
Abstract
BACKGROUND:
Up to date there is no intramedullary, biodegradable osteosynthesis commercially available to treat non-comminuted midshaft fractures of small hollow bones applying not only a stable osteosynthesis but an additional axial compression to the fracture site.
OBJECTIVE AND METHODS:
Therefore we (1) designed different implant profiles and simulated the inner tension/volume using CAD. (2) Thereafter we manufactured a prototype with the best volume/tension-ratio using 70:30 poly-(L-lactide-co-D, L-lactide) (PLLA/PDLLA) and poly-
RESULTS:
The 3-point-bending-test-results showed that mean failure-force of PCL-tubes was 57.94
CONCLUSION:
The study showed that the new type of biodegradable, intramedullary tension-osteosynthesis made of PLLA/PDLLA is even more stable than common plate osteosynthesis in a small-hallow-bone-model. Further in vivo investigation should be performed to evaluate the surgical technique and long-term healing process of the bone and biodegradation process of the implant.
Introduction
Diaphyseal long bone fractures are a frequent occurrence in orthopaedic trauma care. Operative treatment of displaced midshaft fractures includes reduction followed by fragment fixation using either extramedullary (em) plates or intramedullary (im) with metallic nails [1]. These procedures generally lead to clinically and radiologically beneficial results, but up to 15% of intramedullary nailing cases and up to 10% of plating procedures result in malunion or non-union. In addition, removal of metal implants is frequently required after fracture healing, causing not only disadvantages for patients, but also tremendous economic burden to the health care system [7].
Previous studies have shown that plate osteosynthesis compromises the biological activity and fracture healing potential by reducing periosteal blood circulation, while offering inferior biomechanical stability compared to intramedullary nailing [5, 6, 2, 14, 15]. Because of its biomechanical advantages and minimally invasive approach, intramedullary nailing is the preferred approach in long bone shaft fractures, demonstrating overall good results [2, 14, 15].
However, intramedullary osteosynthesis in short hollow bones can be comparatively problematic. Grassi et al. reported three refractures, two delayed unions with pin breakage, and two non-unions out of forty uncomplicated mid-clavicular fractures stabilised by intramedullary fixation with a 2.5-mm threaded pin [3]. The observed nailing complications in small hollow bones are likely due to insufficient biomechanical stability and lack of compression at the fracture site as a result of the small diameter of the elastic nail and the lack of interlocking bolts [2, 4, 16].
In addition, subsequent procedures may be needed to remove implants once the fracture has healed [7]. In an effort to avoid additional surgical intervention, biodegradable polyglycolide rods have been developed for intramedullary stabilisation of metacarpal and finger shaft fractures, demonstrating satisfactory results [8]. Some drawbacks of these implants include a lack of longitudinal compression tension through wiring and the negative effects of implant degradation, such as inflammatory reaction [9]. Other biodegradable raw materials for implant production, such as polylactide, degrade very slowly (up to three years or more) and adverse reactions are virtually unobserved [4, 9].
The aim of the current study was to develop a new type of slow-degrading intramedullary implant that would achieve biomechanically stable fixation of non-comminuted midshaft fractures of small hollow bones through additional axial compression [6]. We present the CAD-development and prototype production process of an implant for metacarpal osteosynthesis, as well as the results of biomechanical testing in comparison with commonly used alternatives.
Materials and methods
Implant design
We aimed to produce a new implant design consisting of one tube, two anchors and one suture. A priori, we set the minimum volume requirements of the tube at 5.0 mm of outer diameter (OD), 2.0 mm of inner diameter (ID) and 30 mm in length, enabling suture wires to pass longitudinally through the centre of the tube. We conducted simulated tests of ten possible implant designs using computer-aided design (CAD) software (CATIA V5 R19; Dassault Systèmes, France). The various implant designs were chosen for their feasibility for injection molding and clinical aspects (gearing, implant ability) in order to select the implant design with the best ratio between maximal biomechanical stability and minimal volume, so as to minimize the amount of cleavage products during implant degradation. Bending stress was simulated using implant models with different cross sections and loaded with a 15 mm-lever-arm applying a force of 50 N (Fig. 1).
