sitting position. Similarly, Curtis et al. [14] showed that the AP and ML sway velocity were 0.54 mm/s and 0.21 mm/s and the AP and ML sway amplitude were 2.05 mm and 0.53 mm in the sitting position in 20 typically developing children. Saether et al. [24] reported that the AP and ML acceleration were 2.30 RMS and 2.55 RMS during gait in 26 children with CP, respectively. Moe-Nilssen and Helbostad [10] compared trunk sway between eyes closed and eyes open during quiet standing in young and elderly healthy subjects. In the cited study, mean difference of the trunk AP and ML acceleration were 38 g
We evaluated reliability and validity using two special measures. The TIS static- and dynamic-sitting balance subscale data correlated moderately with trunk acceleration (
Clinically, we suggest that trunk acceleration should be measured when evaluating therapeutic effects and assessing clinical postural control in children with CP. It is not necessary to use complex tools. In addition, we propose that assessing trunk acceleration under various conditions (such as sitting and standing) is useful to accurately evaluate postural control ability.
This study had three main limitations that should be considered when planning future studies. First, it had a small sample size; thus the findings should be interpreted with care. However, we calculated sample size by reference to a power analysis based on the results of a pilot study. Further studies with larger sample sizes are required. Second, we did not compute the intra-rater reliability of the triaxial accelerometer data. Therefore, future studies should calculate intra-rater reliability. Finally, with respect to the influence of elements on postural control, researches were found on muscle strength, electromyography (EMG) activity, COP velocity, acceleration, visual information, and seat surface. However, in this study, we focused on trunk acceleration. Therefore, caution is needed in the interpretation. Future studies will require multiple regression analysis to determine which elements are most associated with postural control.
Conclusion
Measurements of trunk sway using a triaxial accelerometer exhibited moderate negative correlations with TIS and TCMS data, and a moderate and positive relationship with SACND data. In addition, the accelerometer data exhibited excellent reliability. Our findings suggest that measurement of trunk acceleration using a triaxial accelerometer is not time-consuming, and is simple and easy. Moreover, our approach can be used in the clinical settings to collect information on trunk sway and trunk control ability in children with CP.
Footnotes
Conflict of interest
None to report.