
Abstract
BACKGROUND:
The Human Body Posturizer (HPB), an innovative therapeutic tool able to correct postural changes dynamically, fits perfectly in this framework.
OBJECTIVE:
The aim of this paper is to consider the potential economic benefits of using the Human Body Posturizer both in terms of direct and indirect cost reduction in one year.
METHODS:
This study was carried out using an estimation method in order to investigate the possible economic impact related to the adoption of the HBP in subjects with low back pain as an attempt to quantify the costs (direct and indirect) generated at different levels of the path therapeutic.
RESULTS:
The use of therapy with HBP would generate a saving of € 971.40/year in case of sub-acute LBP and amounted to € 2,922.90/year in case of chronic low back pain.
CONCLUSION:
This paper provides guidance on the potential economic benefits resulting from the adoption of the Human Body Posturizer as an innovative therapeutic approach by the Italian Health System.
Introduction
During the recent years, at both national and international levels, the importance of the clinical and epidemiological of back pain has thrived a lot of studies and guidelines in order to systematize the diagnostic therapeutic approach [1, 2, 3, 4]. Over the past two decades, the back pain treatment offer has been mushrooming, those treatments are related to the various stages of the disease: acute, sub-acute, and chronic [2, 5].
At both national and international levels, the most recommended treatments have a similar pharmacological approach to back pain, both acute and chronic, by administering painkillers and muscle relaxant [6, 7, 8]. In addition, for the non-drug treatment of the acute low back pain, the guidelines [2, 5] suggest the practice of physical activity nonspecific, but preferably if it is a sport.
The indications were controversial for the invasive treatments, which explain why they were not recommended from the national guidelines in opposite to the American [1] and the English [5] that recommend acupuncture only for subjects with acute and chronic low back.
The literature suggests to consider such invasive therapies only with selected patients who have already carried out a clinical and therapeutic for a sufficient period of time, according to various authors, varies between 6 months and 2 years [6, 7, 9, 10].
The clinical and epidemiological importance of back pain has meant that in recent years proliferate studies and guidelines, both nationally and internationally, in order to systematize the diagnostic and therapeutic approach [1, 4, 5, 6, 7, 8]. The offer of “treatments for back pain” proposal over the past two decades is extremely wide.
The variety of suggested approaches is closely related to the various stages of the disease:
Acute: duration of less than 30 days (4 weeks); Sub acute: from 30 to 90 days (8 weeks); Chronic: increased duration to 90 days (over 12 weeks).
Within the latter framework, the Human Body Posturizer (HPB), an innovative therapeutic tool able to correct postural changes dynamically, fits perfectly. The HPB is an orthosis consists of a system of multiple components articulated between each other that allow the subject to modify their postural alignment in static equilibrium [7].
The components, assembled together, have specifically the role of maintaining, in the context of normality, the various anatomical regions with respect to the neutral position (orthostatism). Wearing the orthosis may be able to get a trim optimal static posture. The individual may as well carry more physical activity suited to its characteristics. Each component of the structure is in contact with various anatomical sites and, modeling itself to any type of posture the body have, it allows to carry out normal daily activities without any discomfort.
Starting from a descriptive study, some authors have recently estimated the effectiveness of the Human Body Posturizer in terms of muscle rebalancing [7]. The analysis was performed by evaluating the changes in the morphology of the back in terms of space of different points on subjects who are athletes, who had some asymmetries and paramorphism. Despite that the study results are preliminary, they present a positive frame in terms of the HBP applications both in the therapeutic field, and in the prevention of disfunctionpostures [7, 11, 12].
Any medical condition brings with itself multiple effects regarding “concentric circles of subjects” ranging from where the patient is directly involved, to its relational networks, to the vital worlds in which it operates. Considering the low back pain, if you consider the total of patients who are affected and the multiple consequences, we can say that the economic and the social impact can be very significant, both as direct and indirect costs, as well as the costs in between, even as intangibles costs [7, 13]. Direct costs consists mainly of expenses closely related to the disease (prevention, diagnosis and treatment) and include costs of procedures and medical services, hospitalization, patient’s visits and drug prescriptions [14].
