
Abstract
BACKGROUND:
Clinicians routinely encounter the endodontically treated teeth with wide flared canals and mineral trioxide aggregate (MTA) repair on the canal wall.
OBJECTIVE:
To assess the effect of customized glass reinforced composite (FRC) post and reshaped root canal along with different acid etching protocol of MTA surface on push-out bond strength (PBS) in flared, MTA repaired root canal.
METHODS:
Ninety recently extracted single-rooted premolar teeth were sequentially subjected to root canal obturation, post space preparation, flaring, and MTA application. The samples were randomly divided into 3 groups of control (no relining or reshaping), customized FRC post by relining with self-adhesive resin cement and reshaping the canal with flowable composite. Each group was subdivided into 3 subgroups (
RESULTS:
Control group had the lowest PBS at 1.988 N. The PBS values for the groups with customized post relining were 8.489 N, 8.888 N and 7.911 N for control, H
CONCLUSIONS:
Customized FRC post with 37% H
Introduction
Effective restoration of endodontically treated teeth (ETT) is a constant challenge to clinicians. ETT restoration is complex due to multiple factors involved, like remaining coronal tooth structure, apical seal, radicular dentin thickness and the deleterious effect of root canal irrigants [1]. The iatrogenic root canal perforations are the main cause of treatment failure and accounted for 18–23% of all failed ETT [2, 3]. Restorative dentist’s pursuit of restoring the ETT with long, wider endodontic post and consequent indiscrete post space preparation may also lead to the root canal perforation. Kvinnsland et al. [4] report 53% of iatrogenic perforations happens during post space preparation, while 47% occur during endodontic therapy. The material of choice for non-surgical management of perforations is bioactive mineral trioxide aggregate (MTA) [5]. The previous researchers document the tissue repair and regeneration potential of MTA in new cementum formation and periodontal regeneration [6]. The additional advantages of MTA are its hydrophilic nature and ability to set in the presence of moisture. ETT with inadequate coronal tooth structure often requires the service of an endodontic post. The previous research suggests most common failures of post retained restoration are tooth fracture, post debonding and fracture of the post [7]. Root canal perforations because of stripping, pathological osteoclastic activity, and overzealous instrumentation often associated with wider flared root canal space. The fiber reinforced composite (FRC) posts are most commonly used in contemporary dental practice due to aesthetic color, easy clinical procedure and its compatible modulus elasticity with dentin [8].
Selecting the FRC post with an appropriate dimension is difficult due to its availability in limited dimensions. The utilization of standard dimension FRC post to restore the flared canal lead to thick luting cement and reduced post bond strength. The reduced bond strength of resin cement is attributed to multiple factors like stress because of polymerization shrinkage, lesser mechanical strength [9], and non-homogenous thickness. Thicker resin cement layers with embedded voids and bubbles also act as a stress concentration location leading to cracks, reduced bonding strength [10]. The improved contact between the post and root canal walls will also reduce the role of bonding potential of luting cement in bonding strength [11].
The mismatch between FRC post and post space is the clinical challenge [12]. The previous researchers suggest the customization of FRC by resin relining [13], alternatively reshaping of the root canal with composite. The self-adhesive resin luting cement is advocated by the researchers over other luting cement due to its higher mechanical property and lesser polymerization shrinkage [14]. The self-adhesive flowable composite is advocated for root canal shaping. Since it requires no pre-conditioning of the substrate surface, reduced the clinical time, procedural errors and less technique sensitive [15].
Presence of MTA layer on the lateral surface of the root canal wall adds to the complexity of the bonding performance of resin luting cement. Kayahan et al. [16] reported acid etching created MTA surface changes that might have the potential to enhance bonding of resinous materials. They observed the acid etching of the MTA surface resulted in the loss of matrix around the crystalline structure. Cervino et al. [17] are of the opinion, water in the MTA could inhibit adhesion due to high hydrophobicity of the resin materials. Samimi et al. [18] reported the etching of MTA surface with phosphoric acid resulted in the removal of crystals and amorphous structures, creating a rough and porous surface that improved adhesion of the resin materials. The EDTA is often utilized as the substitute for phosphoric acid to etch the enamel and dentin [19].