Correlation between volume and tension of different tube cross sections (CAD evaluation).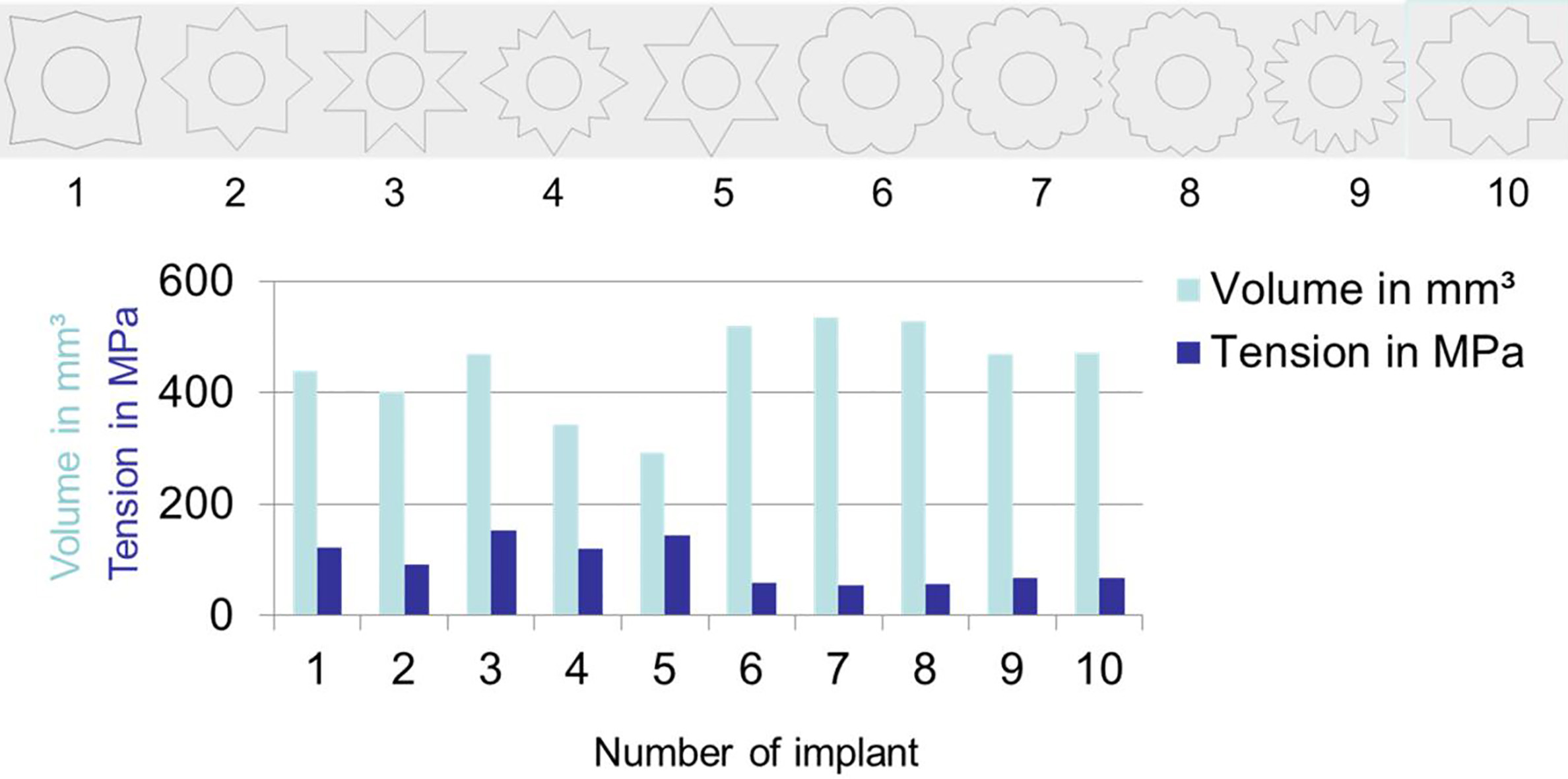
The shape of the anchors was designed similar to a slightly curved shirt button with four perforations of 1.0 mm in height and 6.0 mm in diameter designed for suture wire fixation. Once the design was finalized, tubes and anchors were manufactured using two different biodegradable raw materials: (1) 70:30 poly-(L-lactide-co-D, L-lactide) (PLLA/PDLLA) (Resomer
The functional concept of the new implant is demonstrated in Fig. 2. The intramedullary tube (T), which expands symmetrically over the fracture site, avoids fracture bending and shearing of the hollow bone parts. The outer diameter of the tube should be chosen slightly smaller than the diameter of the intramedullary canal of the fractured hollow bone to facilitate tube insertion. Then, monocortical holes must be drilled at approximately 20 mm from the fracture site and the suture (S) has to be inserted into first hole through the tube and diverted out of the second hole. Positioning of the tube can be achieved by simple intramedullary insertion. Once the tube is positioned, the suture can be tensioned between the anchors (A1 and A2), which are fixed at both fracture ends. The tensioned suture runs longitudinally through the tube leading to a compression of the fracture ends.