Indirect costs include the value of lost productivity in the workplace due to the absence caused only by illness, early retirement, psychosocial and death reasons [10]. Immaterial costs quantify subjective factors such as quality of life, leisure and pain [11].
Comparison of therapeutic pathways (P). Source: our processing. DGM 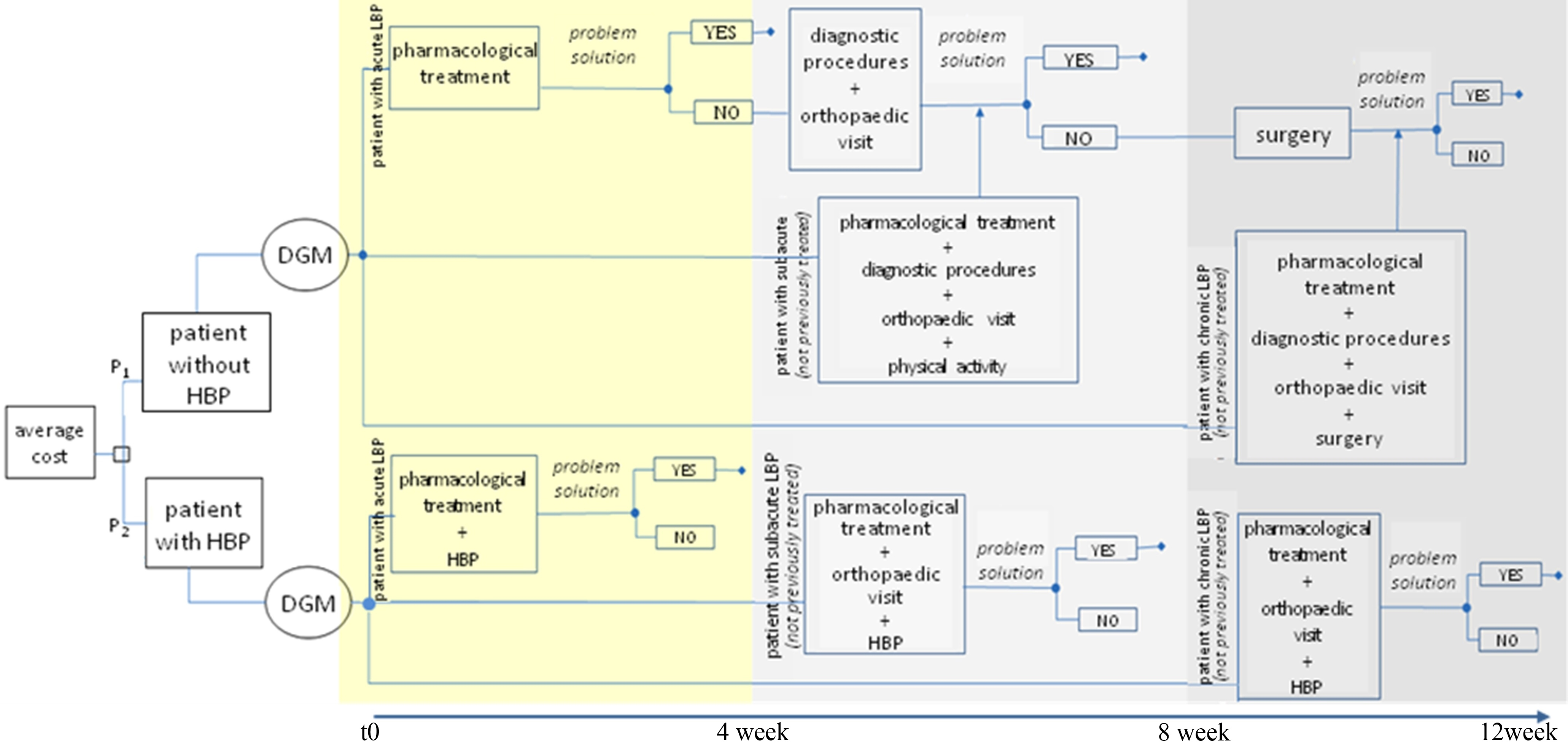
In particular, with regard to indirect costs, back pain represents the 13% of accidents and 20% of interruptions in their careers, although with certain geographical variations [7]. Some surveys conducted in the UK, report that back pain is the leading cause of disability in young adults, with more than 100 million of lost working days/year, with an average of 32.6 days of illness/100 of work; 4% of young adults have to change their jobs every year because of the vertebral column pathologies [13].
