
Abstract
BACKGROUND:
The orientation of the pelvis is of particular importance to the sagittal curve of the spine and has geometric relationships with the top of the spine and lumbar lordosis. Changes in spinal shape or disruptions of sagittal balance in the spine, such as a flattened lumbar spine, have significant negative effects.
OBJECTIVE:
The aim of this study was to investigate the effects of the posterior superior iliac spine support device (PSD) on upper trunk acceleration during gait in individuals with flat lumbar back posture.
METHODS:
In total, 10 young male subjects with reduced lumbar lordosis (global lumbar lordosis angle (T10–S2):
RESULTS:
The normalized AP acceleration of T7 with PSD (40.57
CONCLUSIONS:
We found that wearing the PSD immediately improved pelvic physiological movement during walking in individuals with lumbar flat back posture. Our findings may help healthcare professionals manage flat back posture in asymptomatic younger individuals.
Keywords
Introduction
Walking is a common daily activity, and the trunk contributes to the active control of whole body movements, providing stable support for the head and the lower extremities for efficient locomotion [1, 2]. Trunk motion in the sagittal plane depends on coordination of the thoracic spine, lumbar spine, and pelvis. The coupling of these regions allows optimal posture as well as energy efficient walking [3, 4]. The successive links in this chain are the spine and the pelvis, and their shape and orientation are important variables in the movement of the sagittal plane. The orientation of the pelvis is of particular importance to the sagittal curve of the spine and has geometric relationships with the top of the spine and lumbar lordosis [5, 6].
Changes in spinal shape or disruptions of sagittal balance in the spine, such as a flattened lumbar spine, have significant negative effects. A reduction in lumbar lordosis causes increased pelvic posterior tilt, resulting in stress on muscles, ligaments, and bones. These stresses can lead to mechanical changes in shear support and coupling motion and can therefore cause compensatory posture and movement in adjacent segments of the vertebral curve during various activities, including walking [7, 8, 9, 10].
In the clinical setting, non-elastic taping is commonly used for effective control of the trunk and pelvis and results in improved neuromuscular facilitation and proprioceptive function [11, 12]. Non-elastic tape can immediately correct the posture of body segments or restrict joint motion, and it provides passive mechanical support that decreases pain [13]. Another widely used method for improving impaired movement due to pain or stiffness is mobilization with movement (MWM). During MWM, a therapist applies sustained gliding manual force while the patient performs an active movement [14, 15]. MWM has been used successfully to manage various musculoskeletal conditions, such as ankle joint limitation, locked lumbar zygapophyseal joint, and chronic pains [15, 16]. However, there is a limit to how consistently alignment of the pelvis can be corrected via the application of tape or sustained manual force. Therefore, we developed a posterior superior iliac spine support device (PSD) that can be easily worn and enables self-mobilization through the physiological movement of the pelvis during walking. The PSD is a type of belt that can be worn by itself and applies force to the pelvis. Furthermore, wearing the PSD while walking leads to a self-mobilization intervention to increase movement of the pelvis during daily activities. Therefore, the purpose of this study was to investigate the effects of the PSD on upper trunk acceleration during gait in individuals with flat lumbar back posture.
Methods
Subjects
In total, 10 young male subjects with reduced lumbar lordosis (global lumbar lordosis angle (T10–S2):
Materials
Global angle measurement
The participants stood in an upright relaxed position, with feet shoulder-width apart, and the examiner measured the global lumbar lordosis angle (T10–S2) [17] using a dual inclinometer (Acumar, Lafayette Instrument Co., Lafayette, IN, USA). We measured three times and used the mean value to select participants (ICCs
Components of PSD. a) Outward, b) Inward, c) Lateral.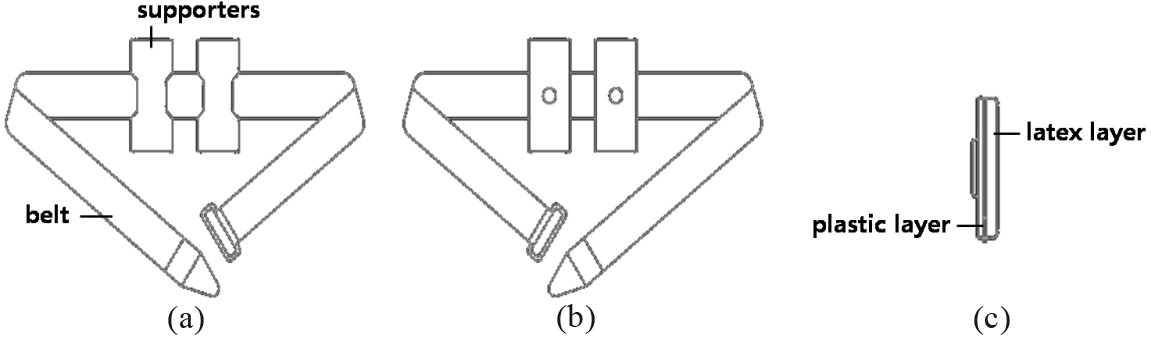
Gait time, energy expenditure, and normalized upper trunk accelerations in each of three directions were measured during gait (sensor range:
PSD
We designed the PSD to apply the principles of MWM to improve pelvic movement in individuals with a flat back posture. The PSD is a type of belt that can be worn by itself and applies force to the pelvis. The PSD consists of two parts. One part is the belt, which is secured with Velcro. The other part provides support and consists of two supporters that are attached to the belt to support the posterior superior iliac spine. The supporters are made of a latex layer (5.2 cm
Procedures
The test was explained to participants in advance. The accelerometer was attached to the participant over the T7 spinous process with double-sided tape. Each participant walks straight for 7 m on a pathway at their self-selected speed with and without a PSD (Fig. 2). To avoid the effects of acceleration and deceleration on measurements, the 2 m at the beginning and end of each trial were excluded. After two practice trials, participants performed three randomly selected measurement trials. Participants rested for 1 minute between trials.