Functional concept of the new osteosynthesis-technic shown by schematic visualisation.
Three types of biomechanical tests were conducted: (1) a failure load test of the anchor; (2) a 3-point bending resistance test of the tube; and (3) a 4-point bending test of the tube compared to commercially available osteosynthesis plates.
Failure loads of the anchors were tested on prototypes made of PLLA/PDLLA (
For the 3-point bending test, 30-mm tubes made of PLLA/PDLLA (
For the 4-point bending test and comparison of the new biodegradable implants with commercially available plates, three different types of Ti6Al4V 6-hole plates (Stryker GmbH & Co. KG, Duisburg, Germany) designed for osteosynthesis of metacarpal bones were used: (1) Profyle hand 2.3-mm 6-hole standard plate; (2) Profyle hand 2.3-mm 6-hole compression plate; and (3) VariAx
According to the 4-point bending test protocol [13], the osteosynthesised synthetic bones were symmetrically positioned on two rollers supporting the sample (distance: 60 mm) at both ends at the bottom of the universal testing machine. By the use of both load rollers (distance: 20 mm) pressing with a speed of 1 mm/min downwards in perpendicular direction to the longitudinal axis, the osteosynthesised bone was loaded at midpoint until either a bending deformation of
Statistical analysis
Descriptive data are presented as mean values accompanied by standard deviation. To compare continuous variables between the different treatment groups the unpaired
Results
Implant design
Cross section no. 10 was chosen for prototype production since (1) best ratio between stability and volume (bending stress 67.3 MPa, tube volume 472 mm
Biomechanical evaluation
All failure load tests of the anchors ended with the breakage of the bar between the two perforations of the button where the tension wire was fixed. PCL anchors had a lower mean failure force (35.77
All 3-point bending tests of the prototype tube implants ended with failure by deformation
Mean failure force of 2.3-mm standard plates was 18.84
The failure force 4-point-bending-test-setup of the im-biodegradable osteosynthesis showed for PCL-tubes a mean failure value of 22.27
The statistical analysis revealed no significant difference between the bending rigidity of osteosynthesised bones stabilised with the biodegradable PCL-tube-system and 2.3 mm-locking-plate in contrast to the other plate-types (
Discussion
In this study testing the design and biomechanical properties of a new biodegradable implant for treating midshaft fractures of small hollow bones, we found that a tubular implant with an eight-jagged cog wheel cross section and button shaped anchor made of PLLA/PDLLA demonstrated superior biomechanical fracture fixation stability compared to other commonly used osteosynthesis plates.
Considering the drawbacks of currently available implants for fixing fractures of small hollow bones, the newly developed biodegradable implant could help improve fracture fixation biomechanics and the biological aspects of bone healing, while reducing risks for the patient and economic burden on the health care system by avoiding a second procedure for implant removal.
The proposed implant addresses some of the current shortcomings in several ways. Having an outer diameter equal to or slightly smaller than the diameter of the hollow bone’s intramedullary canal prevents shearing and bending forces from dislocating the reduced bone fragments. In addition, the tensioned suture attached at both bone ends leads to tube-guided compression of the fracture site that not only improves the stability of the osteosynthesis, but also ameliorates the biological healing process of the fracture itself. The positive effect of contact compression is well documented in numerous studies on acute bone fractures and in the treatment of non-union [6, 14, 17, 18]. It should be noted that the new implant is not designed for osteosynthesis of comminuted fractures, but for transverse and oblique midshaft fractures (approximately
Metal implants like Ti6Al4V plates must frequently be removed after fracture healing [7]. In contrast, biodegradable implants will resorb after fracture healing, avoiding not only a second operation to remove the implant, saving costs and risks for the patient as well as avoiding stress shielding effects observed by the use of rigid metal implants in bone surgery [4, 7]. In the event of a refracture or septic material removal, the implant can be easily removed via the fracture zone. In the case of septic material removal when fracture healing is complete, any non-absorbable parts can be easily removed. Aside from several studies using intramedullary metal nails or wires for small hollow bone fracture fixation, very few authors have reported on the application of biodegradable rods in hand and foot surgery, primarily for arthrodesis [1, 19, 20]. Nearly 20 years ago, Kumta et al. used absorbable polyglycolide intramedullary implants for hand fractures [8]. However, polyglycolides degrade quickly within 6 months of implantation and 40% of the patients presented with adverse reactions like local inflammation of the surrounding tissue, as well as foreign body reactions in the draining lymph nodes or osteolysis [21, 22, 23]. In contrast, when using slow-degrading materials like polylactides, similar findings are observed only sporadically [4, 24, 25]. Additionally, the risk of undesired tissue-reactions can be minimised by a small implant volume [4, 26].