In Scandinavian countries, the average days of absence in work for low back pain reasons is even greater, and can be up to 36 days/100 days of work [14].
In the USA, back pain is the most common and costly cause of disability in work [13, 15] and a frequent cause of lost work days, with estimations that refer approximately to 149,000 days of work/year [4, 16, 17, 18]. In addition, among US workers aged between 40–65 years, the exacerbation of back pain, and the resulting loss of productivity, cost employers approximately 7.4 billion/year, of which 71.6% due for lack of workers with chronic sore back [19]. INAIL – National Institute for Insurance against Accidents at Work – estimates that in Italy each year there are 30 million working hours lost because of back sickness [20].
The aim of this paper is to consider the potential economic benefits of using the Human Body Posturizer both in terms of direct and indirect cost reduction in one year.
Materials and methods
This study was carried out using an estimation method in order to investigate the possible economic impact related to the adoption of the HBT in subjects with low back pain as an attempt to quantify the costs (direct and indirect) generated at different levels of the path therapeutic [21, 22]. The Fig. 1 summarize what we are going to discuss through a structure of a decision tree.
Unit detail for sanitary indirect costs and direct costs
Unit detail for sanitary indirect costs and direct costs
Specifically, the comparison between the average cost of a patient who follows the traditional path (P1) and the one who decides to take the exoskeleton HBP (P2) was formalized.
The financial value used for the assessment of costs (and benefits) is represented by market prices. In the case of the health sector, given the uncertainty of the “price” to be attributed to the disease, it has resorted to an approximate methodology in order to provide an indirect measure of the value in question.
The costs of an individual items, from national rate extracts, are listed in Table 1. They were excluded from the calculation, because it is difficult to find, non-medical costs (indirect costs), such as: transportation, complementary and alternative treatments, intangible costs.
In relation to the drug therapy, for each active ingredient (acetaminophen, ibuprofen, diazepam) it was taken as a reference the average cost of a generic drug, selecting the market supply deemed most suitable to the administration indications suggested by the literature.
With reference to item h, “Measures of hernia, except inguinal and femoral, age
List direct and indirect costs (in €) – P1 and P2
Notes: (b) 4 gr in a day/10 days, (d) (e) 400 mg 3 times per day or 600 mg 2 times per day/6 days, 8 sessions for 12 weeks (4 sessions per week for 3 months) cost of 1.2 days of work for themselves because of low back pain (Guo et al., 1999, 35) [16], 14 cost of working days lost due to back pain (estimated, our processing), cost of 30 lost working days due to the chronic low back pain (Katz, 2006, 37) [18], (m) (n) motor activity with HBP, 1 once daily for 40’, to 15 times a month (at home, without the use of specialist), cost of 2 working days lost due to back pain (estimated, our processing), cost of 3 working days lost due to back pain (estimated, our processing), cost of 2 working days lost due to back pain (estimated, our processing), cost of 2 working days lost due to back pain (estimated, our processing).
It was been assumed that the unit cost of the use of HBP (item i – Table 1) is entirely tolerated by the NHS. It has been speculated, based on the expert’s opinion [7, 23], that the cost/patient/30 days.
Therapy, is around € 300.00 (Table 2). This cost can be given to a ticket for the use of a car for home treatment, or for independent use in hospital departments. The charges related to the possible help of a figure of support are free of cost, since the orthosis can also be used in full autonomy [13]. Regarding the indirect costs, in a working day lost, it turns out to be (according to ISTAT data in 2012) related to Gross Domestic Product (GDP) equal to € 23,470.00 – of € 64.325, crucial amount for the determination of benefits in terms of reduced work absence (method of human capital) [1, 24].
In Tables 2, 3 and 4 are shown the results (expenditure for direct and indirect costs, average costs and P1 vs. P2) variation which is reached as a result of simulation conducted in Fig. 1.
Below the detail, with specific reference to the traditional path (P1) and in the alternative (P2) relating to the different types of low back pain (acute, subacute and chronic), identifying for each, the total direct and indirect costs (Fig. 2).