The rehabilitation of the ETT is incomplete without adequate coronal restoration. The esthetic post retained restoration in MTA repaired flared root canals is predicted with the poor prognosis. As clinicians frequently encounter these clinical situations, it is prudent to know the better management protocol for favorable treatment outcome. Hence, authors proposed to explore the combined effect of post space modification with post relining or canal reshaping along with MTA surface treatment on the bonding strength in flared, MTA repaired canals. This in-vitro study was designed to evaluate the effect of different post space modification methods, different MTA surface treatment on push-out bond strength of FRC post. The null hypothesis of the study was that there is no significant difference in PBS among different MTA surface treatment methods.
Materials and methods
The institutional ethical review board approved the study proposal (SRC/ETH/2017-18/084). A total of 90 intact single-rooted premolars with a mean root length of 16
Implanting the teeth sample in acrylic resin with vertical holding machine.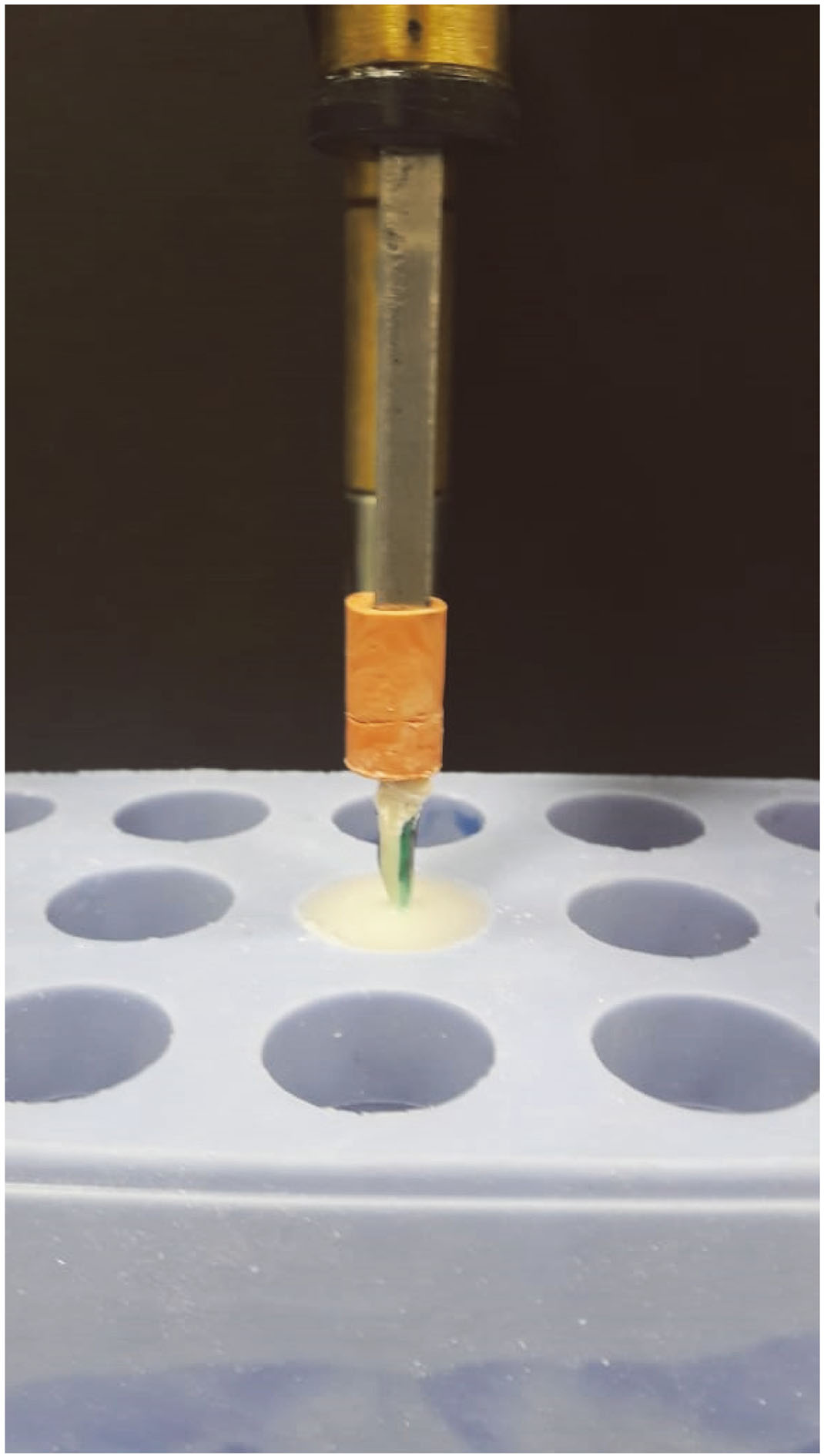
The teeth samples were sectioned at a cementoenamel junction with the help of Double-sided Diamond Discs (Kerr Corporation, Orange, CA, USA) under water coolant. Later they were implanted within acrylic resin vertically with the vertical holding device (Fig. 1). The uniform 10 mm post space length was obtained with sequential use of Gates-glidden, peeso reamers in the low-speed handpiece. Due care was observed to preserve a minimum of 5 mm gutta-percha for an apical