Comparison of normalized T7 acceleration, gait time, and mean energy expenditure during gait with and without a PSD (
10)
Comparison of normalized T7 acceleration, gait time, and mean energy expenditure during gait with and without a PSD (
All values are mean
Wearing a PSD.
All data were analyzed using the SPSS statistical package (version 18.0 for Windows; SPSS, Chicago, IL, USA). Differences in gait time, energy expenditure, and normalized T7 acceleration during walking were analyzed using paired t-tests. Statistical significance was set at
Results
The normalized AP acceleration of T7 with PSD (40.57
Discussion
Our primary finding is that wearing the PSD frequently changed velocity in the AP direction. In this study, we expected to see a self-mobilization effect of wearing the PSD that would increase pelvic anterior physiological movement. The PSD was designed to apply continuous force via the belt and to generate self-mobilization via the motion of walking in individuals with flat back posture. We hoped that this would result in posterior pelvic tilt, an immediate correction of faulty alignment, restricted range of motion, and short-term efficacy in improving the movement of the spine.
Yoon et al. [19] demonstrated that modified MWM using tape made an immediate difference in subjects with limited ankle dorsiflexion. The authors suggest that uphill walking alone is not sufficient to change foot kinematics in individuals with limited ankle dorsiflexion. Because the talus plays a role as an anatomical chain between the hindfoot and the tibia, the modified MWM using tape might have provided a stabilizing force for the talus, altering the posterior inferior glide of the talus during tibia advancement over the fixed foot.
In the present study, we found that the normalized thoracic AP acceleration was higher while using the PSD than while not using it. Walking velocity varies according to the relative locations of the COM, the standing limb, and COM displacement; these changes lead to acceleration of the trunk [3, 4]. Additionally, pelvic movement in the sagittal plane is characterized by short-arc rotations in the AP direction about a ML axis through the hip joint [20]. The pelvis is located between the hip joint and the lumbar spine, and this leads to the coupled lumbo-pelvic and thoracic-pelvic motions. As the pelvis is a relatively rigid structure, walking alone is not likely to be sufficient to change pelvic kinematics in individuals with flat back posture. However, wearing the PSD might have provided a stabilizing force for the anterior glide of the pelvis during walking [21]. In the sagittal plane, modulations of the pelvis allow maintenance of the spinal curves despite changes in other parameters. Thus, we consider our finding of increased normalized thoracic acceleration in the AP direction while wearing the PSD to be important. This result is consistent with the findings of Hu et al. [22], who found that the belt may provide sacroiliac force closure by the transverse and oblique abdominal muscles. This may lead to transfer of contralateral torque to the ipsilateral iliac bone, pelvic rotatory control, and a consequent reduction in the activity of the transverse and oblique abdominal muscles.
In the present study, thoracic acceleration in the vertical direction did not differ between gait task conditions. However, thoracic acceleration in the vertical direction was reduced when wearing the PSD. In the vertical direction, the COM oscillates up and down to follow two full sine waves per gait cycle. The maximum height of the COM occurs at the mid-point of both periods of single limb support (30% and 80% of the gait cycle). The pelvis then begins tilting anteriorly during the period of single limb support, reaching a slight anterior pelvic tilted position at mid-stance (30% of the gait cycle) [20].
In this study, gait time and energy expenditure did not differ between PSD conditions. Meaningful variation in energy consumption was difficult to measure in this study because participants were asymptomatic young men and walked only 3 m. Our study had several limitations. First, our sample size was small, and caution should be exercised when generalizing the results. Second, we did not measure pelvic angle or lumbar acceleration. Third, the effects we investigated were short-term, and our study cannot confirm whether the observed effects will persist in the long-term. Finally, we did not measure or control for the force with which the PSD was applied, although we did ensure that the PSD was always applied by the same investigator with consistent force.
Conclusions
We found that wearing the PSD immediately improved pelvic physiological movement during walking in individuals with lumbar flat back posture. Our findings may help healthcare professionals manage flat back posture in asymptomatic younger individuals.
Footnotes
Acknowledgments
This research was supported by the Leaders in INdustry-university Cooperation Program of the National Research Foundation of Korea (NRF) 2018, and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (No. 2017R1D1A1B03035485).
Conflict of interest
None to report.