Summary of spending on direct and indirect costs (source: our processing)
Summary of spending on direct and indirect costs (source: our processing)
Average costs and variation P1 vs P2 (source: our processing)
myblueRGB54,95,145 myredRGB204,0,0 mygreRGB118,146,60 myyelRGB255,204,0
Evolution of the direct and indirect costs in the two compared paths (P1 vs P2). Source: our processing.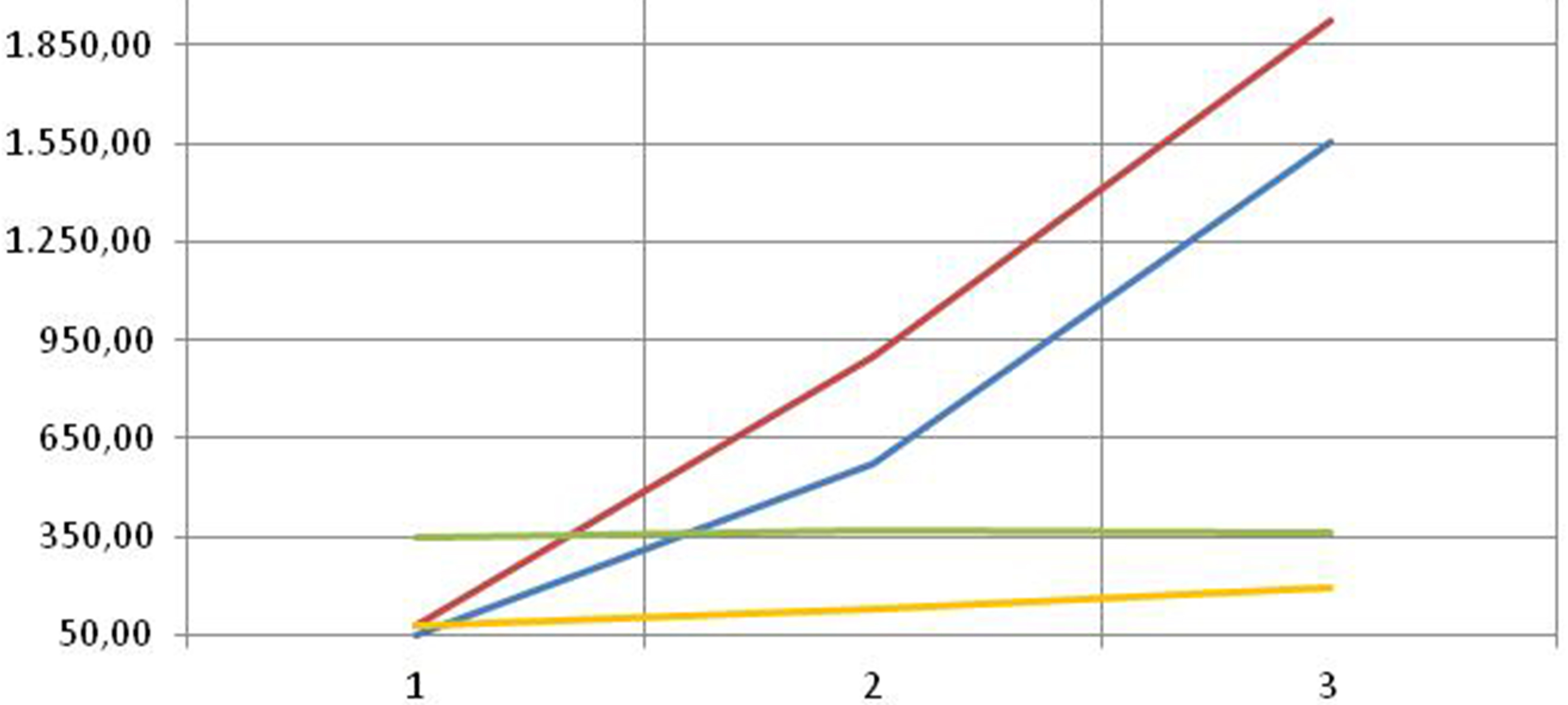
For acute low back pain, the use of the exoskeleton increases the direct costs from € 64.04 (P1) to€ 332.02 (P2) without affecting the indirect ones.