seal. The calibrated post drill (Fibrekleer, Pentron clinical, oranage, CA, USA) was mounted in the low-speed handpiece and post space was refined up to 10 mm length. The coronal 7 mm of post space was carefully flared with help of 2.1 mm diameter, 8 mm length tapered diamond bur (856F, Hager & Meisinger GmbH, Neuss, Germany) under copious water irrigation (Fig. 2). The standardized central position for the post was achieved following the techniques described by Egilimez et al. [20]. Since the flaring of the canal was limited up to 8 mm compared to total post space length of 10 mm, the centralized position of the post was maintained during cementation and relining procedures. The post space was irrigated with normal saline and dried with paper points. The Mesio-proximal wall of prepared post space was coated with a thin uniform, freshly mixed MTA (ProRoot MTA, Dentsply Sirona, York, PA, USA) by MTA carrier (MAP system, Dentsply Sirona, York, PA, USA). The application of MTA within the post space was performed under the dental operating microscope (OPMI pico, Carl Zeiss Meditec AG Göschwitzer Jena, Germany).
Graphic depicting the flaring, centralisation of FRC post.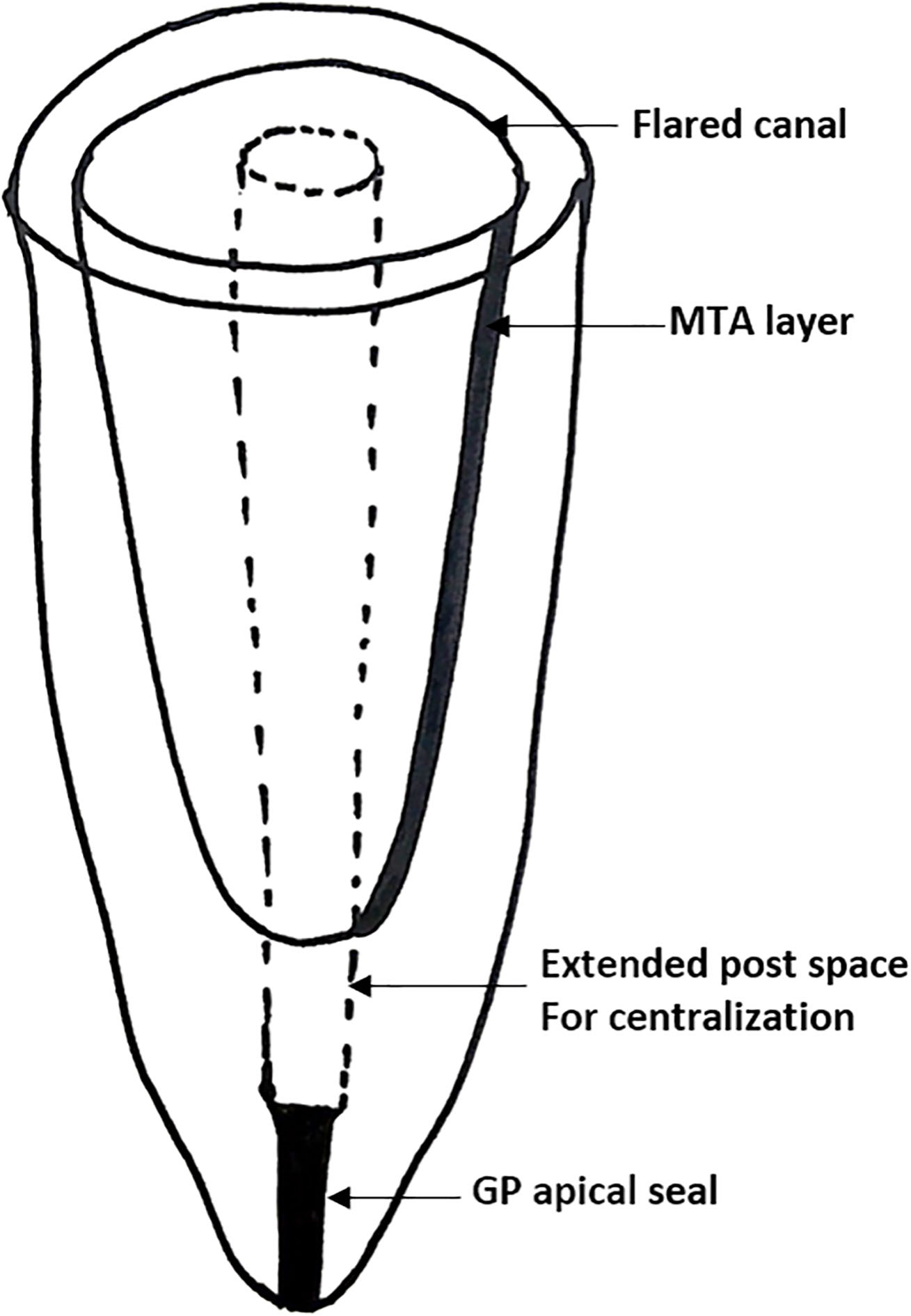
Ninety samples were randomly divided into 3 major groups.
Group I (control group)
Subgroup IA (
Subgroup 1B (
Subgroup IC: No post space modification, MTA surface etching with 19% EDTA (File-Eze, Ultradent Products, Inc., South Jordan, UT, USA) for 60 seconds.
Group II