To address these concerns, the new intramedullary implant presented in this study was produced using materials enabling a very slow degradation. PLLA/PDLLA in a ratio of 70:30 results in more than 18 months of degradation time and PCL results in an even longer degradation period of more than 24 month [4, 27, 28]. Both biodegradable materials have been already used without disadvantages in different medical applications with no evidence of osteolysis [25, 28]. Furthermore, an ideal tube cross section was identified by CAD simulation to provide not only sufficient stability with a minimum implant volume (see Fig. 1) [4, 22, 26].
To the best of our knowledge, there are no data available directly comparing PCL and PLLA/PDLLA as biodegradable materials for the type of implant described in this study (one composed of a tube and anchors). Therefore, we decided to test implants manufactured from both materials. Although the main advantage of PCL is the slow degradation and consequently low accumulation rate of dissolved products, the biomechanical results between both materials showed significant differences in all configurations. Not only the tension tests of the anchors, but also the three-point-bending tests of the tubes revealed a significant superiority of the implants made out of PLLA/PDLLA compared to those made out of PCL. None of the tubes broke during the tests, but deformation of PCL tubes started at an earlier stage of bending.
The osteosynthesis tests performed after stabilising the artificial bone with one of three different plate types or with intramedullary PCL or PLLA/PDLLA implants demonstrated the biomechanical superiority of the PLLA/PDLLA system. Although the use of a more elastic implant material might facilitate the intraoperative procedure of intramedullary tube insertion and prevent stress shielding effects at the contact zones between implant and bone, the measured weakness of PCL implants could lead to a collapse of the construction and non-healing. Moreover, it is known that stress shielding effects are minimized and corrosion is avoided by the use of implants made of biodegradable materials compared to metal implants, potentially improving long-term results [29, 30].
The biomechanical osteosynthesis tests showed superiority of intramedullary PLLA/PDLLA implants compared to plate-constructions. 2.3-mm Ti6Al4V plates are especially designed for small bones and are used in numerous types of trauma cases [31, 32]. Subtracting the 2 mm internal diameter from the 5 mm outer diameter, the 3 mm net diameter of the biodegradable tube is only slightly thicker than the plates and even thinner at the bottom of the valley between two jags. The comparison of intramedullary and extramedullary procedures is valid as both techniques are tested in the same configuration using a synthetic composite bone and under identical mechanical settings.
There are several limitations to this study. First, in contrast to clinical situations with soft-tissue covering the bone, ideal implant positioning was achieved. Second, implant behaviour may differ in clinical situations (e.g. osteoporosis) compared to artificial bones. Third, the effect of cyclic and rotational loading wasn’t examined in this study. Since Bio-ISOS achieves a compression of the fracture, there is interlocking of the fracture fragments, which should minimize the impact of rotational loading on the implant. Furthermore, the healing process with osteogenesis will improve fragment interlocking. Fourth, the healing process using a long-term in vivo trial wasn’t investigated in this study, but should be the subject of future research.
Conclusion
In summary, a new tubular biodegradable implant with an eight-jagged cog wheel cross section and button shaped anchor made of PLLA/PDLLA demonstrated superior biomechanical fracture fixation stability compared to other commonly used osteosynthesis plates. The clinical use of this new type of implant could reduce the need for a second operation for implant removal after fracture healing and reduce the financial burden on the patient and on the health care system.
Footnotes
Acknowledgments
The project was funded by the Ministry of Science and Education, license number 01EZ0830.
Conflict of interest
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.