In the treatment of subacute low back pain, however, adding a treatment program with exoskeleton, helps the passage of the direct costs from € 552.48 (P1) to € 347.18 (P2) and indirect ones from€ 900.20 (P1) to € 128.60 (P2).
Finally, in the treatment of chronic low back pain, direct costs increased from € 1526.98 (P1) to€ 340.18 (P2), while indirect ones rose from € 1,929.00 (P1) to € 192.90 (P2).
The synthesis of the framework of what has been reported is shown in Table 3.
On the basis of what has been reported, the use of therapy with HBP, would generate a saving of€ 971.40/year in the case of sub-acute low back pain and amounted to € 2,922.90/year in case of chronic low back pain (Table 4).
The epidemiological impact of low back pain and the chronic character that distinguishes it have a significant economic burden on the NHS and society, in terms of the direct and indirect costs to it attributable [25].
The literature reports episodes of back pain with varying duration(periodic or repeated), high economic and social costs which can be classified into two main components, healthcare and manufacturing loss, mainly caused by the inability of work [26].
According to some authors, it can be attributed to back pain a social cost superior to all other forms of disability, because of the considerable and already mentioned indirect costs [20, 22]. In fact, the time spent in good health for a person can be quantified in terms of increased productivity within the facility where the work takes place. In this perspective, each day of absence from work due to illness are assigned a value corresponding to that of lost production [10]. Similar to the wide etiopathogenesis, the methods of intervention are numerous and different and they can include the pharmacological treatment, the manual approach, the use of electro-medical equipment, etc..
The estimate of the costs for the two different paths described above, highlights the fact that the average cost of treatment for low back pain is higher in the case of use HBP only in comparison with the one in case of the acute low back pain. In both approaches, the average cost of treatment increases with the severity of the disease, with an important trend in case of the traditional route.
The cost reduction, which is sometimes significant, occurs when recourse of HBP, especially in case of chronic low back pain, is linked to the considerable cost (direct) of hospitalization [27]. However, the most significant savings is linked to the indirect costs for a faster return to work and normal daily activities.
The literature highlights the importance of the acute low back pain treatment, within the first few weeks after the occurrence of the events. This can be crucial in the determination of the eventual reappearance of pain or its persistence [28, 29].
According to Mantini et al., 90% of patients with acute low back pain experienced improvements just within 30 days of the incident [27].
Croft prove frequent episodes of relapse in the short to medium period. This puts the emphasis on the need for a first treatment that may improve the diagnosis, and then reduce the occurrence of new episodes and, consequently, reduce the economic impact [30].
In this phase, the HBP adoption appears to be substantial because of its ability to correct postural abnormalities in dynamic way [21].
The studies conducted in the exoskeleton have shown that the HPB is able to modify the postural attitude even with subjects who present only minor asymmetries of the back and that a postural rehabilitation, followed actively by artificial constraints, could represent a complementary solution in the treatment of the most common posture imbalances [21, 31, 32].
Conclusions
In the industrialized countries, the main problems of public and private health systems are the finding and the allocation of resources for prevention and treatment of low back pain [33].
In the future, the phenomenon will become increasingly important for the healthcare decision makers considering the aging of the population, which itself will rise expectations of patients about the rapid development of the available technology [34, 35].
So, the management departments of these kind of companies, have to be in a good relationships with different stakeholders, that are particularly so important to both individual citizens and, regional and central institutions, which itself requires appropriate behavior and that they do respect the economic links and planning, defined by the allocation of resources [36, 37].
This paper provides guidance on the potential benefits, economically speaking, resulting from an innovative therapeutic approach that provides the adoption of the Human Body Posturizer by the NHS [38, 39].
In one hand, this analysis demonstrates the impact of the use of HBP in economy [40]; in the other hand, it has to be considered as a conservative study (i.e. as reported, it does not cover certain types of cost, of difficult feedback: transport, domestic care fee, etc.) [41, 42].
A further studies are needed to determine the complexities and the diversities of the factors involved in the outflow of back pain care programs, they have to be designed to support the health policies, in order to link output and clinical outcomes with economic ones [43, 44].
Footnotes
Acknowledgments
The authors would like to acknowledge the cooperation of the health institutions in giving permissions to conduct the study.
Conflict of interest
None to report.