In these groups, the root canal was reshaped with a flowable composite (Wave, SDI Germany GmbH, Cologne, Germany). The 1.0 mm diameter FRC post was lubricated with glycerine gel and the root canal was filled with flowable composite. The FRC post was placed to a predetermined length (10 mm) inside the root canal. The composite resin was tack cured for 5 seconds using an LED light curing unit. The post was loosened with a rotating movement and removed from the root canal. The reshaped root canal walls with flowable composite were additionally light cured for 20 seconds. MTA surfaces were modified with etching agents according to the group prior to the reshaping of the canal with flowable composite.
Subgroup IIA: Reshaped root canal with flowable composite, no MTA surface modification.
Subgroup IIB: Reshaped root canal, along with MTA surface etching with 37% H3PO4, 20 seconds.
Subgroup IIC: reshaped canal and 19% EDTA etching of MTA surface for 60 seconds.
Group III
The samples in these groups had relined FRC post with a self-adhesive resin luting cement (RelyX
Group IIIA: Relined FRC post with no MTA surface modification.
Group III B: Relined FRC post with MTA surface etching with 37% H3PO4, 20 seconds.
Group IIIC: Relined FRC post, 19% EDTA etching of MTA surface for 60 seconds.
Prior to cementation of FRC post, it was thoroughly cleaned with 75% ethanol. Post space was irrigated with water, gently air dried, and excess moisture was removed with absorbent paper points. The self-adhesive resin luting cement capsule was activated and mixed in amalgamator for 10 seconds. The cement was carried into the canal with the help of root canal tips. The fiber post was placed within the canal, excess cement was removed and light cured for 40 seconds.
Push-out bond strength testing
The samples were subjected to 1500 thermocycling between 5
The bonding area was calculated with the formula of [21]
The
The statistical analysis was performed using the SPSS 19 software (IBM Corporation, Armonk, New York, USA). The data were evaluated by Factorial ANOVA to evaluate MTA surface conditioning and post space modification along with the Tukey comparison test. The level of statistical significance was determined at
Results
Table 1 displays the mean and standard deviation of the push-out bond strength (N) of all the tested groups. The results of the study show the ill-adapted FRC in root canal had poor PBS. The control group with no post space modification and MTA surface treatment had the lowest PBS at 1.988 (0.124) N. The surface etching of MTA with 37% H
Push-out bond strength mean values (N) and standard deviations of tested groups
Push-out bond strength mean values (N) and standard deviations of tested groups
Note: H
Push-out bond testing of samples under universal testing machine.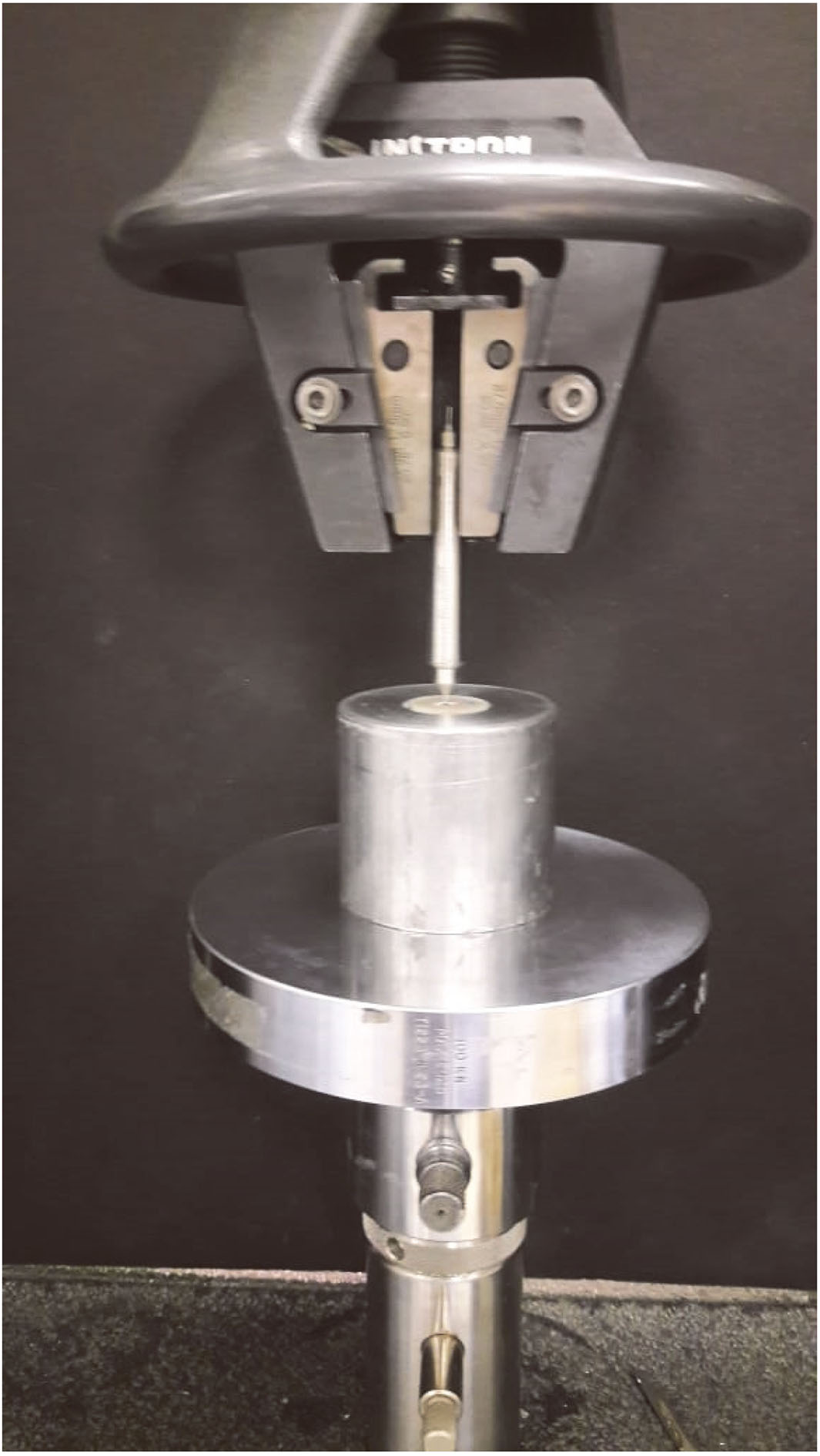
Results of two way ANOVA evaluating the post space modification and MTA surface treatment variation in push-out bonding strength
MS: Mean squares, effect size
Factorial ANOVA (Table 2) was conducted to compare the main effects of post space modification, MTA surface treatment and the interaction effect between the post space modification and MTA surface treatment on the PBS of FRC post. The effect of post space treatment produced an F ratio F (2, 0.025)
The Post Hoc Turkey’s comparison test (Table 3) showed the significant difference between all three groups of control, space modification and surface treatment with
Post hoc comparison using Tukey’s HSD for space modification and surface treatment
SM: Space modification, ST: surface treatment, Control,
Clinicians frequently encounter the ETT with wide, flared root canals repaired with MTA. Often these teeth require the post retained restoration. Adequate coronal restoration is critical not only to restore the function, aesthetics, but it is also essential to prevent coronal leakage. The selection of closely adapted FRC post remains as a challenge for the clinician. This study explores the feasibility of customizing the FRC post to flared canal repaired with MTA. The adequate bonding strength of Post to root canal is decisive for long-term clinical performance of post restored ETT. The push-out bond strength testing was selected in this study since the stress between the cement-radicular dentin and cement-post interfaces are similar to the stress generated during clinical function [22].
The present study results showed the groups with customized FRC post and reshaped canal with higher PBS compared to the control group. The poor PBS could be attributed to the thicker luting cement layer and consequent cohesive failure within the cement layer. Egilmez et al. [20] reported the larger diameter post and thin cement layer significantly improves the bond strength of post. D’Arcangelo et al. [12] described the pull-out resistance of FRC post is decreased in thicker luting cement. Thick luting cement layer potentially weak because of the embedded bubbles or voids. These areas of weakness act as crack initiators and stress concentration areas predisposing for cohesive failures. These internal defects are less likely in thin luting cement layer. Furthermore, the thicker resin luting cement generate higher polymerization shrinkage stress due to a larger volume compared to the thin cement film [23]. The ratio between the bonded and unbonded surface area known as c factors also contribute to the reduced bond strength [24]. Improved adaptation to root canal by customized FRC post improves the bonded area and frictional resistance to post dislodgement [25].
The improved PBS from relined post group could be due to favorable c factor with a smaller volume of resin cement, less polymerization shrinkage and thin, uniform luting cement. Self-adhesive resin luting cement is recommended to reline the FRC post due to high bond strength and lower polymerization shrinkage [26]. The bonding between FRC post and self-adhesive resin cement comprises three adhesive approaches; mechanical interlocking, covalent bonding, and hydrogen bonds [27]. The microporous surface of FRC post allows for additional bond strength through micro retentive effects. Fiber post along with a resin luting cement is reported to create the secondary mono blocks within the root canal. Belli et al. recommend the reduced adhesive interface to create primary mono blocks with the adhesive post-core system; it reduces the stress within tooth structure [28]. The polymerization shrinkage during relining of the FRC post is devoid of stress due to the absence of opposing adhesive interface from the root canal. Previous researchers reported the improved bonding of self-adhesive resin cement with FRC post compared to conventional or self-etch adhesives [29].
The groups comprising reshaped canal with flowable composite revealed the substantially higher PBS comparison to the control group. However, the PBS values were marginally lesser than the relined post groups. Reshaping the canal is a difficult task because of root canal anatomy and poor accessibility. The polymerization shrinkage of flowable composite is higher than conventional composite [30]; consequently, stress may lead to detachment of the bond with radicular dentin. The high C-factor in root canals (expected at 200) may also lead to higher polymerization stress, decreasing the bond strength [31]. The light-activation of the flowable composite in more apical locations of the canal is difficult and jeopardize the effectiveness of a canal reshaping. The finite element method study on the effect of restoration technique on stress distribution in roots with flared canals showed the increased thickness of root canal by composite resin relining lead to less stress on the remaining radicular dentin structure. However, the stress distribution in an anatomic post was more favorable due to the localization of stress inside the post body [32].
Another hypothesis of MTA surface modification with 37% H
The limitation of the study includes the effect of cyclic loading simulating masticatory forces on the bonding strength was not evaluated. Further studies are required to test the effect of long-term storage and cyclic loading on the bonding strength between acid etched MTA surface and resin bonding. The studies are also required to evaluate the effect of these post space modification on stress distribution and fracture resistance of the root canal treated teeth.
Conclusions
Within the limitations of the study it was concluded that during FRC post-restoration of flared, MTA repaired root canal it is advised to reline the post with self-adhesive resin cement to customize the FRC post. The acid etching of the MTA surface with 37 % H
Footnotes
Conflict of interest
None to report.